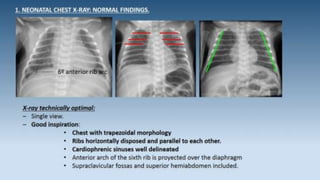
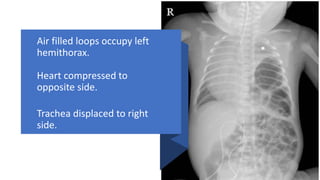
This document provides an overview of neonatal chest x-rays, including when they should and should not be performed, what a normal x-ray looks like, common positions of tubes and catheters, and common causes of respiratory distress in neonates. It discusses the appearance of a normal chest x-ray as well as conditions like respiratory distress syndrome, transient tachypnea of the newborn, meconium aspiration syndrome, and pneumonia. Surgical conditions like diaphragmatic hernia and esophageal atresia are also reviewed.