1.ACHD-ASD-VSD.ppt
•Download as PPT, PDF•
0 likes•75 views

Cardiac notes for B.Sc Nurisng students..BY Jayesh Soni Sir

Recommended
More Related Content
What's hot
What's hot (20)
Similar to 1.ACHD-ASD-VSD.ppt
Similar to 1.ACHD-ASD-VSD.ppt (20)
More from Jayesh
More from Jayesh (16)
Recently uploaded
Recently uploaded (20)
1.ACHD-ASD-VSD.ppt
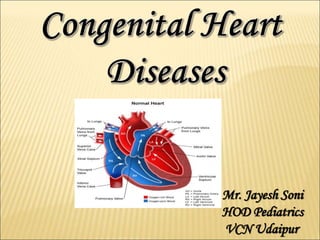
- 1. Mr. Jayesh Soni HOD Pediatrics VCN Udaipur
- 2. 1. Umbilical arteries :- umbilical ligament (2 to 3 months) 2. Umbilical vein :- ligamentum teres 3. Ductus venosus :- ligamentum venosum 4. Ductus arteriousus :- ligamentum arteriosum (1- 3 months) 5. Foramen ovale :- functional closure soon after birth but anatomical closure occurs in about 1 year time (fossaovalis)
- 5. INCIDENCE:- Approximately 8 to 12 childern in 1000 are born with a congenital heart defect. Heart defects are among the most common birth defect and are the leading cause of birth defect-related deaths. Right sided lesions are more common in female, & left sided in males
- 6. ETIOLOGY:- 90 % of cases is unknown. Heredity Consanguinous marriage Chromosomal abnormality – Trisomy 21(Down syndrome), - Turner syndrome Other associated factors - Teratogenic infections (Rubella) - Teratogenic drug (thalidomide) - Alcohol intake - Radiation in 1st trimester of pregnancy - Maternal IDDM - High altitude - Fetal hypoxia - Birth asphyxia
- 7. CLASSIFICATION OF CHD :- Obstruction of blood from ventricles Increased pulmonary blood flow •Aortic stenosis •Coarctation of aorta •Pulmonary stenosis •ASD •VSD •PDA •AVC DEFECT Acyanoti c
- 8. CLASSIFICATION OF CHD :- Mixed blood flow Decreased pulmonary blood flow • TGA • Total anomalous pulmonary venous return • Truncus arterious • Hypoplastic left heart syndrome •TOF •TA Cyanotic
- 10. ACYANOTIC HEART DISEASES If there is no abnormal communication between pulmonary & systematic circulation Or If such connection is present, the pressure forces the blood from arterial to venous side. The blood supplies in the body is therefore oxygenated & caynosis does not occurs.
- 12. ASD: Atrial Septal defects are abnormal opening in wall separating the right & left atria …. More common in females, approx 17% of all cases in congenital cardiac defects..
- 13. TYPES :- 1. Ostium primum - opening at lower end of septum 2. Ostium secundum - opening at centre of septum 3. Sinus venosus - opening at top of septum
- 15. PATHOPHYSIOLOGY:- Shunting b/w Lt to Rt Volume overload in Rt side Rt heart enlargement Overload on pulmonary vasculature Pulmonary HTN RVF
- 16. CLINICAL MANIFESTATIONS • Frequent chest infection • Effort intolerance • dyspnoea • Bulging of chest • Congestive heart failure • Cardiac enlargement
- 17. DIAGNOSIS • Physical examination: systolic murmur • Chest x ray: RA & RV hypertrophy • Echocardiography • ECG
- 18. MANAGEMENT :- Medical management • Treatment of chest infection & infective endocarditis • Interventional therapy - Percutaneous ASD closure Surgical management • Mostly by simple suture closure • In larger defects pericardial or prosthetic patch
- 21. NURSING MANAGEMENT :- Closely monitor vital signs, central venous and intra-arterial pressures, and intake and output. Watch for atrial arrhythmias. Give an antibiotic and an analgesic, as ordered. Provide range-of-motion exercises and coughing and deep-breathing exercises.
- 22. COMPLICATIONS • Pulmonary hypertension • Heart failure • Atrial fibrillation • Stroke from embolization • Eisenmenger syndrome (reversal of the shunt into a right-to-left shunt) • Infective endocarditis • Surgical complication
- 23. VENTRICULAR SEPTAL DEFECT Accounts for 25 %of all congenital heart lesions. Also called Roger’s disease Interventricular septal defect
- 24. Types of VSD:- 1. Membranous VSD 2. Muscular VSD
- 25. PATHOPHYSIOLOGY :- Shunting of blood from Lt to Rt Rv to pulmonary artery Volume overload in the Rt side Pulmonary HTN Eisenmenger’s syndrome and hypertrophy of muscle
- 26. SIGNS & SYMPTOMS :- Palpitation Frequent chest infection Feeding difficulties Tachycardia Excessive sweating associated with feeding Poor weight gain Failure to thrive Biventricular hypertrophy Congestive heart failure
- 27. DIAGNOSTIC EVALUATION •Auscultation of heart sounds – harsh systolic murmur sound. •Chest X-ray :- enlargement of heart. •ECG = biventricular hypertrophy. •2-D-echocardiogram with colour Doppler study.
- 28. MANAGEMENT OF VSD:- • SMALL VSD - all close spontaneously * 50% by 2yrs * 90% by 6yrs * 100% during school yrs Surgical intervention is usually not necessary
- 29. • MODERATE TO LARGE VSDs :- 1. Medical Management: a. CHF management: digoxin and diuretics b. Avoid oxygen; oxygen is a potent pulmonary vasodilator and will increase blood flow into the PA. c. Increase caloric intake 2. Cardiac catheterization for placement of a ventricular occlusion device for muscular defects
- 30. INDICATIONS for SURGERY • Basic Indications for surgical closure – Mid-large shunt – Failure to thrive – Continued CHF or – Recurrent pulmonary infections • SURGERY:- (Usually repaired before age 1) a. One-stage approach: preferred surgical plan; patch closure of VSD (an oval patch of knitted dacron by mattress suture posteriorly). b. Two-stage approach: first surgery is to band the PA to restrict pulmonary blood flow; second surgery is to patch close the VSD and remove the PA band.
- 31. Surgical correction has to be done before irreversible damage to pulmonary vasculature occurs.
- 33. COMPLICATIONS • Congestive cardiac failure • Infective endocarditis on rt.ventricular side • Complete heart block • Delayed growth & development in infancy • Damage to electrical conduction system during surgery (causing arrythmias) • Pulmonary hypertension • Eisenmenger's syndrome.
Editor's Notes
- CHEST RADIOGRAPHY - normal - biventricular hypertrophy - pulmonary plethora