
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (16)
Similar to 3.4 Mecánica muscular
Similar to 3.4 Mecánica muscular (20)
More from EMotionFormacion
Recently uploaded
Recently uploaded (20)
3.4 Mecánica muscular
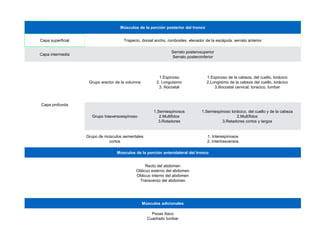
- 1. Músculos de la porción posterior del tronco Capa superficial Trapecio, dorsal ancho, romboides, elevador de la escápula, serrato anterior Capa intermedia Serrato posterosuperior Serrato posteroinferior Capa profunda Grupo erector de la columna 1.Espinoso 2. Longuisimo 3. Iliocostal 1.Espinoso de la cabeza, del cuello, torácico 2.Longísimo de la cabeza del cuello, torácico 3.Iliocostal cervical, toracico, lumbar Grupo trasversoespinoso 1.Semiespinosos 2.Multifidos 3.Rotadores 1.Semiespinoso torácico, del cuello y de la cabeza 2.Multífidos 3.Retadores cortos y largos Grupo de músculos sementales cortos 1. Interespinosos 2. Intertrasversos Músculos de la porción anterolateral del tronco Recto del abdomen Oblicuo externo del abdomen Oblicuo interno del abdomen Transverso del abdomen Músculos adicionales Psoas iliaco Cuadrado lumbar
- 2. Bergmark (1989) Sistema de estabilización local (SEL) Sistema de estabilización global (SEG) Discurren de un segmento a otro de la columna Músculos largos que saltean sus inserciones varios segmentos vertebrales Transverso Multifidos Rotadores diafragma suelo Pélvico Recto abdominal oblicuo externo erectores espinales Cuadrado lumbar, oblicuo interno y psoas
- 3. CARACTERISTICAS MUSCULARES (Mark D.Faries Et al 2007) LOCAL GLOBAL MUSCULATURA PROFUNDA NATURALEZA FIBRAS LENTAS ACTIVOS EN ACTIVIDADES DURADERAS SELECTIVAMENTE DEBILITADOS ACTIVADOS A BAJOS NIVELES DE INTENSIDAD (30-40% DE LA MAXIMA CONTRACCIÓN VOLUNTARIA) MUSCULATURA SUPERFICIAL NATURALEZA FIBRAS RAPIDAS ACTIVOS EN ACTIVIDADES POTENTES RECLUTAMIENTO FACILITADO ACTIVADOS A ALTOS NIVELES DE INTENSIDAD (POR ENCIMA DEL 40% DE LA MAXIMA CONTRACCION VOLUNTARIA)
- 4. Grupo erector de la columna 1.Espinoso 2. Longuisimo 3. Iliocostal 1.Espinoso de la cabeza, del cuello, torácico 2.Longísimo de la cabeza del cuello, torácico 3.Iliocostal cervical, toracico, lumbar 75% fibra s lentas
- 5. ESPINOSOS O ESPINALES (espinoso torácico, espinoso del cuello, espinoso de la cabeza) Origen: Apófisis espinosas Inserción: Apófisis espinosas Función: Eje A-P: Inclinación lateral (poca mecánica) Eje S-I: Rotación (poca mecánica) Eje L-M: Extensión (buena mecánica)
- 6. LONGISSIMUS (dorsal largo) (1. dorsal 2. cuello 3. cabeza) Origen: 1. Apófisis espinosas vertebras lumbares y sacras 2. Apófisis transversas vertebras dorsales 3. Apófisis transversas vertebras cervicales Inserción: 1. Costillas 9-12 2. Costillas 1-9 3. Apófisis mastoides del temporal Función: Eje A-P: Inclinación lateral (buena mecánica) Eje S-I: Rotación (poca mecanica) Eje L-M: Extensión (buena mecánica, plano predominante)
- 7. ILIOCOSTAL(1.fibras lumbares, 2. fibras torácicas, 3. fibras cervicales) Origen: 1. Cresta iliaca y fascia toracolumbar 2. Costillas 7-12 3. Apófisis transversas cervicales Inserción: 1. Costillas 6-12 2. Costillas 1-6 3. Apófisis transversas cervicales Función: Eje A-P: Inclinación lateral (buena mecánica, plano predominante) Eje S-I: Poca rotación Eje L-M: Extensión (buena mecánica,) 1 2 3
- 8. ILIOCOSTAL(1.fibras lumbares, 2. fibras torácicas, 3. fibras cervicales) Origen: 1. Cresta iliaca y fascia toracolumbar 2. Costillas 7-12 3. Apófisis transversas cervicales Inserción: 1. Costillas 6-12 2. Costillas 1-6 3. Apófisis transversas cervicales Función: Eje A-P: Inclinación lateral (buena mecánica, plano predominante) Eje S-I: Poca rotación Eje L-M: Extensión (buena mecánica,) 1 2 3 (www.researchreviewservice.com) The efficiency of correctiveexerciseinterventionson thoracic hyper-kyphosisangle Journal of Back & Musculoskeletal Rehabilitation 2014; 27: 7-16 Seidi F, Rajabi R, Ebrahimi I, et al. Reviewed by Dr. CearaHigginsDC (Research Review Service) ABSTRACT Background And Objective: Correctiveexerciseinterventionsareoften utilized tomanagesubjectswith thoracichyper-kyphosis, yet thequalityof evidencethat supportstheir efficiencyislacking. In thisstudy, the efficacyof local and comprehensivecorrectiveexerciseprograms(LCEPand CCEP) on kyphosisanglewas evaluated. Material And Method: A prospective, randomised controlled design wasused in thepresent study. Sixty patientswith postural hyper-kyphosisdeformity( 42°) entered thestudyfor 12 weeks. Subjectswere⩾ randomlyassigned toaLCEP(n=20), CCEP(n=20), or Control groups(n=20). Pre- and post-participation levelsof kyphosisangleweremeasured byflexicurveruler. Results: Both theLCEPand CCEPgroupsdemonstrated statisticallysignificant reductionsin thoracic kyphosisanglecompared tothecontrol group(p=0.001). Furthermore, based on Cohen'sd-value, the efficiencyof CCEPwaslarger than LCEP. Conclusions: Consideringtheextremelylargeeffect sizeof theCCEP, werecommend that thisprogram be used in thecorrection of postural hyper-kyphosisdeformityin future. right tragus, acromion processof thescapula, and thespinousprocessof C7 weremarked with removable, red adhesivedotsand theparticipant wasplaced 9 inchesout from awall which wasset up with awall mounted grid. A tripod-mounted digital camerawasplaced 104 inchesfrom thewall and adjusted to placethetripod level with theparticipant’sright shoulder. Theparticipant wasinstructed to bend forward threetimesand then raisehandsoverhead threetimesbeforeassumingacomfortable, erect posturewith their weight distributed evenly between their feet and their eyesfixed on theopposite wall. Threephotoswerethen taken within 5 seconds. AdobeAutoCAD 2010 wasused to measurethe anglebetween alineconnecting thetragusand C7 and avertical linethrough C7 (forward head angle) and theanglebetween alineconnectingC7 and theacromion and thesamevertical line(forward shoulder angle). Theaveragefrom thethreephotoswasrecorded asforward head and forward shoulder anglesfor each participant. Exercise Interventions: Both theLCEPand CCEPgroupsweregiven exercisesto perform threetimesper week for 12 weeks under thedirect supervision of theexaminers. Local CorrectiveExerciseProgram(LCEP): TheLCEPgroup received exercisesbased on Kendall’stheory that had been included repeatedly in previousstudies. They aimed to stretch thepectoral musclesand strengthen thethoracic extensor musclesthrough theuseof stretching, self-mobilization, and strengthening, with an emphasison endurance. In each session theparticipantswarmed up with light aerobic activity for 5 minutes, then performed two stretching(exercises1 and 2), oneself-mobilization (exercise3), and two strengthening exercises(exercises4 and 5) sequentially, then cooled down with general stretchingexercisesand slow walkingfor 5 minutes. Thefoam rollersused in stretching exercise2 weregradually increased in diameter from 15 cm to 20 cm and then to 25 cm to increasethestretch. 5 oracicKyphosisMeasurement exicurveruler, 50cm in length and 2cm wide, wasused to measurethoracic kyphosisangle. movable, red adhesivedotswereused to mark thespinousprocessesof T2 and T12. Participantswere n asked to stand barefoot on thebaseof aplatform in acomfortable, erect posturewith their body ght evenly distributed between their feet and their eyesfixed on theoppositewall. Theexaminer n waited 1-minuteuntil theparticipant returned to their normal posturebeforepositioning two wels, which werehorizontally mounted on thespinestabilizer instrument (SSI) on an adjustable nd, to lightly touch thexyphoid processof theparticipant’ssternum and their pubic symphysisin er to control postural sway. Theexaminer then molded theflexicurveruler to theparticipant’s racic spineand marked theintersection with thered adhesivedotsat T2 and T12 on theruler with a ker. Theflexicurveruler wasthen carefully lifted from theparticipant’sspinewithout altering the figuration of thecurveand placed on apieceof whiteposter board whereit washeld whilean stant traced theoutlineof thecurveand marked thepointscorresponding toT2 and T12. The icipant stepped off theplatform for 1-minuteof rest. Theparticipant then stepped back onto the form into previously traced outlinesof their feet, thespinousprocessesof T2 and T12 wereagain ked and themeasurement procedurewasrepeated. Thethoracic curvewastraced onto theopposite eof thewhiteposter board to prevent theinitial contour from influencingtheexaminer. TheT2 and 2 pointson each curvewereconnected usingastraight line(L line) and then thislinewasbisected at deepest point of thecurve(H line). esemeasurementswerethen inserted into an equation to calculatethethoracic kyphosisangle. The rageof thetwo angleswasrecorded asthethoracic kyphosisangleof each participant. eral photographic techniquewasused to measureforward head and forward shoulder angles. The 4 At theend of week 12 theinitial measurementswererepeated. A repeated measuresANOVA, paire N=60 18-25 años Hipercifosis ≥ 42° Cabeza adelantada ≥ 44° Hombros adelantados ≥ 49° Contracción dinamica 5.04° Contracción estatica 12.25° Grupo control 0.64° 1 serie/3 veces por semana/12 semanas
- 9. in-home based therapeutic exercise program on thoracic kyphosis angles 163 , H.K. ortality 220. coliosis e of the tecting 222. trarater opausal 1985. Spinal ne dys- ndrome 09. d M.H. s, Phys onship ol Ther d static J Hand ment of phome- al con- female Adher- recon- Rehabil nvasive t spine, ects of me exer- herapy m of the houlder ), 257– rement Appendix 1. Fig. 4. Four-step prone back extension. Start: arms raised from the floor, thorax raised from the floor, thorax lowered to floor, and arms lowered to the floor. This exercise was progressed to elbows fully extended and arms abducted approximately 125° in the frontal plane. D.W. Vaughn and E.W. Brown / The influence of an in-home based therapeutic exercise program on thoracic kyphosis angles 163 [12] D.M. Kado, W.S. Browner, L. Palermo, M.C. Nevitt, H.K. Genant and S.R. Cummings, Vertebral fractures and mortality in older women, Arch Intern Med 159 (1999), 1215–1220. [13] H.A. Keim and R.N. Hensinger, Spinal deformities: scoliosis and kyphosis, Clinical Symposia 41(4) (1989), 1–32. [14] D.J. Kolessar, G.T. Stollsteimer and R.R. Betz, The value of the measurement from T5 to T12 as a screening tool in detecting abnormal kyphosis, J Spinal Disord 9(3) (1996), 220–222. [15] K. Lundon, A. Li and S. Bibershtein, Interrater and intrarater reliability in the measurement of kyphosis in postmenopausal women with osteoporosis, Spine 23(18) (1998), 1978–1985. [16] R. McKenzie, Treat Your Own Neck, New Zealand: Spinal Publications, 1983. [17] J.Y. Menck, S.M. Requejo and K. Kulig, Thoracic spine dys- function in upper extremity chronic regional pain syndrome type I, J Orthop Sports Phys Ther 30(7) (2000), 401–409. [18] M.T. Moffroid, L.D. Haugh, H.A. Haig, S.M. Henry and M.H. Pope, Endurance training of the trunk extensor muscles, Phys Ther 73(1) (1993), 3–10. [19] M.K. Moore, Upper crossed syndrome and its relationship to cervicogenic headache, J Manipulative and Physiol Ther 27(6) (2004), 414–420. [20] C.B. Novak and S.E. Mackinnon, Repetitive use and static postures: a source of nerve compression and pain, J Hand Ther 10 (1997), 151–159. [21] G. Ohlen, E. Spangfort and C. Tingvall, Measurement of spinal configuration and mobility with DeBrunner’s kyphome- ter, Spine 14(6) (1989), 580–583. [22] G. Ohlen, T. Wredmark and E. Spangfort, Spinal sagittal con- figuration and mobility related to low-back pain in the female gymnast, Spine 14(8) (1989), 847–850. [23] T. Pizzari, N.F. Taylor, H. McBurney and J.A. Feller, Adher- ence to rehabilitation after anterior cruciate ligament recon- structive surgery: implications for outcome, J Sport Rehabil 14(3) (2005), 201–214. [24] S. Raine and L.T. Twomey, Validation of a non-invasive method of measuring the surface curvature of the erect spine, J Manual and Manipulative Ther 2(1) (1994), 11–21. [25] A.M.M. Schoo, M.E. Morris and Q.M. Bui, The effects of mode of exercise instruction on compliance with a home exer- cise program in older adults with osteoarthritis, Physiotherapy 91(2) (2005), 79–86. [26] J.S. Sobel, J.C. Winters and K. Groenier, Physical exam of the cervical spine and shoulder girdle in patients with shoulder complaints, J Manipulative Physiol Ther 20(4) (1997), 257– 262. [27] K.M. Tillotson and A.K. Burton, Noninvasive measurement of lumbar sagittal mobility. An assessment of the flexicurve technique, Spine 16(1) (1991), 29–33. [28] C. Wang, P. McClure, N.E. Pratt and R. Nobilini, Stretching and strengthening exercises: their effect on three-dimensional scapular kinematics, Arch Phys Med Rehabil 80(8) (1999), 923–929. [29] R.B. Winter and J.E. Hall, Kyphosis in childhood and adoles- cence, Spine 3(4) (1978), 285–308. Appendix 1. Fig. 4. Four-step prone back extension. Start: arms raised from the floor, thorax raised from the floor, thorax lowered to floor, and arms lowered to the floor. This exercise was progressed to elbows fully extended and arms abducted approximately 125° in the frontal plane. Fig. 5. Shoulder horizontal abduction/scapular adduction 4-step ex- ercise. Start: arms elevated at 90° in front of the body (as shown). Then, shoulders horizontally abducted to frontal plane, scapulae ad- ducted, scapulae return to initial position, and arms reach forward again. Exercise progressed to one higher level of band resistance. 164 D.W. Vaughn and E.W. Brown / The influence of an in-home based therapeutic exercise program on thoracic kyphosis angles Fig. 6. Cervical retraction exercise. Patient repeatedly emphasizes upper cervical flexion with lower cervical/upper thoracic extension; (A) (B) 164 D.W. Vaughn and E.W. Brown / The influence of an in-home based therapeutic exercise program on thoracic kyphosis angles Fig. 6. Cervical retraction exercise. Patient repeatedly emphasizes upper cervical flexion with lower cervical/upper thoracic extension; alternating position with the opposite (resting) cervical posture. Fig. 7. Self-mobilization of the thoracic spine into extension with a Styrofoam roll. (A) (B) Fig. 8. Thoracic extension exercise. (A) Patient begins in cervical, lumbar and thoracic flexion. She then is instructed to extend neck and thoracic spines on a segment-by-segment basis. She adducts scapulae at end of exercise. Pillow placed to encourage maintenance of relative lumbar flexion. 164 D.W. Vaughn and E.W. Brown / The influence of an in-home based therapeutic exercise program on thoracic kyphosis angles Fig. 6. Cervical retraction exercise. Patient repeatedly emphasizes upper cervical flexion with lower cervical/upper thoracic extension; alternating position with the opposite (resting) cervical posture. Fig. 7. Self-mobilization of the thoracic spine into extension with a Styrofoam roll. (A) (B) Fig. 8. Thoracic extension exercise. (A) Patient begins in cervical, lumbar and thoracic flexion. She then is instructed to extend neck and thoracic spines on a segment-by-segment basis. She adducts scapulae at end of exercise. Pillow placed to encourage maintenance of relative lumbar flexion. 164 D.W. Vaughn and E.W. Brown / The influence of an in-home based therapeutic exercise program on thoracic kyphosis angles Fig. 6. Cervical retraction exercise. Patient repeatedly emphasizes upper cervical flexion with lower cervical/upper thoracic extension; alternating position with the opposite (resting) cervical posture. Fig. 7. Self-mobilization of the thoracic spine into extension with a Styrofoam roll. (A) (B) Fig. 8. Thoracic extension exercise. (A) Patient begins in cervical, lumbar and thoracic flexion. She then is instructed to extend neck and thoracic spines on a segment-by-segment basis. She adducts scapulae at end of exercise. Pillow placed to encourage maintenance of relative lumbar flexion. Fig. 9. Yoga exercise to strengthen back extensors. Patient starts from flexed thoracic spine and arms internally rotated. Progresses to arms outwardly rotated and thorax extended (as shown). Leg position D.W. Vaughn and E.W. Brown / The influence of an in-home based therapeutic exercise program on thoracic kyphosis angles 165 Fig. 10. Latissimus Dorsi and Pectoralis Major stretch exercise. Pa- tient starts in “90-90” position of shoulders/elbows with arms relaxed on floor as shown. Patient takes arms overhead as far as possible. Goal is full elevation of arms overhead without losing floor contact. Leg position restricts compensatory lumbar extension. Appendix 2. (A) (B) Fig. 11. Alternative exercise for patients unable to do exercise shown in Fig. 8. Patient alternately flexes (A) and extends (B) thoracic spine from all-4’s position; emphasis on extension of thorax. Arms remain locked at elbows. Journal of Back and Musculoskeletal Rehabilitation 20 (2007) 155–165 155 IOS Press The influence of an in-home based therapeutic exercise program on thoracic kyphosis angles Daniel W. Vaughna,∗ and Eugene W. Brownb a Physical Therapy Program, Grand Valley State University, Grand Rapids, MI, USA b Department of Kinesiology, Michigan State University, 204 Intramural Sports Circle, East Lansing, MI, USA Abstract. Objective: Altered postural presentations have been associated with a variety of musculoskeletal disorders. Therapeutic exercise interventions are often utilized to manage patients with increased thoracic kyphosis or “round shoulders,” yet few controlled studies have evaluated their efficacy. Design: A prospective, randomized, controlled design was used to evaluate the influence of a home-based exercise regimen on these postural variances. Seventy-one patients with real or perceived concerns about their thoracic posture completed the 13-week study. Patients with 23–80◦ of thoracic kyphosis entered the study. Pre- and post-intervention flexicurve measurements of thoracic kyphosis were made. Patients were randomly assigned to an exercise (n = 32) or control group (n = 39). A mixed design ANOVA tested main effects and interactions. Results: A statistically significant (p < 0.05) interaction was found between group assignment and delta kyphosis values. Post- hoc analysis of the multiple comparisons produced a marginal p-value (p = 0.0557). Mean delta kyphosis values were (+ ) 0.5◦ (± 7.0◦ ) for the control group and (− ) 3.0◦ (± 6.1◦ ) for the experimental group. Conclusions: This 13-week home exercise program targeting modification of thoracic kyphosis angles had a statistically significant impact. However, post-hoc statistical analyses and clinical implications are marginal. Keywords: Evidence-based practice, outcome measures, postural relationships 1. Introduction 1.1. Influence of exercise on posture The normal range of thoracic kyphosis is 20–45 ◦ [6, 13–15,20–22]. Excessive kyphosis (> 45◦ ) is an eti- ological factor of, or significant impairment in, up- per quarter pathologies ranging from shoulder pain to spinal compression fractures [3,9,12,17,20,26]. Phys- ical therapists routinely use therapeutic exercises to manage patients with hyper-kyphosis. However, the quality of evidence that supports effective therapeutic exercise interventions for this postural abnormality is lacking. In 2001, Hrysomallis and Goodman [10] pub- ∗ Address for correspondence: D.W. Vaughn, Physical Therapy Program, Grand Valley State University, 260 CHS, 301 Michigan Street, NE, Grand Rapids, MI 49503, USA. Tel.: +1 616 331 2678; Fax: +1 616 331 5999; E-mail: vaughnd@gvsu.edu. lished a literature review which evaluated the effect of exercise for the correction of postural abnormalities. The authors concluded that, “Based on the existing lit- erature, it is inadvisable to strongly promote strength- ening exercises to correct postural malalignments, such as abducted scapulae, excessive lumbar lordosis, scol- iosis, or kyphosis.” (p. 389). Poor methodology and/or the absence of a control group confounded the results of many of the studies they reviewed [10]. Itoi and Sinaki [11] evaluated the effect of a prone- lying spinal extension exercise on kyphosis angles and thoracic spinal extensor strength. The study was con- ducted over a two-year period of time on 60 patients with estrogen deficiency. The patients were 49–65 years old (mean = 59). Their range of kyphosis an- gles was 9.5–69.5◦ (mean = 34.1◦ ). The experimen- tal group (n = 32) showed no statistically significant improvement in the kyphosis angle, as compared to the control group (n = 28). This was in spite of the fact ISSN 1053-8127/07/$17.00 Ó 2007 – IOS Press and the authors. All rights reserved N=71 21 a 63 años 13 semanas 4 sesiones/semana D.W. Vaughn and E.W. Brown / The influence of an in-home based therapeutic exercise program on thoracic kyphosis angles 165 Fig. 10. Latissimus Dorsi and Pectoralis Major stretch exercise. Pa- tient starts in “90-90” position of shoulders/elbows with arms relaxed on floor as shown. Patient takes arms overhead as far as possible. Goal is full elevation of arms overhead without losing floor contact. Leg position restricts compensatory lumbar extension. Appendix 2. (A) (B) Fig. 11. Alternative exercise for patients unable to do exercise shown in Fig. 8. Patient alternately flexes (A) and extends (B) thoracic spine from all-4’s position; emphasis on extension of thorax. Arms remain locked at elbows. Fig. 12. Alternative exercise for patients unable to do exercise shown in Fig. 7. Patient performs self mobilization of thoracic spine into extension by sliding roller up and down thoracic region through knee bending and straightening while holding self as erect as possible against the Styrofoam roll. D.W. Vaughn and E.W. Brown / The influence of an in-home based therapeutic exercise program on thoracic kyphosis angles 165 Fig. 10. Latissimus Dorsi and Pectoralis Major stretch exercise. Pa- tient starts in “90-90” position of shoulders/elbows with arms relaxed on floor as shown. Patient takes arms overhead as far as possible. Goal is full elevation of arms overhead without losing floor contact. Leg position restricts compensatory lumbar extension. Appendix 2. (A) (B) Fig. 11. Alternative exercise for patients unable to do exercise shown in Fig. 8. Patient alternately flexes (A) and extends (B) thoracic spine from all-4’s position; emphasis on extension of thorax. Arms remain locked at elbows. -3.0 Home exercise D.W. Vaughn and E.W. Brown / The influence of an in-home based therapeutic exercise program on thoracic kyphosis angles 157 3. had a ScoliometerT M reading of greater than five degrees at the point of peak axial rotation on the forward bending test. 4. had a structural kyphosis, confirmed by radio- graphs. 2.4. Screening of participants Following random assignment, patients were further screened by the lead investigator forlimitations in range of motion that would interfere with their ability to per- form the exercises. Patients were also screened for ex- cessive axial trunk rotation, using the ScoliometerT M . Amendt et al. [1] established the utility of this instru- ment for scoliosis screening. Since the exercises uti- lized in the present study were not designed to influence tri-planar thoracic curvatures, patients with potentially significant scoliosis were excluded from the study. 2.5. Kyphosis measurements The flexicurve is a malleable, metal ruler covered with plastic that can be bent only in a single plane. Once bent, it retains its shape to conformto the patient’s spine. Three consecutive thoracic kyphosis angle mea- sures were made. The mean of these measurements served as the pre-participation kyphosis angle. Every kyphosis angle measurement followed the same proto- col. The lead author first identified, through palpation, the spinous processes of T1 and T12 and marked them with a skin marker. The patient was asked to inhale and exhale without forcing out the breath. The flex- icurve was carefully conformed to the thoracic spine (Fig. 1). The researcher noted the span of the curve using the flexicurve’s ruler. This process was repeated three times. The lead author calculated the kyphosis angle from the three tracings. Figures 2 and 3 illustrate the method described by Hart and Rose [8], as well as the trigonometric calculation, used to determine the kyphosis angle in the current study. 2.6. Exercise protocol and instruction A literature review produced few articles where exer- cises were prescribed specifically to influence postural changes in the adult thoracic spine. The seven exercis- es prescribed in the current study were a combination of strengthening, stretching, and self-mobilization ac- tivities (Appendix 1). The exercises targeting Erector Spinae strength were selected on the basis of evidence provided by Moffroid et al. [18]. The cervical retrac- Fig. 1. Application of the flexicurve to the patient’s back for kyphosis measurement. tion exercise was recommended by McKenzie [16] and Moore [19] for its postural realignment value. The in- terscapular muscle strengthening and pectoral stretch- ing exercises were validated by Wang et al. [28] as a way to improveupper trunk posture and scapular stabil- ity. These authors reported a reduction of thoracic “an- terior inclination” as a result of their six-week exercise program. The exercises in this study were carefully dosed by a research assistant. This licensed physical therapist has more than 20 years of clinical practice in primarily outpatient orthopedic settings. Her primary intent in teaching the exercises was accurate performance with- out discomfort. The research assistant contacted the patients within 24 hours of his/her initial data collection session. The assistant determined the patient’s group assignment by inquiring as to the number the patient rolled on the die. Patients assigned to the control group were told that they would be contacted in three months for a follow- up data collection session. No further contact with this group occurred until the follow-up appointment was established. Patients assigned to the experimental group were given an appointment with the research assistant in order to learn the exercises. All seven exercises were prescribed with appropri- ate progressions defined for repetitions, resistance (in the case of the TherabandT M (Hygenic Corporation, Akron OH) exercises), and hold times over the course of the 13-week training program. Two levels of band resistance were given to the patient at the training ses- sion; one appropriate to the patient’s abilities at the initial session and a second band one resistance grade higher. Detailed written and pictorial descriptions (Ap-
- 10. 15,3% en niños de 11 años (Hazebroek- Kampschreur A.A et al. 1992) 38% en adultos de 20 a 50 años (Morris GP. et al 1992) 35% en adultos de 20 a 65% (Cutler WB et al 1993) INCIDENCIA HIPERCIFOSIS Relación con….. *Mayor indice de caídas *Patologias respiratorias *Dolor cervial *Reducción espacio subacromial *Impingement sulbcromial *Aumento de la mortalidad
- 12. SEMIESPINALES (cruzan 6 a 8 vertebras) 1.De la cabeza 2.Del cuello 3. Torácico Origen: apófisis transversas a espinosas Inserción: Apófisis espinosas Función: Eje A-P: Inclinación lateral poca mecanica Eje S-I: Rotación contralateral (buena mecánica) Eje L-M: Extensión (buena mecanica
- 13. MULTIFIDOS (cruzan de 2 a 4 vertebras) Origen: Sacro, espina iliaca y apófisis transversas Inserción: Apófisis espinosas Función: Eje A-P: Inclinación lateral poca mecanica Eje S-I: Rotación (buena mecánica) Eje L-M: Extensión (buena mecanica)
- 16. ROTADORES (cruzan 1-2 vertebras) (rotadores cortos y largos) Origen: Sacro, espina iliaca y apófisis transversas Inserción: Apófisis espinosas Función: Eje A-P: Inclinación lateral poca mecanica Eje S-I: Rotación (buena mecánica) Eje L-M: Extensión (buena mecanica)
- 17. INTERTRANSVERSOS Origen: Apófisis transversas Inserción: Apófisis transversas INTERESPINOSOS Origen: Apófisis espinosas Inserción: Apófisis espinosas Función: Eje A-P: Inclinación lateral Eje S-I: Rotación (poca mecánica) Eje L-M: Extensión Grupo de músculos segmentales cortos 1. Interespinosos 2. Intertrasversos
- 20. Recto abdominal Superiores: (costilla 5,6 y 7 - cresta y sinfisis pubica) Plano predominante flexión Ligera flexión ipsilateral Ligera flexión contralateral Torax sobre pelvis fijo Inferiores: (costilla 5,6 y 7- cresta y sinfisis pubica) Plano predominante flexión Ligera flexión ipsilateral Ligera flexión contralateral Pelvis sobre tórax fijo
- 21. Inferiores (linea alba hasta sínfisis púbica ligamento inguinal, cresta ilíaca, fascia toracolumbar) Flexión poca mecánica Flexión ipsilateral ligera mecánica Rot. ipsilateral Pelvis Pelvis sobre tórax fijo (Rotación) 2 1 Superiores (linea alba desde ombligo hasta apófisis xifoides cartílagos costales, costilla 10) Flexión muy poca mecánica Flexión ipsilateral ligera mecánica Rot. Contralateral Tronco Torax sobre pelvis fijo (Rotación) Transverso
- 22. Estabilización local mejora dolor lumbar O’sullivan et al.Spine. 1999 Mejor 4 apoyosactivación Beith, R Man Ther 2001 Entrenar aislado Hodges, P. Man Ther 2001 Mejora extensión cadera Madokoro,S. et al JPST 2014 Masestable que brace Richardson, M et al, Spine. 2002 Respuesta anticipadora Hodges, P.Arch Phys Med Rehabil 1999
- 23. Oblicuo externo Anteriores superiores (1) (costilla laterales 10-12 - labio externa cresta iliaca) Rotación contralateral Flexión poca mecánica Flexión lateral poca mecánica Torax sobre pelvis fijo (Flex 20º+ Rot contral) 1 2 3
- 24. Oblicuo externo Laterales (3) (costilla laterales 10-12 - labio externa cresta iliaca) Flexión lateral Flexión poca mecánica Rot. contralateral poca mecánica Pelvis sobre tórax fijo (Flex + flexión lat) 1 2 3 Anteriores inferiores (2) (costilla 7-9 - lig inguinal y zona inferior linea alba) Rotación contralateral Flexión Flexión ipsilateral Torax sobre pelvis fijo (Flex + Rot contra)
- 25. Anteriores superiores (2) (lateral ligamento inguinal y mitad anterior cresta iliaca capas anteriores de la linea alba y vaina abdominal Flexión tronco Flexión ipsilateral poca mecánica Rot. ipsilateral pelvis Pelvis sobre tórax fijo (Flex + Rot ipsi) 2 3 4 1 Anteriores inferiores (1) (Al igual que transverso fibras inferiores) Oblicuo interno
- 26. Oblicuo interno Laterales anteriores(3) (zona lateral cresta iliaca capas superiores de la linea alba y costillas 9-10 Flexión tronco (mecánica tronco sobre pelvis) Flexión ipsilateral buena mecanica Rot. ipsilateral torax debil Torax sobre pelvis fijo (Flex ipsi) 2 3 4 1 Laterales posteriores(4) (zona latero-posterior cresta iliaca - fascia toracolumbar costillas 10-11-12 Flexión tronco poca mecánica Flexión ipsilateral buena mecánica Rot. ipsilateral torax poca mecánica Torax sobre pelvis fijo (Flex ipsi)
- 28. CUADRADO LUMBAR Origen: ¼ posterior de la cresta ilia ca Inserción: costilla 12 y apófisis tran sversas L1-L4 Eje A-P: Inclinación lateral (buena mecánica, pelvis sobre torax fijo) Eje S-I: Ligera rotación Eje L-M: Extensón