Diagnostic dilemma in tachycardiomyopathy - PCICS 2018
•
0 likes•77 views

Ectopic atrial tachycardia (EAT) is one of the most common forms of persistent supraventricular tachycardia in children. • EAT is due to increased automaticity of a non-sinus atrial focus, and when leIt untreated can cause tachycardia-induced cardiomyopathy, also known as tachycardiomyopathy (TCMP). • EAT can be difficult to distinguish from sinus tachycardia depending on the location of the ectopic focus.
Recommended

Recommended
More Related Content
What's hot
What's hot (19)
Similar to Diagnostic dilemma in tachycardiomyopathy - PCICS 2018
Similar to Diagnostic dilemma in tachycardiomyopathy - PCICS 2018 (20)
More from Texas Children's Hospital
More from Texas Children's Hospital (19)
Recently uploaded
Recently uploaded (20)
Diagnostic dilemma in tachycardiomyopathy - PCICS 2018
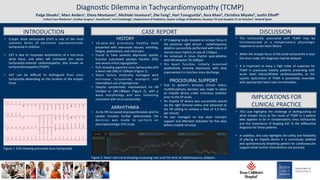
- 1. Page 1 Diagnos(c Dilemma in Tachycardiomyopathy (TCMP) Paige Sheaks1, Marc Anders1, Elena Montanes2, Michiaki Imamura3, Zhe Fang4, Hari Tunuguntla5, Asra Khan5, ChrisDna Miyake5, JusDn Elhoff1 CriDcal Care Medicine1, Cardiac Surgery3, Anesthesia4, and Cardiology5, Department of Pediatrics, Baylor College of Medicine, Houston TX and Hospital 12 de Octubre2, Madrid Spain INTRODUCTION CASE REPORT DISCUSSION • Ectopic atrial tachycardia (EAT) is one of the most common forms of persistent supraventricular tachycardia in children. • EAT is due to increased automa(city of a non-sinus atrial focus, and when leI untreated can cause tachycardia-induced cardiomyopathy, also known as tachycardiomyopathy (TCMP). • EAT can be difficult to dis(nguish from sinus tachycardia depending on the loca(on of the ectopic focus. HISTORY • 16-year-old previously healthy male presented with new-onset nausea, vomi(ng, fa(gue, palpita(ons, and chest pain. • Found to have severely depressed systolic func(on (calculated ejec(on frac(on 22%) and severe mitral regurgita(on. • ECG revealing apparent sinus tachycardia with a heart rate (HR) of 120bpm (Figure 1). • Heart failure medically managed with milrinone, furosemide, enalapril, and intermiWent use of epinephrine. • Despite symptoma(c improvement his HR trended to 180-190bpm (Figure 2), with p wave morphology and axis remaining consistent with sinus tachycardia. ARRHYTHMIA • As his HR increased dispropor(onately and his cardiac func(on further deteriorated, the decision was made to perform an electrophysiologic (EP) study. • EP mapping study revealed an ectopic focus in the posterior right atrium - radiofrequency abla(on successfully performed with return of normal sinus rhythm at rate of 110bpm. • He remained in sinus rhythm post-abla(on with HR between 70-100bpm • His heart func(on ini(ally remained qualita(vely severely depressed, with slow improvement in func(on since discharge. PROCEDURAL SUPPORT • Due to pa(ent’s tenuous clinical status, mul(disciplinary decision was made to place an Impella device under conscious seda(on prior to the EP study. • An Impella CP device was successfully placed via the right femoral artery and advanced to the P8 se_ng to achieve a flow of 3.3 liters per minute. • He was managed on low dose inotropic support and aIerload reduc(on for five days before Impella removal. • The tachycardia associated with TCMP may be misinterpreted as a compensatory physiologic response to acute heart failure. • When the ectopic focus of the atrial tachycardia is near the sinus node, the diagnosis may be delayed. • It is important to keep a high index of suspicion for TCMP in previously healthy pa(ents presen(ng with acute heart failure/dilated cardiomyopathy, as the systolic dysfunc(on of TCMP is poten(ally reversible with appropriate heart rate normaliza(on. IMPLICATIONS FOR CLINICAL PRACTICE • This case highlights the challenge of dis(nguishing an atrial ectopic focus as the cause of TCMP in a pa(ent who appears to be in compensatory sinus tachycardia and the importance of keeping EAT in the differen(al diagnosis for these pa(ents. • In addi(on, this case highlights the u(lity and feasibility of placing an Impella device in a consciously sedated and spontaneously breathing pa(ent for cardiovascular support while further interven(ons are pursued. Figure 1. ECG showing presumed sinus tachycardia. Figure 2. Heart rate trend showing increasing rate un(l the (me of radiofrequency abla(on.