Megaloblasticanemia
•Download as PPT, PDF•
5 likes•2,119 views

Under graduate Lecture for Megaloblastic anaemia Definition, Pathophisiology ,clinical feature and lab Diagnosis

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Megaloblasticanemia
Similar to Megaloblasticanemia (20)
More from Ibrahim khidir ibrahim osman
More from Ibrahim khidir ibrahim osman (20)
Recently uploaded
Recently uploaded (20)
Megaloblasticanemia
- 2. Concept An anemia in which there is a predominant number of megaloblasstic erthyroblasts, and relatively few normoblasts, among the hyperplastic erythroid cells in bone marrow
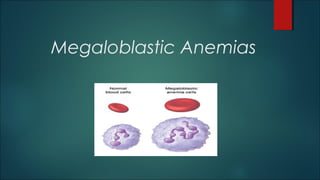
- 3. Megaloblastic Anemia Megaloblastic anemia is an anemia (of macrocytic classification) that results from inhibition of DNA synthesis during red blood cell production. When DNA synthesis is impaired, the cell cycle cannot progress from the G2 growth stage to the mitosis (M) stage. This leads to continuing cell growth without division, which presents as macrocytosis. Megaloblastic anemia has a rather slow onset, especially when compared to that of other anemias anemia or pancytopenia caused by impaired DNA synthesis commonly due to deficiency of vitamin B12 or folic acid
- 6. Etiology 95 % of cases due to: VIT B12 deficiency Folic Acid Deficiency 5% of cases due to: Ant metabolic Drugs Inborn error of metabolism
- 7. Cobalamin (vitamin B12) It is solely synthesized by microorganisms and the only source for humans is food of animal origin like meat, fish and dairy products. Adult daily losses (mainly in urine and feces) are 1-3 ug and so daily requirements are also 1-3 ug. Body stores are of the order of 2-3 mg, sufficient for 3-4 years if supplies are completely cut off.
- 9. Transportation path of Vit B12Diet Stomach B12 IF B12+ IF Ileum B12+IF TCII B12 +TCII Circulation Bone marrow )DNA synthesis( Liver )storage( Other tissues )DNA synthesis(
- 10. Important for DNA synthesis, nervous tissue and fat metabolism in the liver an intermediate of the citric acid cycle, porphyrin synthesis (Heme synthesis)
- 11. Vit B12 plays important role in two reactions: • Necessary in the synthesis of methionine from homocysteine. 1. In this reaction both vit B12 and folic acid are involved. 2. B12 acts as a co-enzyme (methyl cobalamin) for methyltransferase. Homocysteine methionineMethyl B 12 Methyl THF THF • Vit B12 is important in conversion of methylmalonyl CoA to succinyl CoA in Krebs cycle. 1. In this reaction B12 acts as co-enzyme for methylmalonyl Co A mutase. Methylmalonyl Co A Succinyl Co A Adenosyl Cb Ado B12
- 14. Pernicious Anemia Most common cause of cobalamin deficiency caused by failure of the gastric mucosa to secrete intrinsic factor Immune Abnormalities 1. Anti–parietal cell antibodies 2. Anti–intrinsic factor antibodies -Two types Blocking” antibodies, which block the binding of cobalamin to IF Binding” antibodies, which bind to the cobalamin–IF complex and prevent the complex from binding to receptors in the ileum
- 15. The Schilling test Radioactive cobalamin (Cbl*) is taken orally; followed by injection of a saturating dose of non-radioactive cobalamin. The level of Cbl* is measured in the urine. In pernicious anemia the excreted levels of Cbl* are low. If intrinsic factor is given with the Cbl* the Cbl* levels will correct in PA, but not in ileal malabsorption.
- 16. SCHILLING TEST
- 17. Folate Folic acid is parent compound of large family of natural folate compounds. Its highest concentration is found in liver, yeast, spinach, other greens and nuts. Folate easily destroyed by heating, particularly in large volumes of water. Total folate in adult is ~10mg with liver containing the largest store. Daily adult requirements are ~100 μg and so stores are sufficient for 3-4 months in normal adult and severe folate deficiency may develop rapidly.
- 19. Absorption Absorption: during absorption in the upper small intestine, folates are converted to MTHF. Once inside the cells they are converted to folate polyglutamates. Location: duodenum and jejunum. Transport: folate found in circulation as mono-glutamate MTHF, transported to the liver and B.M by bound loosely to proteins including albumin and α2-macroglobulin.
- 22. Biochemical basis of megaloblastic anemia The folate is needed as coenzyme 5,10-methylene THF polyglutame for conversion of dUMP to dTMP. In deficiencies of folate or cobalamin, there is failure to convert of dUMP to dTMP; precursor of dTTP. The availablity of 5,10-MTHF is reduced in either cobalamin or folate deficiency. in cobalamin deficiency due to failure of formation of THF, the substrate on which folate polyglutame are build, MTHF accumulates in plasma and intracsellular concentration fall; termed as THF starvation or methylfolate trap.
- 23. Pathogensis Megaloblastic anemia are group of disorders characterized by distinct morphological pattern in hematpoitic stem cells. A common feature is a defect in DNA synthesis with lesser alterations in RNA and protien synthesis, leading to state of unbalanced cell growth and impaired cell division. Most RBCs are not resting but vainly engaged in attempting to double their DNA,with frequent arrest in S phase and lesser degree of arrest in other phases of cycle. An increased percentage of RBCs have increased DNA content is expressed morphologically as larger than normal “immature nucli” with finely particulate chromatin whereas the relatively unimpaired RNA and protein synthesis results in larger cells with greater “mature” cytoplasm and cell volume. The microscopic appearance of this nuclear-cytoplasmic asynchrony is morphologically discribed as “megaloblastic”.
- 24. Clinical features Many patients are diagnosed through finding of a raised MCV on rotuine CBC. The main clinical features in more severe cases are those of anemia. Anorexia is usually marked and there may be weight loss, diarrhea or constipation. Glossitis, angular cheilosis and mild fever in more severely anemic patients, Juandice(unconjugated) and reversible skin melanin hyperpigmentation also may occur with deficiency of cobalamin or folates. Thrombocytopenia sometimes leads to bruising and this may be aggrevated by vitamin C deficiency or alcohol in malnourished patients. Anemia and low leukocyte count may predispose to infections, particularly of respiratory and urinary tract. Cobalamin deficiency has also been associated with impaired bactericidal function of phagocytes.
- 27. Diagnosis of megaloblastic anemia Hematological findings 1. Peripheral blood 2. Bone marrow 3. Ineffective hematopoiesis 4. Chromosome abnomalities Diagnosis of cobalamin and folate deficiencies 1. Serum cobalamin 2. Serum folate 3. Red cell folate 4. Serum methylmalonate and homocysteine
- 28. Laboratory findings Hb: low RBCs count: low PCV: may not reflect the actual decrease in erythrocytes because of the enlarged size of the RBCs. MCV: high MCH: high MCHC: normal Leucocyte count: low PLT count: usually low
- 29. Blood film: RBCs: • Moderate to marked anisocytosis and poikilocytosis with many macrocytic ovalocytes. • Tear drop and fragmented cells may be seen. • Megaloblasts may seen in the P.B. • Red cell inclusions: Howell-jolly bodies, Cabot ring and basophilic stippling may present. WBCs: • Hyper-segmented neutrophils is classical finding PLT: • Giant form is usually present.
- 30. Reticulocyte count: low B.M: • Hypercellular with increased M:E ratio. • Increased ratio of megaloblasts. • Giant metamyelocytes are characteristics. • Megakaryocytes: reduced in number. Biochemical tests: • Serum B12: low • Serum folic acid: low • Serum bilirubin: increased • Serum LDH: increased.
- 32. PB MorphologyPB Morphology Macro-ovalocytes Howell-Jolly bodies Hypersegmented neutrophils Bi-nucleated RBCs
- 34. THANK YOU