Systemic lupus erythematosus
•Download as PPTX, PDF•
1 like•190 views

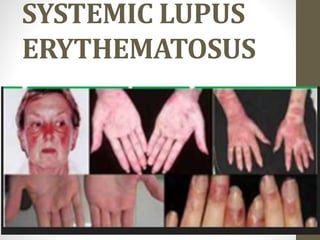
Systemic lupus erythematosus (SLE) is an autoimmune disease. In this disease, the immune system of the body mistakenly attacks healthy tissue. It can affect the skin, joints, kidneys, brain, and other organs

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Systemic lupus erythematosus
Similar to Systemic lupus erythematosus (20)
Recently uploaded
Recently uploaded (20)
Systemic lupus erythematosus
- 2. INTRODUCTION • Systemic lupus erythematosus (SLE) is a systemic multisystem • autoimmune disease characterized by the presence • of autoantibodies and multiorgan system involvement.
- 3. HISTORICAL REVIEW - Medical literature described the dermatitis of SLE as early as the 13th century. The butterfly rash was recognized in 1845, and in 1852 the term lupus erythemateux was coined. - Osler described the clinical features, and in 1924 Libman and Sacks reported the characteristic endocarditis. In 1948 Hargroves and colleagues described the lupus erythematosus (LE) cell and one year later cortisone was first used. In 1957 the association of a positive ANA and SLE was made.
- 4. SLE IN CHILDREN • Accounts for ~15% of all lupus patients. • More common in girls than boys. • More common in Asian-, African-American, and Hispanic than white American children. • Rare in children under 5; more common in adolescents. • May have more severe disease at onset and a more aggressive course than in adults.
- 5. PRESENTATION OF SLE IN CHILDREN • Common initial presentations: – Unexplained fevers or prolonged general illness without explanation – Swollen lymph nodes – Changes in blood counts: • Low platelets • Low white blood cells • Anemia – Rashes, skin changes, or ulcers • Classic malar “butterfly” rash is only seen in up to ½ of patients. • Discoid rashes are relatively rare, but are more likely to progress to systemic disease. – Joint pain, swelling, or stiffness • Often in the hands and wrists but can affect other joints too.
- 6. PRESENTATION OF SLE IN CHILDREN • Other initial presentations: • Kidney disease • Though occurs in up to 80% of patients eventually. • Neurologic symptoms • Seizures, psychosis, movement problems, etc. • Some neurologic symptoms occur in up to 20 or 30% of pts, usually within the first year. • Blood clots • Antiphospholipid antibodies are relatively common. • Other • Heart disease • Lung disease • Organ enlargement
- 7. DIAGNOSIS • Similar to clinical criteria used in adults. Most patients can be diagnosed by history, exam, and lab testing. • Not uncommon to have “partial” presentations in children, with unclear initial diagnoses. These may progress over time. • Younger age at diagnosis (esp. before puberty) may imply more severe disease and worse prognosis.
- 10. LAB TESTS Lab tests: • Proteinuria, hematuria, other urine abnormalities • Low white blood cells, low platelets, hemolytic anemia •Positive ANA •Positive anti-Smith or anti-dsDNA •Anti-Ro, anti-La, anti-RNP, anti-histone •Coombs test •Low complements •Elevated inflammatory markers
- 11. OTHER FINDINGS • Depends on the presenting features. • Leukemia, lymphoma, or other malignancy • Infections • Juvenile arthritis • Can present with polyarticular joint symptoms. Many children with juvenile arthritis have a positive ANA. • Organ-specific autoimmunity • Thyroid disease • Idiopathic thrombocytopenia (low platelets) • Many other possibilities depending on presentation
- 12. CAUSES OF SLE • Genetics affect risk – Children with close relatives who have lupus are at higher risk, but no genetic test predicts disease perfectly. Risk increases with more affected relatives. • Environmental exposures • Medications: – Minocycline (an antibiotic often used for acne in adolescents) is a well-known cause of positive ANA and lupus-like syndromes. Symptoms often resolve after discontinuation. – Antiseizure medications, antihypertensive (blood-pressure), and several other medications can have similar effects, though are less commonly used in children and teens. – Stimulants prescribed for ADHD can cause Raynaud’s phenomenon or can make it worse.
- 13. TREATMENT OF SLE • Generally similar to that of adults. – Many patients require corticosteroids (e.g. prednisone or SoluMedrol) to control symptoms, especially early. – Mild lupus • Often responds to hydroxychloroquine (Plaquenil). • May benefit from NSAIDs (ibuprofen, naproxen, etc.) for musculoskeletal symptoms. – Moderate lupus • May require the addition of azathioprine (Imuran) or mycophenolate (CellCept). These are often used for hematologic or renal involvement of the disease. – Severe lupus • May be treated with cyclophosphamide (Cytoxan) or sometimes rituximab (Rituxan), for involvement of the central nervous system or for severe kidney or hematologic disease.
- 14. CONSIDERATIONS OF SLE • May be approached more aggressively. • Corticosteroids in children • (prednisone, prednisolone, Medrol, SoluMedrol) – Growth effects – Body image • Cyclophosphamide – Fertility? Cancer risks? • Rituximab – Future immune function, vaccine effectiveness • Other medication issues
- 15. Transition to adulthood • Often very challenging. – Adolescents are “invincible.” – Change of primary care physician and specialists. – Change of physical location (for college or job). – Change of insurance coverage. – Balancing adult responsibilities with demands of managing a chronic illness. – Family changes, relationships, and pregnancy.
- 17. THANK YOU