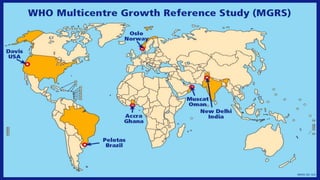
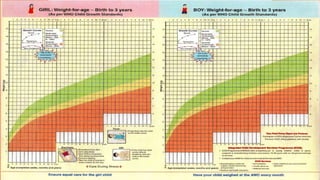
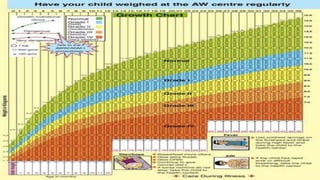
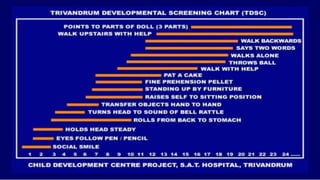
The document discusses growth charts and child development scales. It provides background on the WHO growth chart, including that it was developed based on data from healthy breastfed children in diverse settings. The MGRS from 1997-2003 aimed to establish new growth curves. The WHO charts use 2nd and 98th percentiles to identify abnormal growth. In India, the WHO growth chart was incorporated into the "Mother and Child Protection Card" in 2009. The Trivandrum Developmental Screening Chart is also discussed as a tool to screen motor, mental, hearing and visual development in children under 2 years.