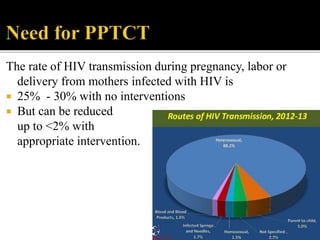
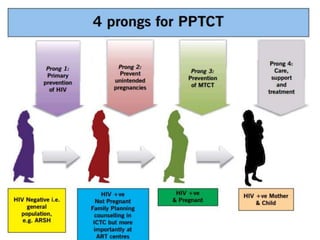
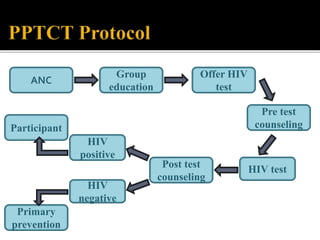
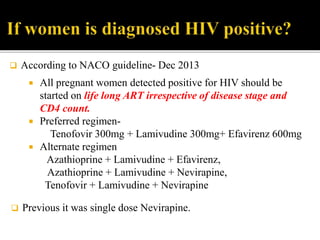
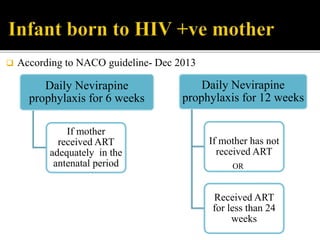
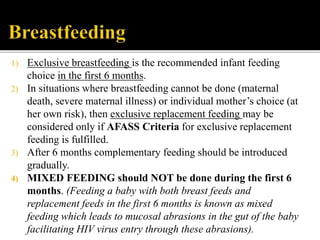
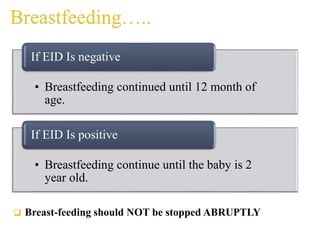
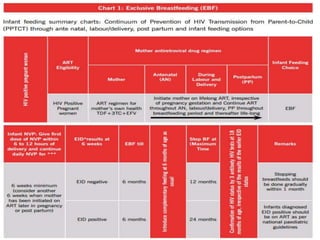
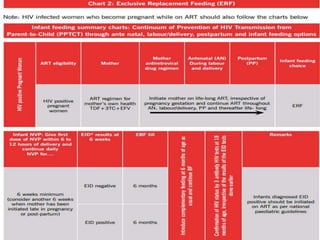
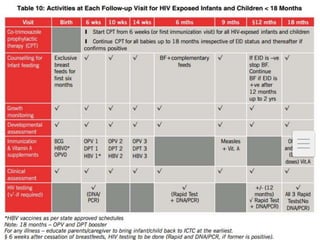
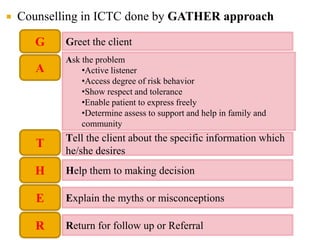
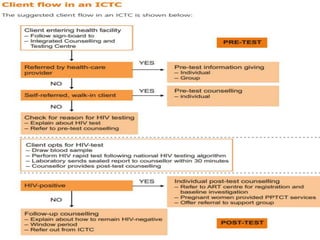
This document summarizes India's HIV epidemic and prevention strategies. It notes that India has the third largest HIV epidemic globally, with approximately 2.5 million people living with HIV. The National AIDS Control Organization aims to reduce new HIV infections by 50% through the current NACP-IV program. It then discusses strategies for preventing mother-to-child transmission, including antiretroviral treatment protocols for HIV-positive pregnant women and breastfeeding guidelines. Finally, it outlines the role and functions of Integrated Counselling and Testing Centres in detecting HIV early and linking those infected to care.



























![Adult immunization [BANGLADESH]](https://cdn.slidesharecdn.com/ss_thumbnails/adultimmunization-160520135511-thumbnail.jpg?width=640&height=640&fit=bounds)







































