Coa pathophysiology
•Download as PPTX, PDF•
0 likes•291 views

PATHOPHYSIOLOGY OF COARCTATION OF AORTA

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Coa pathophysiology
Similar to Coa pathophysiology (20)
More from India CTVS
More from India CTVS (20)
Recently uploaded
Recently uploaded (20)
Coa pathophysiology
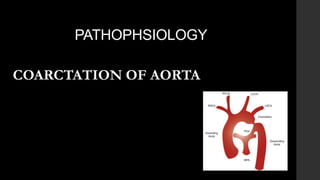
- 2. NOMENCLATURE coarctatis (Latin)- Contracted, tightened or pressed together. The first description of this condition is attributed to Johann Freidrich Meckel, a Prussian anatomist who demonstrated the case of an 18-year-old female in 1750 CONGENITAL NARROWING OF UPPER DESCENDING THORACIC AORTA ADJACENT TO SITE OF ATTACHMENT OF DUCTUS ARTERIOSUS
- 3. 4 6 Thoracic coarctation is a manifestation of abnormal development of the embryologic left fourth and sixth aortic arches
- 4. FLOW THEORY DUCTUS SLING THEORY THEORIES
- 5. FLOW THEORY • In the normal fetus the aortic isthmus receives only 10% of the combined ventricular output, which explains that the normal neonatal isthmus diameter is only about 70% to 80% of the diameter of the ascending aorta. • Decreased blood flow in the aortic isthmus in the embryonic period • Due to reduced perfusion, the isthmus region cannot develop properly and remains hypoplastic. In such cases there is often not only localized coarctation, but also tubular hypoplasia of the aortic arch proximal to the isthmus. • Intracardiac lesions diminish the volume of left ventricular outflow promote development of coarctation in the fetus by reducing flow through the aortic isthmus “NO FLOW, NO GROW”!
- 6. DUCTUS SLING THEORY In 1855, Skoda speculated that the constriction of the aorta is related to the closure of the ductus arteriosus extending into the walls of the aorta,a proposal which is referred to as the Skodiac hypothesis Coarctation develops as the result of migration of ductal smooth muscle cells into the periductal aorta, with subsequent constriction and narrowing of the aortic lumen.This concept is concordant with the clinical observations that coarctation often becomes manifest after ductus closure and that it may be palliated in the newborn with prostaglandin E1 infusion.
- 7. OTHER FACTORS • GENETIC TURNERS SYNDROME 22q DELETION • NEURAL CREST CELLS -Believed to play role in pathogenesis of juxtaductal aorta
- 8. CLASSIFICATION •EDWARDs(Preductal,Post ductal,Juxtaductal) •AMATO et al I - Primary CoA II- CoA with isthmic hypoplasia III- CoA with tubular hypoplasia •BONNET(Infantile & Adult) •Surgical classification: I - Isolated CoA II - CoA with VSD III - CoA with complex intra-cardiac anomaly
- 9. In the infantile group, the ductus arteriosus is open and there is a tubular narrowing of the isthmus of the aorta proximal to the ductus. The ductus supplies the blood flow to the descending aorta In the adult type of coarctation the ductus is closed and there is a shelf-like narrowing within the lumen of the aorta
- 10. PREDUCTAL TYPE 1. PDA is patent and large and provide blood flow to lower extremity. 2. Tubular narrowing of isthmus 3. No shelf like narrowing in aorta. 4. Minimal post stenotic dilatation of aorta. 5. Minor enlargement of intercostal arteries. POSTDUCTAL TYPE 1. The ductus is closed and no longer acts as a shunt. 2. No narrowing of isthmus. 3. Shelf like narrowing with in the aorta in juxtaductal position. 4. Post stenotic and prestenotic aorta is dilated. 5. Intercostal arteries are grossly dilated. The key difference between these two types is the patent ductus arteriosus provides blood flow to the lower extremity in the preductal (infantile) group and the ductus arteriosus is closed in the postductal (adult) coarctation
- 11. MORPHOLOGY Most commonly is a discrete stenosis The most common site is at the junction of the aortic isthmus, the arterial duct or ligament, and the descending aorta
- 12. • C/s area reduced by at least 50%. • An intimal and medial malformation and a prominent posterior infolding (the posterior shelf) which often extends around the entire circumference of the aorta . In the majority of cases, the shelf is formed by ductal tissue • Histologic examination reveals thick intimal and medial ridges that protrude posteriorly and laterally into the aortic lumen Usually intimal hypertrophy ( intimal veil ) extends the shelf circumferentially and further narrows the
- 13. TUBULAR HYPOPLASIA / PREDUCTAL/ INFANTILE COARCTATION - INVOLVES ISTHMUS & DISTAL ARCH - PRESENT IN INFANCY - INTRACARDIAC LESIONS COMMON
- 14. Common association • Uncommon • VSD • AORTIC STENOSIS/AORTIC ATRESIA. • MS/MR • VSD WITH LVOTO • TOF • CONGENITAL PULMONARY STENOSIS • PULMONARY ATRESIA • TRICUSPID ATRESIA • RT AORTIC ARCH
- 15. Associated pathology 1. Collateral Formation 2.. Aneurysm formation of intercostal arteries 3. Aortic valve * bicuspid (27-45%) * stenosis 4. Intracranial aneurysm * berry type intracranial aneurysm 5. Associated cardiac anomaly * 85% of neonates presenting COA
- 16. COLLATERAL CIRCULATION Collateral arteries bypass the obstruction and augment perfusion to the lower body.Although rarely present in infants, collateral circulation gradually develops throughout childhood in those with subcritical coarctation Between aorta proximal to and distal to coarctation. More developed in adult or postductal type as ductus is closed and collaterals are the only source of blood supply to the lower half of body. Inflow primarily from branches of the subclavian artery Outflow primarily into upper DTA.
- 17. Site Inflow Outflow Lateral chest wall 1. 3rd to 6th ant. I/C art. from IMA (First two ant I/C art do not participate) 2. Lat. Thoracic art. From 2nd part of Axillary art 3. I/C br. from musculophrenic art. 1. Ant. Br of 3rd to 9th post. I/C art 2. Arteria Aberrans Around the Scapula 1. Transverse cervical & transverse scapular art from thyrocervical trunk of subclavian art 2. Suprascapular art from Subclavian art 3. Subscapular art from 3rd part of Axillary art 1. Muscular br from post div of 3rd to 7th post I/C art Diaphragm 1. Musculophrenic art from IMA 1. Inf phrenic art from Abd Aorta 2. Lower post I/C art (ant div) Upper abdominal wall 1. Sup epigastric art (terminal br of IMA) 1. Inf epigastric art (br of EIA) 2. Ant div of upper lumbar art Around the spinal cord 1. Ant spinal art from vertebral art 2. Post spinal art from Post inf cerebellar art or vertebral art 1. Radicular art from post div of post I/C and lumbar art Collateral flow predominantly arise from: 1. Subclavian artery and its branches: Internal thoracic artery , intercostal artery, scapular artery, cervical artery, vertebral artery, spinal artery. 2. Epigastric artery.
- 18. Pseudocoarctation • It is a rare condition presumably resulting from the congenital elongation of the aortic arch . • The elongation leads to redundancy and kinking of the aorta which may appear similar to the coarctation but has no actual obstruction to the blood flow. (Absence of narrowing of Aortic lumen) • There is no actual pressure gradient in pseudocoarctation. • There is tendency of dilatation and aneurysm formation due to the turbulant flow in aorta.
- 19. PATHOPHYSIOLOGY • Upper body HTN, systolic gradient across CoA • When obstruction develops rapidly • ventricle fails to take up increased afterload • lv failure • increased LAP & PV congestion • increased shunting across foramen ovale and hypoperfusion of distal organs • acidosis, oliguria, gut ischemia, cold clammy extremities.
- 20. • If ductus closes gradually allows time for LVH and collateral formation. • If ductus is wide open RV output provides lower body perfusion.
- 21. Natural History • Incidence 50: 1lakh live births. Common in males. • 5-7% of congenital heart disease • 80% of these are isolated CoA ± PDA • Natural history of untreated isolated CoA 1st month:10% - acute CHF 1st year: 20% - CHF 1-4 yrs: 10% - chronic CHF • Thus 50% die within 10 yrs of life • 14-20yrs of age: 20% will die d/t Bacterial endocarditis, aortic rupture or intracranial hemorrhage • 20-50 yrs of age: 20% d/t heart failure secondary to HT or valvular heart disease
- 22. • MC causes of death -heart failure(26%) - infective endocarditis(25%) - aortic rupture(21%) -intracranial haemorrhage(13%)
- 23. CLINICAL FEATURES • NEONATES AND INFANTS • CHILDHOOD • ADULTS
- 24. NEONATES AND INFANTS • When coarctation presents in infancy, it often presents as a catastrophic illness. • Congestive heart failure and shock can occur suddenly as the ductus arteriosus closes. • A large proportion of these infants have coarctation with important associated structural lesions such as a ventricular septal defect or aortic stenosis. • In an infant with severe coarctation and a large ventricular septal defect, the sudden onset of ventricular dysfunction, low cardiac output, shock, and acidosis classically develops around 8 to 10 days of life. • Multiorgan system failure, particularly renal failure and/or necrotizing enterocolitis, and death occur rapidly unless definitive medical and surgical interventions are provided rapidly
- 25. NEONATES AND INFANTS SYMPTOMS OF CONGESTIVE HEART FAILURE FAST BREATHING POOR FEEDING BREATHELESSNESS SWEATING FAILURE TO THRIVE COLLAPSE
- 26. NEONATES AND INFANTS • TACHYPNOEA • INTERCOSTAL RECESSION • PROFOUND SKIN MOTTLING • SLOW CAPILLARY REFILL • PERPHERAL CYANOSIS • ABSENT /WEAK FEMORAL PULSES • OVERACTIVE PRECORDIUM The presence of palpable femoral pulses in the first day or two of life does not exclude the diagnosis of coarctation or interruption, since flow of blood to the lower body may be maintained antegradely through the persistently patent arterial duct. Once symptoms occur, the femoral pulses are usually weaker, or absent
- 27. BEYOND INFANCY • Childhood—Usually asymtomatic, Hypertention • Adolescence & adult life-- --Asymtomatic --reduced femoral pulse --murmur, hypertention --Headache,epitaxis,claudication --rarely with CCF, dissection,intracranial hemorrhage
- 28. BEYOND INFANCY • CVA – 2nd – 3rd decade • IE / Endarteritis – 2nd – 4th decade • Rupture / Dissection – 3rd – 4th decade • HT & CAD
- 29. General Examination • Normal • Broad chest and narrow leg • Left arm may be smaller than right • Impaired growth in infants with CHF • Turner’s syndrome (XO)
- 30. CVS examination •Pulse • Brachio-femoral delay Left radial pulse weak – LSCA stenosis Right radial pulse weak – aberrant RSCA
- 31. Blood pressure Systolic blood pressure gradient Difference b/w UL & LL BP > 20mmHg On echo- gradient across CoA– 20mmHg On cath withdrawl gradient > 20mmHg The gradient will increase with exercise. Hypertension
- 32. • The combination of weak or absent femoral pulses together with a gradient in pressure between the limbs is therefore virtually pathognomonic of aortic coarctation.
- 33. Differential cyanosis • (PDA with Right to Left shunt) Ductal-dependent perfusion of the lower half of the body results in differential cyanosis. If there is critical aortic coarctation, the lower half of the body is supplied with venous blood via a right-to-left shunt at the ductal level. A relevant difference in pulse oximetry exists between the right arm (preductal) and the legs (postductal). Left ventricular pressure and volume overload may produce a prominent, heaving ventricular impulse at the apex.
- 34. Auscultation • S1 Normal • S2 Normal • S3 LVF • S4 severe HT . A constant systolic ejection click may be heard at the apex, signaling the presence of a bicuspid aortic valve
- 35. Murmurs 1. Systolic 2. (A grade 2–3/6 systolic ejection murmur originating from the coarctation itself is usually best heard at the base and the left interscapular area posteriorly.If the coarctation is severe, the systolic murmur may be long and spill into diastole) 3. Collateral – 4. Continuous murmurs ,delayed onset crescendo- decrescendo in ant thorax, right infraclavicular, left sternal and suprasternal. 5. Associated intracardiac lesions create other murmurs. Functional – ESM of BAV PSM at the lower left sternal border or apex.–VSD/MR • MDM at the apex-MS
- 36. Thank you
Editor's Notes
- The aortic arches are formed sequentially within the pharyngeal arches and initially appear symmetrical on both sides of the embryo,[1]but then undergo a significant remodelling to form the final asymmetrical structure of the great arteries Each primitive aorta consists of a ventral and a dorsal segment that are continuous through the first aortic arch. The two ventral aortae fuse to form the aortic sac. The dorsal aortae fuse to form the midline descending aorta. Six paired aortic arches, the so-called branchial arch arteries, develop between the ventral and dorsal aortae. In addition, the dorsal aorta gives off several intersegmental arteries The aortic sac is the endothelial lined dilation just distal to the truncus arteriosus; it is the primordial vascular channel from which the aortic arches arise.