Endodontic surgery
•
17 likes•2,464 views

Dr. Bhavik Miyani, Resident Doctor in Department of Oral and Maxillofacial Surgery, Narsinhbhai Patel Dental College and Hospital, Visnagar.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Endodontic surgery
Similar to Endodontic surgery (20)
More from Dr Bhavik Miyani
More from Dr Bhavik Miyani (20)
Recently uploaded
Recently uploaded (20)
Endodontic surgery
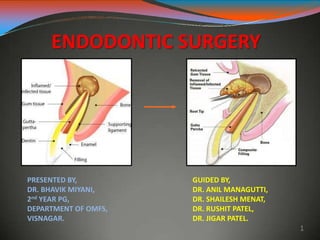
- 1. ENDODONTIC SURGERY PRESENTED BY, DR. BHAVIK MIYANI, 2nd YEAR PG, DEPARTMENT OF OMFS, VISNAGAR. GUIDED BY, DR. ANIL MANAGUTTI, DR. SHAILESH MENAT, DR. RUSHIT PATEL, DR. JIGAR PATEL. 1
- 2. Introduction Over the past decade, periradicular surgery has continued toevolve intoa precise, biologically based adjunct to nonsurgical root canaltherapy. Although nonsurgical endodontic treatment gives good results in mostcases, surgery may be indicated for teeth with persistent periradicular pathoses that have not responded to nonsurgicalapproaches. 2
- 3. History Over 1,500 years ago - Aetius, a Greek physician performed first recorded endodonticsurgical procedure - incision and drainageof an acuteendodontic abscess 5000 BC – Sushruta – performed excision of palatalgrowth 9th century – Abulcasis – performed surgical removal of epulis andCautery procedure 1728 - Pierre Fauchard - Replantation and Transplantationtechniques 1845 - Hullihen - ‘Hullihen’s surgery’ or ‘Rhizodontrophy’ orTrephination procedure 3
- 4. History 1871 – Smith - First root endresection 1880 – Brophy - Root end filling 1881 - Claude Martin - Father of root endresection 1884 – Farrar - Rootamputation Surgical operating microscopes – - 1980’s - Endodonticmicrosurgery 1990s – Dr. Gary Carrsurgical ultrasonic tips firstdesigned – Carr tips 1999 – Spartan/Obtura - Kim Surgical tips – Kistips 4
- 5. Definition A surgical procedure related to problem of the pulp less or periodontallly involved tooth, requiring root amputationand endodontictherapy. (John I Ingle) Removal of tissuesotherthan thecontents of therootcanal space to retain a tooth with pulpal and/orperiapical involvement. (Franklin Weine) 5
- 6. Rationale Toremove thecausativeagentsof periradicularpathology. Torestore the periodontium toa stateof biologic and functional health. 6
- 7. Objectives Toensure the placementof a properseal between the periodontium and the root canalforamina. 7
- 8. Indications Glick and Ingle 1. Need for surgicaldrainage Incision and drainage Trephination 2. Failed nonsurgical endodontic treatment Irretrievable root canalfilling,material Irretrievable intraradicularpost 3. Calcific metamorphosis of the pulpspace 4. Procedural errors Instrument fragmentation Non-negotiable ledging Root perforation Symptomatic overfilling 5. Anatomicvariations Rootdilaceration Apical rootfenestration 8
- 9. 6. Biopsy 7. Correctivesurgery Root resorptivedefects Rootcaries Root resection Hemi section Bicuspidization 8. Replacement surgery Replacement surgery Intentional replantation (extraction/replantation) Post-traumatic Implantsurgery Endodontic Osseo integrated 9
- 10. Relative Contraindications 1. Patient’s medical status Major system disorder – Cardiovascular, Respiratory, Digestive, Hepatic, Renal, Immune, Skeleton-muscular 2. Anatomical considerations Nasal floor Maxillary sinus Proximity to neurovascular bundles of mandibular canal and mental foramen limitations to adequate visual and mechanical access 3. Practitioner’s skill and experience 10
- 12. CLASSIFICATION (by Kim et al) Based on sequence of use: Examination instruments Incision blades Elevation instruments Tissue retractioninstruments Curettage instruments Osteotomyinstruments Inspection instruments Retro fill carriers Retro fill Pluggers Miscellaneous instruments Suturing instruments Suction tips Irrigation instruments Ultrasonic instruments Surgical operating microscope 12
- 13. Examination Instruments Dental mirror Periodontal probe Endodontic explorer Micro explorer Tip of microexplorer used to – • Search for leak in root-end filling • Distinguish canal or craze line from microfracture line 13
- 14. Incision blades Bard Parker Blades: Microblade No. 15c No. 15 No. 12 No. 11 15C blade in use Microblades 14
- 15. Elevation Instruments Traditional Microsurgical Enlarged tips of soft tissue elevators Molt’s curette (above) Periosteal elevator No. 9 (below) 15
- 16. Tissue Retraction Instruments Arens tissueretractor Selden retractor University of Minnesotaretractor Cats paw retractor 16
- 17. Curettage Instruments •Minicurettes •Mini jacquette 34/35 •Columbia 13- 14 •Miniendodontic curettes •Minimolten curettes Enlarged tips of minijacquettes and mini- endodontic curettes 17
- 18. Osteotomy Instruments Straight Handpiece Microhead Handpiece Impact air 45o handpiece with H161 Lindemann bone cutting bur – instrument of choice for osteotomy 18
- 19. No. 4 round bur No. 6 round bur No. 8 round bur No. 57 fissurebur Multipurpose bur Endo-Z bur 19
- 20. Inspection Instruments Micro mirrors Round and modified rectangular Flexible neck Stainless steel (top and bottom) Scratch-free sapphire mirror surface (centre two) 20
- 23. Surgical Operating Microscope Magnification Range = 2X - 32X MAGNIFICATION RANGE Low: 3 - 8 X Medium: 10 – 16 X High: 20 – 30 X The surgical operating microscope was used first time in neurosurgery and ophthalmology in 1960 and Endodontic microsurgeries in 1980s 23
- 24. Advantages High magnification Surgical technique can be performedprecisely and accurately Surgical technique can be easilyevaluated Fewer radiographs needed Video recordingspossible Reduces occupationalstress 24
- 25. Classification of Endodontic surgery Fisulative surgery Incision anddrainage Cortical trephination Decompression procedures Periradicularsurgery Curettage Root-end resection Root-end preparation Root-end filling Correctivesurgery Perforation repair Mechanical (iatrogenic) Resorptive Periodontal management Root resection Tooth resection Intentional replantation 25
- 26. Surgical Drainage : Surgical drainage is indicated when purulentand/or hemorrhagic exudates forms within the soft tissue and the alveolarbone; a result of a symptomatic Periradicularabscess. Surgical drainage maybe accomplished by; Incision and drainage (I and D) cortical Trephination 26
- 27. Incision And Drainage Procedure Local anesthetic - Mepivacaine (low pKa) Horizontal incision with No.11 or 12 BP blade at the base ofthe fluctuant area Frank et al - rubber dam drain to maintain the patency of thesurgical opening. McDonald and Hovland - incision alone Gutmann and Harrison- use of drain is Indicated in moderate to severe cellulitis and other positive signs of an aggressive infective process. 27
- 29. Materialsused Iodoformgauze Rubberdam material -“H” or “Christmastree” shape. Penrosedrain Penrose drain Serrated drain 29
- 30. 30
- 31. Trephination Cortical trephination is a procedure involving the perforation of the cortical plate to accomplish the release of pressure from the accumulation of exudate within the alveolar bone. No 6 or 8 round bur Buccal approach The objective is to create a pathway through the cancellous bone to the vicinity of the involved periradicular tissues. 31
- 33. Treatment planning for periradicular surgery 1. Presurgical patientmanagement 2. Need for profound local anesthesia andhemostasis 3. Management of softtissue 4. Management of hardtissues 5. Surgical access, both visual andoperative 6. Access to rootstructure 7. Periradicularcurettage 8. Root-end resection 9. Root endpreparation 10. Root-end restoration 11. Soft-tissue repositioning andsuturing 12. Postsurgical care 33
- 34. PRESURGICAL PATIENT MANAGEMENT Patients medical status Proper history taking is first key forsuccessof any surgical procedure. Patientshould beevaluated for majorsystem disorders (cardiovascular, renal, hepatic, digestive, immune and skeletal muscle) which may contraindicate or alter approach tosurgery. Also premedication for patient in normal or in presence of any of the above medical conditions should begiven priorityand consulted with physician. 34
- 35. Patientpreparation Patient preparation starts with patient communication regarding reason for surgery, risks involved, also factors which improve prognosis forsuccessful outcomeof surgical procedure. There may be necessity of premedication (sedatives or hypnotics, systemic antibiotics) for patient in order to improve accessibility also postsurgicalhealing. Presurgical mouth rinse with chlorhexidine gluconate (Peridex) may improve surgical environment bydecreasing tissue surface bacterialcontamination. Mouth rinse should be started aday before surgery, immediately before surgery, and up to 4 to 5 days post surgically. This reduces bacterial contamination of surgical site and improve woundhealing. 35
- 36. Anaesthesia Local anaesthetic withvasoconstrictor Objectives: obtain profound and prolongedanaesthesia providegood hemostasis bothduring and afterthe surgical procedure Selection based on: Medical status of thepatient Desired duration of anaesthesia 36
- 37. TYPES OF LOCAL ANALGESIA Topical analgesia (surfaceanalgesia) Sub mucosal infiltration Sub periosteal infiltration Nerve blockanalgesia Intra ligamentaryanalgesia. Intra osseousanalgesia. 2 1 3 6 5 4 37
- 38. TOPICAL ANALGESIA (SURFACE ANALGESIA) An anaesthetic is applied in a gel form to the intact mucous membrane. It passes through the epidermis and makes the nerve endings analgesic prior to administration of a deeper or infiltration analgesic. Use-The surface analgesia prevents the pain of the needle. 38
- 39. Treatment planning for periradicular surgery 1. Presurgical patientmanagement 2. Need for profound local anesthesia andhemostasis 3. Management of softtissue 4. Management of hardtissues 5. Surgical access, both visual andoperative 6. Access to rootstructure 7. Periradicularcurettage 8. Root-end resection 9. Root endpreparation 10. Root-end restoration 11. Soft-tissue repositioning andsuturing 12. Postsurgical care 39
- 40. Management of soft tissue PRINCIPLES OF FLAP DESIGN 1. Making sure base of the flap should be wider than the freeend. 2. Avoiding the incision overa bonydefect 3. Including the full extent of thelesion. 4. Avoiding sharpcorners 5. Avoiding incision across a bonyeminence 40
- 41. 6. Avoiding incision in the mucogingival junction. 7. Taking care during retraction. 8.Incision should be made with firm, continuous firm strokeperpendicularto thecortical bone plate. 9.The sutured flap margin should rest on solidcortical boneplate. 41
- 42. Classification Full thickness (Mucoperiosteal) - Epithelium + Connective tissue+ Periosteum Partial thickness (Split) - Epithelium + Connectivetissue According to Gutmann & Harrison Full mucoperiosteal Limited mucoperiosteal Full mucoperiosteal flap – no attached Gingiva around neck of crown Limited mucoperiosteal showing - Remaining attached gingiva 42
- 43. Full mucoperiosteal flap Triangular Rectangular Trapezoidal Horizontal/Envelope Papilla base Limited mucoperiosteal Sub marginal curved/Semilunar Sub marginal scalloped rectangular/Luebke Ochsenbein 43
- 44. Advantages of Full Mucoperiosteal Flaps 1. Rapid wound healing 2. Good surgicalaccess 3. Minimal disruption of bloodsupply 4. Minimal untoward post-surgical sequelae 5. Optimal apical orientationand 6. Primary intentional healing. Disadvantages 1. Loss of soft tissueattachment 2. Loss of crestal boneheight 3. Post surgical flapdislodgement 44
- 45. Advantages of limited mucoperiosteal flap 1. Marginal and interdental gingiva notinvolved 2. Unaltered soft tissue attachmentlevel 3. Crestal bone is notexposed 4. Adequate surgical accessand 5. Good would healing potential Disadvantages 1. Disruption of blood supply to unflappedtissues 2. Flapshrinkage 3. Difficult flap re-approximation 4. Delayed secondary wound healing. 5. Limited apical orientation 45
- 46. TRIANGULAR FLAP INDICATIONS: Mid root perforationrepair Periapical surgery in posteriorareaswith shortroots ADVANTAGES: ○ Good wound healing ○ Minimal disruptionof vascularsupply to flapped tissue ○ Easeof flap re-approximation with minimum numberof sutures DISADVANTAGES: ○ Limited surgicalaccess ○ Difficult toexpose the rootapices of long teeth like maxillary and mandibularcanines ○ Tension is created onretraction 46
- 47. 47
- 48. RECTANGULAR FLAP INDICATIONS: Mandibularanteriors Multiple teeth Teeth with long roots like maxillarycanines ADVANTAGES: Increased surgical access torootapex Reduces retractiontension DISADVANTAGES: Difficulty in re-approximation of flapmargins Post surgical stabilization isdifficult Gingival attachmentviolated, gingival recession, crestal bone loss mayoccur 48
- 49. 49
- 50. TRAPEZOIDAL FLAP Similar to rectangular except the 2 vertical incisions intersect the horizontal incision atan obtuseangle → tocreatea broad based flap with thevestibularpartwider than thesulcularportion Disadvantages: Angled incision – severs more vitalstructures More bleeding Disruption of vascularsupply to non-flapped tissues Shrinkage of flapped tissues 50
- 51. HORIZONTAL FLAP Horizontal intrasulcularincisionwith novertical releasing incision Limited applications - Limitedaccess Repairof cervical defects (rootperforations, resorption, caries) Hemi sections and Rootamputation ADVANTAGES: Ease of repositioning as novertical incision DISADVANTAGES: Limited access andvisibility Difficult to reflect andretract Predisposed to stretching andtearing 51
- 52. SUBMARGINAL CURVED/SEMILUNAR FLAP ADVANTAGES Reduces incisionand reflection time Maintain integrityof gingival attachment Eliminates potential crestal bone loss INDICATION 1. Esthetic crownspresent 2. Trephination DISADVANTAGES Limited access and visibility Tendency for increase hemorrhage Crosses rooteminences May not include entire lesion Predisposed to stretching and tearing Repositioning is difficult Healing is associated with scar 52
- 53. SUBMARGINAL SCALLOPED RECTANGULAR/ LUEBKE OCHSENBEIN FLAP Modification of rectangularflap Horizontal incision is placed in buccal/labial attached gingiva & is scalloped - follows thecontourof marginal gingiva INDICATIONS Prostheticcrowns Periradicular surgery of anteriorregion longerroots 53
- 54. ADVANTAGES Ease in incision and reflection Enhanced visibility and access Ease in repositioning Maintains integrity of attachment Prevent gingival recession Avoid dehiscence Prevent crestal bone loss DISADVANTAGE Horizontal component disrupts blood supply Vertical componentscrosses mucogingival junction and may enter muscle tissue Difficult to alter if sizeof lesion misjudged 54
- 55. INCISION Incisions for the majorityof mucoperiosteal flaps for periradicularsurgerycan beaccomplished by ; No.11, NO.12, No.15, No.15C, micro surgical blade. 55
- 56. FLAP REFLECTION Flap reflection is the process of separating thesoft tissue (Gingiva Mucosaand Periosteum) from thesurfaceof thealveolar bone. Thisprocess should begin in thevertical incisiona few millimeter apical tothe junctionof the horizontal and vertical incisions. Periosteal elevatorforflap reflectionare ; No.1 and No.2 (Thompson Dental Manufacturing Co) No.2 (Union Bronch) No.9 (Union Bronch Co) 56
- 57. FLAP RETRACTION Processof holding in position the reflected soft tissues Provides visual and operativeaccess Tissueretractormustalways reston solid cortical bonewith firm lightpressure 57
- 58. HARD TISSUE MANAGEMENT Osteotomy Following reflectionand retraction of the mucoperiosteal flap, surgical access must be made through thecortical bone to the roots of theteeth. Methods to locate the rootapex Methylene bluedye Visual and tactilemethod(Barnes) 1. Rootstructuregenerally has ayellowish color 2. Roots does not bleed whenprobed 3. Roottexture in smoothand hard as opposed to thegranularand porous nature of bone 4. Theroot is surrounded by the PDL 58
- 59. OPTIMAL OSTEOTOMY SIZE Traditional endodontic surgery - approximately 10 mmin diameter. Should be just largeenough to manipulate ultrasonic tips freely within the bonecrypt. Since the length of an ultrasonic tip is 3 mm, the ideal diameter of an osteotomy is about4mm. 59
- 60. Periradicular curettage A surgical procedure to remove diseased or reactivetissue from alveolar bone in the periradicular area or lateral region surrounding a pulp less tooth (AAE 1994) Purpose: • To remove pathological periradicular tissues for visibility and accessibility for treatment of apical root canal system •To remove foreign material present in periradicular tissues 60
- 61. Toaccomplish removal of entire mass, the largest bone curette, consistent with the size of the lesion, is placed between the soft tissue mass and lateral wall of the bonycrypt with concavesurfaceof curette facing thebone. Once soft tissue has been freed along the periphery of the lesion, the bonecuretteshould be turned with concaveportion towards thesoft tissue and used in scraping fashion to free tissue from deep walls of bonycrypt. 61
- 62. Root End Resection Indications Eliminating Anatomicalvariations Ledges Canal obstructions Resorptivedefects Perforationdefects Separated instruments Visualizeseal created by orthogradetreatmentand need forroot- end seal Gain access to pathological tissue trapped along lingual surfaceof root 62
- 63. Ingle et al recommended the root end resection is best accomplished by the No.702 tapered fissure bur or No.6 or No.8 round bur in a low speed straight hand piece. Lasers Komori and associatesevaluated the useof the Er:YAG laser forroot-end resections: Er:YAG laser - smooth, clean, resected rootsurfaces freeof anysigns of thermal damage. INSTRUMENTS 63
- 64. Moritz and associates CO2 laser treatment optimally prepares the resectedroot-end surfacetoreceivea root-end filling seals the dentinaltubules eliminates niches for bacterialgrowth sterilizes the rootsurface Advantages of the laseruse: Absence of discomfort andvibrations Less chance forcontaminationof thesurgical site Reduced risk of trauma to adjacenttissue 64
- 65. Rationale for laser use in endodonticperiradicularsurgery includes (Miserendino etal) (1) improved homeostasisand concurrentvisualizationof the operative field (2) potential sterilizationof thecontaminated rootapex (3) potential reduction in permeabilityof root-surfacedentin (4) reduction of post-operativepain (5) reduced risk of contamination of the surgical site through eliminationof the useof aerosol-producing airturbine hand pieces. 65
- 66. EXTENT OF APICAL RESECTION 66
- 67. BEVEL ANGLE Historically – 30-45o: togainvisual and operating access to the root tip for resection, placement of retro filling materials, and inspection. Present - 90o Maximum= 10o degree bevel Advantages: •Exposes fewer dentinal tubules, thus preventing excess leakage and contamination. 67
- 68. ROOT END PREPARATION Purpose: • Tocreateacavity toreceivea root-end filling. Objective: It must be placed parallel to the long axis of the root. Instruments Used: Small round or inverted coneburs Ultrasonictips 68
- 69. IDEAL ROOT END PREPARATION Theapical 3 mm of the rootcanal must be freshlycleaned and shaped. The preparation must be parallel toand coincidentwith the anatomic outlineof the pulp space. Adequateretention form must becreated. All isthmus tissue, when present, must beremoved. Remaining dentin walls must not beweakened. 69
- 70. Traditional root-end cavity preparation technique Miniaturecontra-angleorstraight hand piece Small round or inverted conebur. Class I cavity preparation along the long axis of the rootwithin the confines of the rootcanal. Recommended depth - 2 to 3 mm being the mostcommonly advocated. (Gutmann and Harrison) Disadvantage: Apical perforationdue todifficulty in aligning the bur 70
- 71. Recently, speciallydesigned ultrasonicrootend preparation instruments have beendeveloped. Ultrasonictips developed by De Gary Carr- Availablewith plain and diamond coated tips. Kis Microsurgical Ultrasonic Instruments – The tips arecoated with zirconium nitrite for faster dentin cutting with less ultrasonic energy 71
- 72. Advantages of Ultrasonic tips over micro head burs Need for bevelingeliminated Tipstayscentered in rootand followscanal space ↓ chances of lingual orlateral root perforations Conserving greaterthicknessof rootcanal wall Betteraccess tosurgical areas, especiallydifficult toreach areas such as lingual apices Deeper root-end preparationachieved 72
- 73. Less dentinal tubulesexposed Cleanercavity than bur – smoother, less debrisand smear layer Ultra precise isthmuspreparations. Parallel canal walls preparation for betterretentionof filling materials. Drawbacks: Creationof microcracks due tovibrationsproduced 73
- 74. RETROGRADE RESTORATIVE MATERIALS AND TECHNIQUES Purpose: Toseal theapex so that no bacteriaor bacterial by productscan enteror leave from thecanal Properties of ideal retrograde restorative materials: Well tolerated by periapical tissues Bactericidal orbacteriostatic Adhere to thetooth Dimensionallystable Readilyavailableand easy to handle 74
- 75. Notstain teethorperiradiculartissue Noncorrosive Resistant todissolution Electrochemically inactive Promote Cementogenesis Radiopaque 75
- 76. Root End filing materials : Guttapercha Amalgam Cavit IRM Super EBA Glass Ionomer Compositeresins Carboxylatecements Zinc phosphatecements Zinc oxide eugenolcements Mineral trioxide aggregation(MTA) 76
- 77. The prognosis ultimately depends on factors such as: An accuratebevel Adequateaccess Homeostasis Accurate retrogradepreparation Accurate retrograderestoration Existent periodontaldisease Occlusal trauma Missed verticalfractures Quality of the orthogradefilling Individuals hostresponse. 77
- 78. SOFT TISSUE REPOSITIONING AND COMPRESSION Theelevated muco periosteumgentlyreplaced to itsoriginal position with the incision lines approximated as closelyas possible. Typeof flap designwill affect theease of repositioning. Tissuecompression: Using a surgical gauze moistened with sterile saline, gently apply firm pressure to the flapped tissue for 2 to 3 minutes (5 minutes forpalatal tissue) beforesuturing. Enhances intravascularclotting in thesevered blood vessels 78
- 79. SUTURING Purpose: Toapproximatethe incised tissueand stabilize the flapped muco periosteum until reattachmentoccurs. CLASSIFICATION OF SUTURE MATERIALS Based on material: Natural Collagen Gut Silk Syntheticfibers Nylon Polyester Polyglactin Polyglycolicacid Absorbency: Nonabsorbable Silk Nylon Absorbable Polyester Polyglactin Polyglycolicacid Collagen Gut 79
- 80. Size: USP size: 3-0, 4-0, 5-0, 6-0. The higherthe first number, thesmaller thediameterof the suture material. Structure: Monofilament and Multifilament Twisted and Braided 80
- 81. Silk Sutures: Non absorbable, multi filamentous, andbraided. High capillaryeffect Enhances movement of fluids and microorganisms between fibers Plaque accumulation on thefibers Severe oral tissuereactions Prevented by postoperative rinse withchlorhexidine Advantage: Ease of manipulation 81
- 82. Gut:Collagen is the basic component of plain gut suture material derived from sheep or bovineintestines. Thecollagen is treated withdiluted formaldehyde to increase its strength Shaped into the appropriate monofilamentsize. Gutsuturesareabsorbable in 10 days Chromic gut: plain gut treated with chromium trioxide. delayed absorptionrate Gutsuture material is available in sterilepackets containing isopropyl alcohol. 82
- 83. Polyglycolic Acid (PGA): made from fibers of polymerized glycolic acid- absorbable. The rateof absorption is about 16 to 20 days. Multi-filament, braided and handling characteristicssimilartosilk. Firstsyntheticabsorbablesutureand it is manufactured as Dexon. Polyglactin (PG): Developed by Craig and coworkers In1975 Copolymerof lacticacid and glycolicacid Called polyglactin 910 (90 partsglycolic acid and 10 parts lacticacid). Suturesof polyglactin areabsorbable, braided and multi filament. Commercially available asVicryl 83
- 84. NEEDLES Needle with reversecutting edge (the cutting edge is on theoutside of the curve) is preferable. Available in arcs of 1/4, 3/8, 1/2 and 5/8 of a circle, with the most useful being the 3/8 and 1/2circle. 84
- 85. SINGLE INTERRUPTED SUTURE SUTURING TECHNIQUES
- 86. INTERRUPTED LOOP (INTERDENTAL) SUTURE 86
- 87. POST OPERATIVE INSTRUCTIONS AND CARE Do not lift up lipor pull back thecheek to look at where the surgery was done. A little bleeding from surgical is normal. This should only last fora few hours. A little swelling and bruising face may be evidentwhich may last fora few days. Do not drink alcohol oruse tobacco (smoke orchew) for the next 3 days. Havea good, soft dietand drink lots of liquids for the first few days after surgery. 87
- 88. Place an ice bag (cold) on face where the surgery was done. Leave it on for 20 minutes and take it off for 20 minutes. Continue this for 6 to 8 hours. Take the prescribed medicines asrecommended. Rinse the mouth with 1 tablespoon of the chlorhexidine mouthwash twice daily for 5days. Sutureremoval after5-7 days by thedental personnel only. Maintain postoperative follow up recall visits If any problemsexists informand visityourdentist immediately. 88
- 89. BARRIER MEMBRANE TECHNIQUES IN ENDODONTIC SURGERY Regeneration: is the replacementof destroyed tissuewith new tissue formed by the cells of the same origin. This new tissue reacts in a similar manneragainst pathologicstimuli as theoriginal tissues. Repair: is the restorationof thedestroyed tissue bydiseasewith new tissue consisting of cells different from the original cells. These cells reactdifferently from theoriginal cells against pathologicstimuli. 89
- 90. Materials used: GTR membrane Calciumsulphate Periosteal graft Platelet richplasma Tri calcium phosphate Objective: To enhance the quality and quantity of bone regeneration in the peripheral region and to accelerate bone growth in circumscribed bonecavitiesafterendodonticsurgery. 90
- 91. GTR Membrane Indication Through and through periapicallesion. Large periapical lesion Endo-perio lesion Periapical lesion communicating with thealveolarcrest Furcation involvementas a resultof perforation Rootperforationwith bone loss toalveolarcrest 91
- 92. Advantages: ○ Barrier function in case of lack ofperiosteum. ○ Greaterconcentration of osteogenic cells in the healing area ○ High successrate. Disadvantages: ○ Cost ○ Possibility of infection ○ Need fora second surgery (non resorbablematerialsonly) ○ Need for a space-maintaining device in largedefects ○ Problems in the application of thebarrier. ○ Operatorskill (e.g. , high surgical skill required whena palatal flap is raised) 92
- 93. CALCIUM SULFATE Indications : Post apicoectomy bonedefects Through and throughlesions Periapical lesions with furcationinvolvement Post surgical endo-periocommunications. Advantages: Inexpensive No inflammatoryreaction Absence of post operativecomplications. Possibility of using the materialseven in asepticenvironment Ability toachievesecondaryclosureof soft tissueon theexposed material. Stabilization of blood clot. Adhesion to rootsurface. Biocompatible Completeabsorption. 93
- 94. PERIOSTEAL GRAFT AS BARRIER MATERIAL: (Kwan et al 1998) Actions: 1. Periosteum Osteo progenitorcells Osteogenesis 2.Barrier for epithelialinfiltration Indications: multifaceted endodontic- periodontic problems Advantages: ○ Highlyvascular ○ Easily harvested ○ Configuration adjusted to shape of recipientsite Disadvantages: ○ Profuse bleeding ○ Difficulty in obtaining the split thicknessgraft 94
- 95. Platelet rich plasma – Rich source of growth factors Properties andAdvantages: •Decreased intra operative and post operativebleeding •Rapid soft tissuehealing •Rapid vascularization •Decreased post operativepain •Osteoconductive •Hemostaticproperties •Safe •Affordable (Demiral et al JOE , 30 (11) , 2004) PLATELET RICH PLASMA + TRI CALCIUM PHOSPHATE 95
- 96. Corrective surgery Correctivesurgery is categorized as surgery involving thecorrectionof defects in the bodyof the roototherthan theapex. Corrective surgical procedure may be necessary as a result of procedural accidents, resorption (internal orexternal), rootcaries, root fracture, periodontaldisease. Corrective surgery mayinvolve Rootresection. Hemi section. Intentional replantation. 96
- 97. ROOT AMPUTATION Rootamputation proceduresarea logical way toeliminatea weak, diseased root toallow the strongerroot(s) tosurvivewhen, if retained together, they would collectivelyfail. 97
- 98. Distance between pulpchamber floorand coronal aspectof the root separation= 3mm (Minimum) 2 mm allow forestablishmentof supracrestal attachmentapparatus and 1 mm for placement of crownmargins 98
- 99. INDICATIONS FOR ROOT AMPUTATION: (Rosenberg et al) Existence of periodontal bone loss to the extent that periodontal therapy and patient maintenance do not sufficiently improve the condition. Destructionof a root through resorptive processes, caries, or mechanical perforations. Surgically inoperable roots thatarecalcified, contain separated instruments, oraregrosslycurved. The fractureof one root thatdoes not involvetheother. Conditions that indicate the surgerywill be technically feasible to perform and the prognosis isreasonable. 99
- 100. CONTRAINDICATIONS FOR ROOT AMPUTATIONS: Lack of necessaryosseoussupport forthe remaining rootorroots. Fused rootsorroots in unfavorableproximitytoeach other. Remaining rootorrootsendodontically inoperable. Lack of patient motivation toproperly perform home-care procedures. 100
- 101. HEMISECTION Hemi section is defined as separationof a multi rooted toothand the removal of a root and the associated portion of the clinical crown. Sutures placedResected root Deep periodontal pocket Flap raised 101
- 102. BISECTION OR “BICUSPIDIZATION” Refers toadivisionof acrown that leave the two halves and the respectiveroots. BS should be considered in mandibular molars in which periodontal disease has invaded the bifurcation andrepair of internal furcation perforation has beenunsuccessful. The furcation is then turned intoan interproximal space where the tissue is more manageable by the patient 102
- 103. BICUSPIDIZATION 103
- 104. INTENTIONAL REPLANTATION Defined as theactof deliberately removing a toothand following examination, diagnosis, endodontic manipulation and repair returning the tooth into itsoriginal socket. INDICATIONS Difficultaccess Anatomic limitations Perforation in areas notaccessible surgically. Failed apical surgery Apical surgery creatingdefect Accidental avulsion( unintentionalreplantation) 104
- 105. Contraindication Pre-existing moderate to severe periodontaldisease Curved and flared roots Non restorabletooth Missing interseptal bone 3 factors that directly affect the outcome of intentional replantation. Extra oral time Keeping PDL cellsviable Minimizing damage to the cementum and pdl ligament cells during elevation andextraction 105
- 106. Endodontic microsurgery DEFINITION A surgical procedureon exceptionallysmall and complex structures with an operationmicroscope. (Kim etal) The microscope has changed surgical endodontics froma “blind” techniquetoone that is visuallydominated. Itenables thesurgeon toassess pathological changes moreprecisely and to remove pathological lesions with far greater precision, thus minimizing tissue damage duringsurgery. 106
- 107. Indications Failure of previous nonsurgical endodontictreatment Failure of previous endodonticsurgery Anatomicdeviation Procedural errors Contraindication Periodontal health of thetooth Patient healthconsideration Surgeons skill andability Hard tissue management Osteotomy: H161 lindermann bone cutter----- 8x to16x Periradicularcurettage: Columbia no 13 and no14 ---10x to 16x Apical resection: lindermann bur -----4xto8x 107
- 108. Comparison of traditional v/s microsurgery Kim and Rubenstein, 2001 PROCEDURE TRADITIONAL MICRO-SURGERY Identification of apex Difficult Precise Osteotomy Large (=>10 mm) Small (<5mm) Root surface inspection None Always Bevel angle Large (45o) Small (<10o) Isthmus identification Nearly impossible Easy Retro preparation Approximate Precise Root end filling Imprecise Precise 108
- 109. SURGICAL SEQUELAE Pain: - Minimal and of shortduration, if the tissue management is adequate - Long acting Localanesthetics - Analgesics and Anti inflammatorydrugs Swelling: Causes: ○ Post surgicaledema ○ Hematoma ○ Infection Management: Inform patient Reassurepatient Cold packapplication 109
- 110. MANAGEMENT: Cold pack application Pressure packs: 2X 2 inch gauge orwet tea bag held with moderate pressure for 10- 15 minutes. If severe return to thedental clinic - Resuturing and use of hemostatics (Tannic acid: hemostatic) •Improper elevation and Retraction •Incision into muscle attachment •Inadequate suturing •Trauma due to brushing, mastication Bleeding 110
- 111. Ecchymosis Discoloration of the facial or oral soft tissues caused by extravasation and subsequent breakdown in the subcutaneous tissue Common in elderly patients with fragile capillaries Causes: •Bruising •Soft tissue compression Depends on: site degree of trauma complexion 111
- 112. CONCLUSION Endodontic surgery is dynamic and it is imperative that scientific investigation continue, concepts ,techniques and materials used in endodontic surgery must be continually evaluated and modified and more emphasis must be placed on the assessment of long-term outcome 112
- 113. REFERENCE Pathways of the Pulp by Stephen Cohen, Richard C. Burns,7th,8th Edition Endodontics by John I. Ingle, Leif Bakland 5th Edition Microsurgery in Endodontics: Syngkuc Kim Surgical Endodontics: Guttman and Harrison: Mosby:1994. Contemporary surgical endodontics: Stockdale: 2 Edition Contemporary oral and maxillo facial surgery:Peterson: 5th Edition. Colour Atlas of surgical endodontics: Barnes Colour atlas of endodontic surgery:Loushine Microscopes in endodontics: DCNA: Syngkuc Kim, July; 41 (3)1997. Ultrasound real time imaging in the differential diagnosis of periapical lesions: Cotti et al. IEJ; 36; 2003. 113