Download to read offline


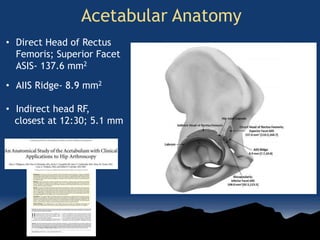
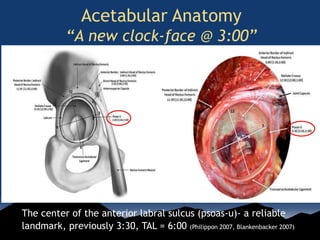
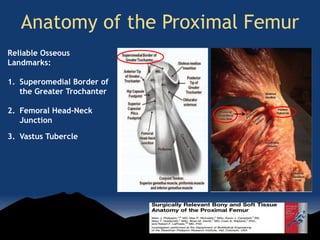
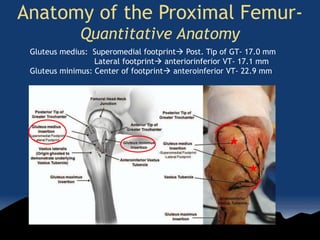
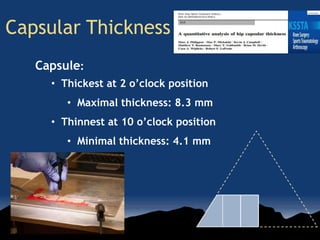
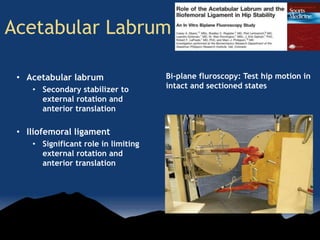
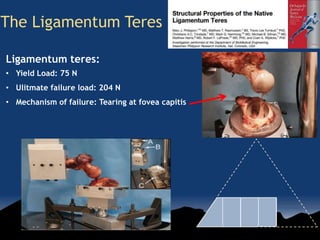
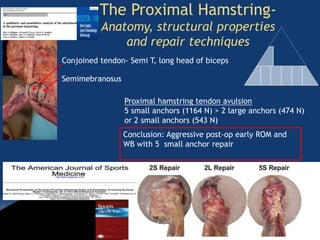


This document summarizes a presentation on bioengineering research of the hip. It discusses how quantitative anatomical research has improved understanding of hip structures like the acetabulum, proximal femur, capsular thickness, labrum, ligamentum teres, and proximal hamstrings. Biomechanical studies investigate injury patterns and validate surgical reconstruction/repair techniques. Future research directions include robotic studies of the hip. The conclusion is that anatomical and biomechanical hip research is growing and will lead to improved surgical techniques and patient outcomes.


































































