
Recommended
More Related Content
What's hot
What's hot (20)
Similar to MYOPIA CLINICAL
Similar to MYOPIA CLINICAL (20)
Recently uploaded
Recently uploaded (20)
MYOPIA CLINICAL
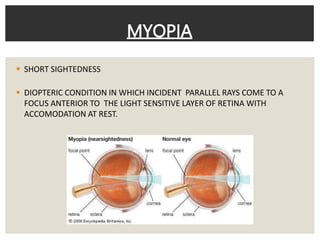
- 1. SHORT SIGHTEDNESS DIOPTERIC CONDITION IN WHICH INCIDENT PARALLEL RAYS COME TO A FOCUS ANTERIOR TO THE LIGHT SENSITIVE LAYER OF RETINA WITH ACCOMODATION AT REST. MYOPIA
- 2. Optics of Myopia Image of distant object - circle of diffusion formed by divergent beam parallel rays of light coming from infinity – in front of the retina Far point - finite point in the front of eye near object situated at far point is focused without an effort of accommodation Nodal point in a myopic eye is further away from the retina therefore the image formed will be larger than it would be in a emmetropic eye. Angle Alpha- negative -> convergent squint accommodation in uncorrected myopes is not developed normally
- 3. 1. Axial myopia Commonest form Increase in antero-posterior length of the eyeball 2. Curvatural myopia Increased curvature of cornea, lens or both 3. Positional myopia Produced by anterior placement of crystalline lens in eye 4. Index myopia Increase in the refractive index of crystalline lens associated with nuclear sclerosis 5. Myopia due to excessive accomodation Spasm of accomodation ETIOLOGICAL CLASSIFICATION
- 4. 1. Congenital myopia 2. Simple or developmental myopia 3. Pathological or degenerative myopia 4. Acquired myopia which may be Post traumatic Post keratitic Drug induced Pseudomyopia Space myopia Night myopia Consecutive myopia CLINICAL CLASSI.FICATION
- 5. AGE ONSET CLASSI. CONGENITAL: since birth YOUTH ONSET: Below 20 yrs. ( Simple Myopia) EARLY ADULT ONSET: 20-40: Acquired Index myopia d/t Early NS LATE ADULT ONSET: 40+ AIM d/t Age NS
- 7. ◾Since birth ◾Diagnosed by 2-3 years ◾Mostly unilateral-Manifests as anisometropia ◾High degree of error: 8-10 D ◾Child may develop convergent squint in order to preferentially see clear at its far point (10-12cms) ◾Prematures, Marfan Sy, Homocystinuria ◾Associated with cataract, micropthalmos, aniridia, megalocornea, congenital separation of retina CONGENITAL MYOPIA
- 8. ◾ Developmental myopia- commonest variety ◾ School myopia (school going age 8 -12 years) ◾ Etiology Axial type: physiological variation in length of eye ball precocious neurological growth during childhood SIMPLE MYOPIA ◾ Curvatural type Underdevelopment of eye ball ◾ Role of diet in early childhood ◾ Role of genetics – Autosomal Dominant Prevalence in children both parents myopic(20%) One parent myopic(10%) No parent myopic(5%)
- 9. SYMPTOMS Begins bet. 7 to 10 yrs. – about -5D, never exceeds -8D. POOR VISION FOR DISTANCE: VA beyond Punctum Remotum affected HALF SHUTTING OF EYES: Stenopaeic vision ASTHENOPIC: Pts with small degree of myopia- Strain symp. d/t dissociation between convergence and accommodation 1. Convergence weakness, Exophoria, Suppression in one eye 2. Exce Accommodation – Ciliary Spasm
- 11. ◾Signs Prominent eyeballs Anterior chamber - deeper than normal Pupils- Large, sluggishly reacting Fundus- normal; temporal myopic crescent may be seen Magnitude of refractive error Increasing at rate -0.5+- 0.30/ year. Does not exceed 6 to 8 ◾Diagnosis Confirmed by performing retinoscopy
- 12. ◾Degenerative/ progressive myopia ◾Rapidly progressive error which starts in childhood at 5-10 years of age ◾High myopia in early adult life with degenerative changes PATHOLOGICAL MYOPIA
- 13. ◾Role of heredity Heredity linked growth of retina is the determinant in developmental myopia Sclera due its distensibility follows retinal growth but choroid undergoes degeneration due to stretching, which in turn causes degeneration of retina Progressive myopia is Familial More common in chinese,japanese,arabs and jews Uncommon among negroes,nubians and sudanese ETIOLOGY
- 14. ◾Role of general growth process Lengthening of the posterior segment of globe commences only during the period of active growth and ends with termination of active growth
- 15. Genetic factors (play major role) General growth process(minor) More growth of retina Stretching of sclera Increase axial length Degeneration of choroid Degeneration of retina Degeneration of vitreous
- 16. ◾Defective vision- uncorrectable loss of vision ◾Muscae volitantes Floating black opacities in front of eyes Degenerated liquified vitreous ◾Night blindness- In high myopes, d/t degenerative changes SYMPTOMS
- 17. ◾Prominent eye balls Elongation of eye ball mainly affects posterior pole and surrounding area ◾Cornea-large ◾Anterior chamber -deep ◾Pupils-slightly large ,react sluggishly to light SIGNS
- 18. ◾Fundus examination: Optic disc large and pale Temporal edge presents a characteristic myopic crescent- Atrophy of choroid - sclera visible Peripapillary crescent encircling the disc may be present, where choroid and retina is distracted away from disc margin Super traction crescent may be present on nasal side (retina pulled over disc margin)
- 21. Degenerative changes in retina and choroid Common in progressive myopia Characterized by white atrophic patches at macula with a little heaping of pigment around them
- 23. • FOSTER-FUCH’S SPOT: • Dark red circular patch due to sub- retinal neo vascularization and choroidal haemorrhage • Present at macula • CYSTOID DEGENERATION – at periphery • Advanced cases: Total Total retinal atrophy in central area
- 24. ◾Posterior staphyloma Due to ectasia of sclera at posterior pole It may be apparent as an excavation with vessels bending backward over margins
- 25. ◾Degenerative changes in vitreous include: Liquefaction Vitreous opacities Posterior vitreous detachment(PVD)- Weiss’ reflex
- 26. POSTERIOR STAPHYLOMA: d/t Ectasia of sclera at post. Pole LATTICE DEGENARATION- SNAIL TRACK LESION
- 29. ◾Visual fields Contraction Ring scotoma may be seen ◾ERG reveals subnormal electroretinogram due to chorioretinal atrophy
- 30. ◾Retinal detachment/Tears ◾Complicated cataract ◾NS ◾Vitreous haemorrhage ◾Choroidal haemorrhage+ Thrombosis ◾Strabismus fixus convergence ◾GLAUCOMA COMPLICATIONS
- 32. SECONDARY MYOPIA INDEX: • Nuclear Sclerosis- hyperrefrigent Nucleus • Incipient Cataract • Diabetic Myopia- RI decreases CURVATURAL: • Corneal- Ectasis, Keratoconus • Lenticular POSITIONAL- Ant. Subluxation of lens CONSECUTIVE- surgical overcorrection of Hypermetropia, IOL
- 33. o PSEUDOMYOPIA/ARTIFICIAL – Spasm of Accommodation o SPACE- Distance fixation o NIGHT/TWILIGHT- photopic to scotopic- shorter wavelengths o DRUG INDUCED- Cholinergic – Pilocarpine, Echothiophate, DIPFP o Steroid o Sulphonamides
- 34. MYOPIA OF PREMATURITY TRUE MOP: WITHOUT ROP MYOPIA OF ROP: Following T/t of ROP Abnormal dev of Ant. Seg. Corneal curvature Shallow Ant. Chamber Shorter axial lenth relative to their D value Due to: 1. Mechanical Restrcition of ocular growth Cryo treated eyes> Laser > I/vitr Anti-VEGF inj.
- 36. ◾Optical treatment of myopia Concave lenses Basic rule – minimum acceptance providing maximum vision ◾Modes of prescribing concave lens- 1. Spectacles 2. Contact lens TREATMENT OF MYOPIA
- 37. ◾Contact lenses are used in case of high myopia as they avoid peripheral distortion and minification produced by strong concave spectacle lens
- 39. ◾Radial keratotomy Making deep radial incisions in peripheral part of cornea leaving the central a 4mm optical zone These incisions on healing ; flatten the central cornea thereby reducing its refractive power Correct low to moderate myopia(2-6D) DISADVANTAGES: Cornea is weakened – globe rupture in sports persons Uneven healing – irregular astigmatism Patient may feel glare at night SURGICAL TREATMENT OF MYOPIA
- 41. ◾Photo refractive keratectomy (PRK) A central optical zone of anterior corneal stroma is photoablated using excimer laser (193nm uv flash) to cause flattening of central cornea Correction for -2 to - 6D of myopia
- 42. Disadvantages: Post operative recovery is slow Pain and discomfort Residual corneal haze in centre affecting vision Expensive
- 43. ◾Refractory surgery of choice for myopia of upto -12D LASER ASSISTED IN-SITU KERATOMILEUSIS(LASIK)
- 44. Flap of 130-160 micron thickness of anterior corneal tissue is raised Midstromal tissue is ablated directly with an excimer laser beam ultimately flattening the cornea
- 46. 1. Patients >20 years 2. Stable refraction for at least 12 months 3. Motivated patient 4. Absence of corneal pathology ◾Absolute contraindication for LASIK Presence of ectasia Corneal thickness <450mm PATIENT SELECTION CRITERIA
- 47. ◾Customised(C)-LASIK: Based on wave front technology Corrects spherical, cylindrical and other aberations present in eye Gives vision beyond 6/6 i.e.,6/5 or 6/4 ADVANCES IN LASIK
- 48. ◾Epi-(E) LASIK: Only epithelial sheet is separated with Epiedge Epikeratome Devoid of complications related to corneal stromal flap
- 50. ◾Minimal or no postoperative pain ◾Recovery of vision is very early as compared to PRK ◾No risk of perforation during surgery and rupture of globe due to trauma like RK ◾No residual haze unlike PRK where subepithelial scarring may occur ◾LASIK is effective in correcting myopia of -12D ADVANTAGES OF LASIK
- 51. Expensive Requires greater surgical skill than RK and PRK Flap related complications Intraoperative flap amputation Wrinkling of flap on repositioning Postoperative flap dislocation/subluxation Epithelization of flap – bed interface Irregular astigmatism DISADVANTAGES
- 54. ◾Intraocular contact lens implantation for correction of myopia of >12D ◾Special type of IOL is implanted in anterior chamber or posterior chamber anterior to natural crystalline lens PHAKIC INTRAOCULAR LENS
- 55. ◾Into the peripheral cornea at approximately 2/3rd stromal depth ◾Flattening of central cornea, decreasing myopia ◾Advantage: reversible procedure INTRACORNEAL RING (ICR) IMPLANTATION
- 56. ◾A non-surgical reversible method of molding the cornea with overnight wear unique rigid gas permeable contact lenses ◾Myopia correction upto -5D ◾Used in patients below 18 years of age ORTHOKERATOLOGY
- 57. ◾General measures : Balanced diet rich in vitamins and proteins Early management of associated debilitating disease ◾Low vision aids indicated in patients with progressive myopia with advanced degenerative changes ◾Prophylaxis Genetic counselling