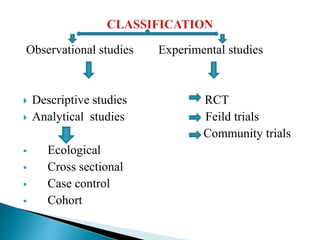
The document provides an overview of epidemiology. It begins with definitions and history, then covers components, aims, principles, classifications, and descriptive epidemiology. Procedures discussed include defining the population and disease, describing disease distribution by time, place and person, measurement, and formulating hypotheses. Descriptive studies are meant to observe disease distribution and identify associated characteristics rather than test hypotheses. The document outlines types of descriptive studies and how epidemiology can describe disease occurrence and distribution.


































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
