
Recommended
More Related Content
Similar to humerus shaft
Similar to humerus shaft (20)
Recently uploaded
Recently uploaded (20)
humerus shaft
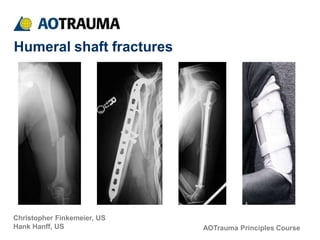
- 1. AOTrauma Principles Course Christopher Finkemeier, US Hank Hanff, US Humeral shaft fractures
- 2. Objectives • Identify several acceptable treatment strategies for humeral diaphyseal fractures • Learn the operative indications for humeral diaphyseal fractures • Understand the benefits and limitations of the various treatment strategies
- 3. Humeral shaft fractures • Humeral shaft fractures account for approximately 1–3% of all fractures [Beaty 1996, Zuckerman, 1996] • Usually the result of blunt trauma such as a fall or from high-energy trauma including motor vehicle accidents and gunshot injuries • Fracture displacement is the result of muscular forces
- 4. General considerations • • Energy of injury? Associated injuries? (isolated vs polytrauma) Status of soft tissues? Radial nerve function? Patient factors? • • • - - Obesity Expectations • • Stable vs unstable? Need upper extremity weight bearing? Open or closed? Exploration? Nonoperative treatment? Do patients demand or expect perfect x-rays? • • • •
- 5. Treatment options Nonoperative: • • • Coaptation splint Hanging arm cast Functional orthosis Operative: • • • • • • • Compression plating Intramedullary fixation Antegrade Retrograde Interlocking Flexible External fixation
- 6. Nonoperative treatment Indications: • Isolated injury • Adequate alignment after splinting - - AP bowing < 20o lateral bowing < 300 • Preferred method • Functional orthosis
- 7. Nonoperative treatment Functional orthosis Collar-and-cuff
- 8. Nonoperative treatment 17-year-old man, isolated fracture, closed injury from snowboarding
- 9. Nonoperative treatment—10 days postinjury after orthosis
- 10. Nonoperative treatment—21 days post injury with orthosis in place
- 11. Nonoperative treatment—11 weeks postinjury 15° varus 12° anterior angulation
- 12. Nonoperative treatment • • 15° varus 12° anterior angulation
- 13. Nonoperative treatment Sarmiento, et al (2000) J Bone Joint Surg Am • Followed 620 patients with humeral shaft fractures treated with cast bracing Non-union rate: < 2% of closed fractures Refracture rate: 1% between 2 and 8 weeks post cast removal Radial Nerve Palsy: 11% Most common was varus angulation (16%) with 10°–20° of angulation • • • •
- 14. Humeral shaft fractures—operative indications • • • Open fractures Vascular injury Radial nerve palsy after closed reduction Floating elbow Failure of closed treatment Pathologic fractures (bone metastases) Brachial plexus injury • • • •
- 15. Humeral shaft fractures—relative operative indications • Polytrauma • Bilateral humeral fractures • Morbid obesity • Segmental fractures • Need to use crutches
- 16. Humeral shaft fractures—operative options • • • Plate fixation Interlocked IM nail Ender’s nails, rush rods External fixation •
- 17. Humeral shaft fractures—external fixation • Open fractures with extensive soft-tissue injuries • Severe contamination
- 18. Humeral shaft fractures—indications for plate fixation • Fractures requiring nerve or vascular exploration • Very distal fractures • Very proximal fractures • Any diaphyseal fracture
- 20. Humeral shaft fractures—surgical approaches • Anterolateral: - Proximal and middle third • Posterior: - Distal and middle third
- 21. Humeral shaft fractures—anterolateral approach • Supine • Good for polytraumatized patient
- 22. Humeral shaft fractures—anterolateral approach • Deltopectoral approach proximally • Interval between biceps and brachialis • Split brachialis fibers
- 23. Humeral shaft fractures—posterior approach • Prone or lateral • Arm draped over padded support
- 24. Humeral shaft fractures—posterior approach • Interval between lateral and long heads of triceps • Identify radial nerve • Split medial (deep) head
- 25. Humeral shaft fractures—posterior plate • Tension band • Placed beneath radial nerve • Dictate location of nerve
- 26. Humeral shaft fractures—implants • Broad 4.5 large fragment plate • Small bone individuals: - - Narrow large fragment plate Small fragment plate 3.5
- 27. Absolute stability Relative stability
- 28. Humeral shaft fractures—flexible nails • Ender nails • Antegrade or retrograde • Rotational control? • Migration problems
- 29. Intramedullary fixation—flexible nails 22-year-old with acetabular fracture and closed humeral fracture
- 30. Intramedullary fixation—flexible nails • Multiple, flexible, retrograde IM nails • Early weight bearing allowed on upper extremity • Callous at 4 weeks postoperative Nancy nails
- 31. Intramedullary fixation—flexible nails Fracture healed at 3 months
- 32. Intramedullary fixation—flexible nails Brumback, et al (1986) JBJS • 63 fractures, 58 followed up • Both antegrade and retrograde • 94% union rate • Retrograde insertion proximal to olecranon fossa gave excellent results
- 33. Humeral shaft fractures—antegrade locked IM nails • Pathological and osteopenic fractures • Good rotational/length control • Good healing rates • Often allows weight bearing
- 34. Humeral shaft fractures—antegrade locked IM nails Concerns: • • • Insertion often damages rotator cuff tendons Inrtamedullary canal narrows distally Neurovascular injury at interlocking sites X
- 35. Open reducation internal fixation ORIF vs intramedullary nailing • Two randomized prospective studies published compare ORIF to IM nailing • Chapman et al (2000) concluded that “neither method was shown to be markedly superior to each other although nails were associated with a higher incidence of shoulder discomfort.” • McCormack et at (2000) suggested that “DCP fixation should continue to be regarded as the best treatment for fractures of the humeral shaft which require surgical stabilization.”
- 36. Humeral shaft fractures—locked IM nails Design modifications to avoid shoulder problems: • More lateral entrance site • Retrograde insertion
- 38. Stannard et al (2003) J Bone Joint Surg Am • 42 consecutive patients • 95% union rate • All nonunions (2) occured with 7.5 mm nail • 10% shoulder pain • 24% some loss of motion • All patients with loss of motion and shoulder pain had RETROGRADE nails
- 39. Humeral shaft fractures—retrograde IM nailing • Interlocked nails may also be inserted through distal site • Care to avoid fracture at entrance site
- 41. Humeral shaft fractures—radial nerve palsy • • • • Incidence 1.8–24 % Most are a neuropraxia > 70–90% recover spontaneously EMG (electromyography) if no evidence of recovery at 6–12 weeks
- 42. Humeral shaft fractures—radial nerve palsy • Associated fracture patterns • Transverse mid third - Usually neuropraxia • Spiral distal third - - Holstein-Lewis fracture Higher risk of laceration or nerve entrapment
- 43. Humeral shaft fractures—immediate radial nerve exploration • Open fractures • Distal-third spiral fractures • Secondary palsy following closed reduction
- 44. Summary • Most humeral shaft fractures can be treated successfully with a functional brace • Flexible nails are an effective treatment method • Plates and nails have “similar” union rates, but nails have more complications • Plates are preferable