
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Vestibular Schwannoma
Similar to Vestibular Schwannoma (20)
More from Oussama Alserwy
Recently uploaded
Recently uploaded (20)
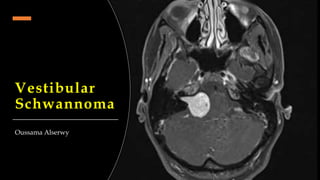
Vestibular Schwannoma
- 2. Overview • Composed of Schwann cells and involve the vestibular rather than the acoustic division of the 8th cranial nerve. • Benign and usually slowly growing. • Arises in the IAC can reach up to the CPA compressing the brain stem. Here, complications start. • Incidence is increasing and approaches 20 per million/yr.
- 3. Predisposing Factors 1. Congenital de novo from a mutation and usually associated with (NF2) 2. Acquired due to ionizing radiation, exposure to extremely loud noise at work, female hormones and mobile phone use of at least 10 years’ duration.
- 4. Tumour Size • Only the extracanalicular portion of the tumor should be measured. • Tumors limited to the IAC should be reported as "intracanalicular tumors.“ • Axial CT or MRI is used to estimate tumor size.
- 5. Presenting symptoms • Unilateral hearing loss and tinnitus, followed by vertigo, dizziness, or unstable gait. • Later symptoms include those due to facial and trigeminal nerve compression (.e.g diminished corneal reflex). • The time from initial symptoms to tumour diagnosis varied from 1 month to 20 years.
- 6. Investigation • PTA showing ‘Roll over phenomenon’. • Confirm by MRI.
- 7. Management Goal: completeness of tumor resection along with preservation of facial nerve function and hearing. Conservative
- 8. Microsurgery • Consider the risk-benefit ratio. • Large or cystic tumors that require decompression of the brain stem. • Risk profile including facial nerve palsy, dizziness, stroke, death and late tumour regrowth. • Noting that the recurrence rate is considerably higher in large tumors. • Preservation of the facial and trigeminal nerves is attempted for all patients in fear of the combined cosmetic and functional problems to the patients. Considerations
- 9. 3 surgical approaches to the CPA have been proposed; retrosigmoid (traditional), translabyrinthine, and middle fossa (rare) Retrosigmoid (Suboccipital) Translabyrinthine Advantages • Possibility of hearing preservation. • Any size of tumour can be removed. • Excellent view, allowing early identification and preservation of nerves. • Any size of tumour can be removed. • No cerebellar retraction is required. Disadvantages • Cerebellar retraction and the increased incidence of chronic post-craniectomy headache. • Loss of any residual hearing. • loss of the ipsilateral peripheral balance function.
- 11. Stereotactic Radiosurgery ‘Gamma Knife’ • Consider the risk-benefit ratio. • Control of smaller tumors, by increases in tumor diameter from tumor capsule expansion associated with central tumor death . • Control of larger tumours will need more radiation dose that will carry a huge side effects on the adjacent vital tissues. • Noting that the recurrence rate is considerably low. • Preservation of the facial nerve & hearing is the best comparing microsurgery. Considerations
- 13. Microsurgery Gamma Surgery Advantages • Any size of tumour can be removed. • No need to general anesthesia. • Short recovery time. • Possibility of preserving any residual hearing. • Very low risk profile than surgery. Disadvantages • Need of general anesthesia. • Longer recovery time. • High risk profile. • Inability to treat large lesions.