2. The accidental or involuntary loss of:
1. Urine from the bladder (urinary incontinence) or
2. Bowel motion, faeces or wind from the bowel (faecal or anal
incontinence).
1. Definition of Incontinence
3. 2. Incidence of Bladder and Bowel Problems in Monash
• Incontinence is a condition that ranges in severity from 'just a small
leak' to complete loss of bladder or bowel control.
• In fact, over 4.8 million Australians have bladder or
bowel control problems for a variety of reasons.
• Approximately 37,241 residents in Monash suffer with
incontinence.
• Incontinence can be treated and managed.
• In many cases evidence based research states that:
it can also be cured.
4. • Urinary incontinence affects up
to 13% of Australian men & up to
37% of Australian women.
Facts & Figures
• Faecal incontinence affects up toFaecal incontinence affects up to
20% of Australian men & up to20% of Australian men & up to
12.9% of Australian women.12.9% of Australian women.
5. • 65% of women & 30% of men waiting
to see a GP report some type of
urinary incontinence, yet only 31%
seek professional help.
Facts & Figures cont.
• Faecal incontinence is one of the three
major causes (along with decreased
mobility & dementia) for admittance
to a residential aged care facility..
6. Women comprise over 70% of people
affected by incontinence due to:
pregnancy
younger women who have had children
menopause
obesity
Coughing bouts
Constipation & straining
specific types of surgery such as
prostatectomy and hysterectomy
Causes:
7. Causes cont..
reduced mobilityreduced mobility
neurological and musculoskeletal conditionsneurological and musculoskeletal conditions
such as multiple sclerosis and arthritissuch as multiple sclerosis and arthritis
health conditions such as diabetes, stroke,health conditions such as diabetes, stroke,
heart conditions, respiratory conditions, andheart conditions, respiratory conditions, and
prostate problems.prostate problems.
Risk factors for faecal incontinenceRisk factors for faecal incontinence
Urinary incontinenceUrinary incontinence
Tearing of the perineum during childbirthTearing of the perineum during childbirth
chronic diarrhoea,chronic diarrhoea,
Straining and constipation.Straining and constipation.
10. FALLEN BLADDER
->-> urinary tract infections
->-> pelvic dragging or heaviness
->-> Incomplete bladder emptying
Examples of Prolapse- a.
11. B. FALLEN VAGINA
->-> Pelvic dragging or heaviness
->-> sensation of a vaginal lump or
bulge.
->-> discomfort & skin irritation
Examples of Prolapse- b.
12. Fallen bowel
->-> worse with straining and
completely emptying bowels
->-> causes pelvic dragging,
heaviness and discomfort
Examples of Prolapse- c.
14. • empties 4-8 times each day (every 3-4 hours);
• can hold up to 400-600ml of urine (the
sensation of needing to empty occurs at 200-
300 ml);
• may wake you up once at night to pass urine
and twice if you are older (i.e. over 65 years
of age);
A Normal Bladder:
15. • tells you when it is, full but gives you enough
time to find a toilet;
• empties completely each time you pass urine;
and
• does not leak urine.
A Normal Bladder cont.:
16. • The bowel is a tube-like organ part of the digestive tract
• It begins in the stomach and ends at the anus.
• It consists of the small intestine ( where nutrients from the food are
digested and taken into the body – the remainder forms waste
(‘poo’)and travels to the large intestine.
• Faeces enter the large bowel as liquid.The large bowel absorbs
water back into the body and the faeces become more solid.
• When faeces reach the lower part of the large bowel (rectum), you
you feel fullness or the urge to pass a bowel motion.
Bowels
17. • Approximately 5 % of people experience poor bowel control.
• Poor bowel control occurs in both males and females
• It's more common as you get older, but young people can also have
poor bowel control.
• Younger women who have had perineal tears (obstetric anal
sphincter injuries) suffer with “faecal incontinence”.
• Often, people with poor bowel control also have
poor bladder control and may leak urine.
Bowels cont..
18. Stress incontinence :
is the leaking of small
amounts of urine when there is
increased pressure inside the
abdomen that pushes down on the
bladder.
Commonly associated with:
coughing, sneezing, laughing,
walking, lifting, or playing sport.This
occurs mainly in women and
sometimes in men (most often as a
result of prostate surgery).
Types of Incontinence a.
19. -is a sudden and strong need to
urinate.
It is often associated with
frequency (the need to frequently
pass urine) and nocturia (waking
several times at night to pass
urine).
Some people with urge
incontinence get little or no
warning and wet themselves
before they get to a toilet.
Urge continence is often due to
having an over-active or unstable
bladder.
Urge incontinence:
20. Faecal Incontinence
•Occurs when people experience difficulty controlling their bowels. As a
result they pass faeces or stools & at the wrong time or in the wrong
place.
•Staining of underwear or an excessive passage of wind (anal
incontinence) without control may also be a problem.
•May occur as a result of an obstetric anal sphincter injury –
3rd
or 4th
degree perineal tear.
•Faecal incontinence affects up to 20% of Australian men and up to
12.9% of Australian women (Australian Instiute of Health andWelfare,
2006).
Types of Incontinence b.
21. Pelvic floor muscle training should be offered as first line
of therapy to all women with stress , urge or mixed
urinary incontinence. (Level 1a evidence 3rd
international
consultation on Incont. Abraam 2005).
An observational study at the university of South
Australia has shown physiotherapy has proved effective
for more than ~80 % of women who received pelvic floor
muscle training by a trained continence physiotherapist.
The cure rate was 64 %.
Studies & Evidence- a.
22. 1. Intensive Pelvic Floor Rehabilitation cures 56-84% people suffering from
stress, urge or mixed incontinence.(Beet et al 1999,Wong et al 1997,
Neuman et al 2008).
2. (Bo K 2009 )”Does pelvic floor muscle training (PFMT) prevent and
treat urinary and fecal incontinence in pregnancy?”
Found that intensive PFMT was effective in treating ante and postnatal
women with urinary and faecal incontinence particularly those suffering
with post partum incontinence.
3. (MorkvedS et al 2007) “Does Pelvic Floor MuscleTraining with Follow Up
Instructions by a Physiotherapist Reduce Urinary Incontinence after Radical
Prostatectomy? A Randomised ControlTrial” - found that conservative
management for post prostatectomy urinary incontinence with intensive
and supervised pelvic floor muscle training has been proven to show a
clinically relevant difference at 6 months and 12 months both clinically and
statistically.
Studies & Evidence- b.
23. Weak pelvic floor muscles
Constipation and straining
Perineal tears, forceps
deliveries, episiotomies
Excessive coughing,
Menopause
Obesity
Asthma or lung disease
What AggravatesThe Problem?
24. Leaking bladder-Which worsens with
having more children & ageing.
Reverting to a lifetime use of pads
The need for surgery– costly &
painful .
Consequences Of Not Doing
Anything??
25. Anxiety ++++
Increased Embarassment
Poor quality of life
Social isolation in elderly
Falls in elderly relating to not getting to
the toilet in time or going often at
night
Institutionalisation- ie entering aInstitutionalisation- ie entering a
nursing homenursing home
Consequences Of Not Doing
Anything??
26. 3. Education on how
to empty bladder and
bowel effectively to
alleviate dragging pain
in pelvis.
4. Electrical
stimulation of the
nerve supply to the
pelvic floor muscles.
ie neuromodulation
1. Intensive, individualised ,
& progressive pelvic floor
muscle training.
2. Bladder retraining
3. Dietary advice in
relation to fibre intake,
weight loss, and fluid
consumption
Cure/ Solution
We offer a money back guarantee if you have not improved after
5-8 treatment sessions within 2-4 months time (conditions apply)
27. 1. Observe the image of the water droplet.
2. I would like you to imagine your pelvic
floor muscles at the base of your pelvis
relaxing similarly to when you are
urinating.
3. Try breathing in and out feeling them relax
as you breathe out.
4. Now I would like you to reverse the film of
this image, on your breath out- imagine
the ripples coming in towards the centre
-squeeze and lift your pelvic floor muscles
(from the back to the front)- up & in
towards your diaphragm.
5. Hold for up to 3 secs and rest.
6. Now try to hold this for up to 20 secs.
Practical
28. Make mention you have attended this seminar when booking an initial
appointment and you will receive:
a FREE individualized pelvic floor strength
training regime (RRP $70)
A FREE recommended action plan (R4L )
addressing your particular concerns/ goals /fears
(RRP $30)
A FREE report about how to remedy incontinence
(RRP $250)
$30 off your Initial Pelvic Floor Assessment
Total = $380 added value.
Special Offer :
Editor's Notes
Why only 31% seek help–
You may be thinking to yourself this is you & are too embarassed to see anyone about it and think this is a normal process of ageing.
IF this is you I want to reassure you that I’ve treated hundred’s of women with this problem & eased their anxieties frustrations, and cured them from this. Treating them in a private confidential setting.
Pregnancy- esp. vaginal and delivering >3.5kg heavy children (both pre- and post-natal women)
Menopause- due to low oestrogen and thining of bladder lining
UTI’s common amidst women with bladder prolapse
Prostatectomy- (removal of all or part of the prostate)
Hysterectomy- Removal of all or part of the uterus and vagina
& getting to the toilet in time.
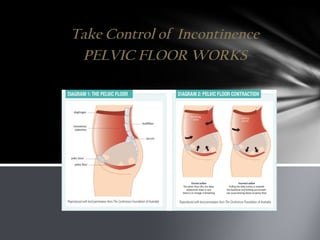
1. by closing the bladder neck, vaginal & anal outlet during a contraction to maintain continence.
3. : bladder, vagina, uterus, and bowel.
5. to promote lumbar stability and help ease lower back pain.
Weak pelvic floor muscles/ post natal tears with childbirth, being overweight and constipation causes this heaviness and bulging or dragging sensation.
This is not a normal or comfortable feeling and research has proven how effective PFMT can help.
The bladder is a storage organ that sits in your pelvis. Urine is made by your kidneys and stored in the bladder until you are ready to empty it. When you go to the toilet your bladder outlet muscles (urethral sphincter and pelvic floor) relax and your bladder contracts (squeezes) emptying your bladder of urine. Your brain controls your bladder by sending messages to tell it when to hold on and when to empty.
How many times or trips do you make to the toilet? Does it affect your sleep & increase your fatigue?
If you are feeling this ie if you have to stand and feel as though u need to go again, it could mean that you haven’t emptied your bladder completely and have a fallen bladder (prolapse) & possibly have a number of UTI’s– you need education on how to empty it completely and strengthen your PFM’s
If you cough
Why worry?
-- can worsen, lead to surgical correction, pain with coitus, and can be quite costly robotic surgery can cost up to ~$5,000- $7,000
-- As women approach menopause- no oestrogen and lining of bladder neck and bladder thins and hence incontinence worsens.
Why worry?
-- can worsen, lead to surgical correction, pain with coitus, and can be quite costly ~$3,000- $3,500
-- As women approach menopause- no oestrogen and lining of bladder neck and bladder thins and hence incontinence worsens.
-- As women approach menopause- no oestrogen and lining of bladder neck and bladder thins and hence incontinence worsens.
--prolapse develops or gets worse
-- may lead to surgical correction & post surgical complications: pain with coitus, & costly ~$3,000- $3,500
-- If left alone– can lead to reduced mobilityobesity falls and institutionalisation ie nursing home