Ocular toxoplasmosis
•Download as PPTX, PDF•
9 likes•2,895 views

presentation made during uveitis session.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Ocular toxoplasmosis
Similar to Ocular toxoplasmosis (20)
More from Bipin Bista
More from Bipin Bista (20)
Recently uploaded
Recently uploaded (20)
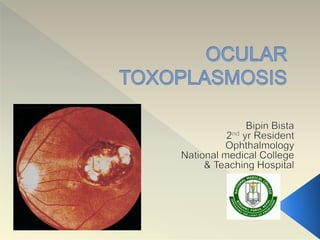
Ocular toxoplasmosis
- 2. O.T is a recurrent retinochoroiditis caused by the organism Toxoplasma gondii, and represents the most common cause of infectious posterior uveitis worldwide.
- 3. Most successful obligate intracellular parasite. Apicomplexan parasite infecting one third of the human population. Sexual reproduction occurs in intestine of members of the Felidae family among which cat represents the definitive host.
- 5. Tachyzoite (6-7 mm) is the active proliferative form; present in intermediate and definitive during acute infections . It is able to penetrate any nucleated cell and circulate all over the body, leading to cell lysis, direct tissue damage, subsequently to potentially destructive immune response.
- 6. Tachyzoite differentiate into bradyzoites , forming tissue cyst which are the latter forms and remains in host tissue without eliciting any significant inflammatory response.
- 7. Definitive hosts gets infected by either ingesting meat containing tissue cysts/tachyzoites from intermediate hosts, or by ingesting sporulated oocysts , present in the soil and shed in the faeces of another hosts. Once in the intestine , the parasite invades enterocytes and reproduces asexually and sexually. Felines shed oocysts 3-18 days after oral infection, gets matures in the soil into sporulated oocysts, become infective after 1-21 days, and persists for up to 18 months
- 8. Manifests as a focal retinochoroiditis with necrotizing granulomatous inflammation of retina with reactive granulomatous involvement of choroid, vitreous,anterior uvea. Mononuclear infiltrates . Disruption/Migration of RPE. After resolution CR Scar is seen. Pathogenesis depends upon a delicate balance between host immunity and parasite virulence. Adaptive immune response is mediated by CD4+ T lymphocytes and macrophages. Th-1 helper reaction leads to pro-inflammatory cytokines : IL-12, Interferon-Ý and TNF-
- 9. Type I : highly virulent : Strong proinflammatory response Type II : least virulent Type III : less virulent.
- 10. Systemic Disease Fever, malaise and variable lymphadenopathy. Pneumonitis Hepatitis Myocarditis Encephalitis Congenital T : IUFD, anaemia, thrombocytopenia, cutaneous rash, hepatitis,pneumonitis,myocarditis and even encephalitis. Sabin’s Tetrad : Hydrocephalus, Intracranial calcifications, Mental retardation and chorioretinits which occurs in less than 10 % of infected newborns . However, 80% of these infected newborns will manifest with chorioretinitis.
- 12. Retinochoroiditis : active : whitish yellowish exudates in inner retina with retinal edema. Begins from margin of satellite lesion. Involves full thickness of retina. Inflammatory cellular infiltrates may lead to granulomatous precipitates on the posterior hyaloid and to denser vitreous bands/haze – ‘headlight in the fog’ Periarterial lipidic exudates (Kyrielis arteriolitis). Granulomatous or non-granulomatous iridocyiclitis. Retinochoroidal lesion – ‘wagon –wheel’ scar
- 15. Essentially clinical, based on presence of necrotising chorioretinitis. Serological findings are supportive IgG Antibodies specific to T.gondii – previous exposure Absence of specific IgG & IgM exclused possibility of Toxoplasmosis IgM &/or IgA Ab, IgG Ab (High level)- Congenital Toxoplasmosis. PCR of ocular fluids. Goldman-Witmer or Witmer-Desmonts Coefficient : Serum titer of sp. T.gondii Ab vs globulin titers. Positivity of Vitreous sample > Aqueous humor samples.
- 16. May be self-limited Worsening of Intraocular inflammation as well as development of sight threatening complications indicates the necessity of treatment.
- 17. A lesion within temporal arcade A lesion abutting the optic nerve or threatening a large retinal vessels. A lesion that has induced a large degree of hemorrhage. A lesion that has induced enough of a vitreal inflammatory response that the visual acquity has dropped two line after acute infections Multiple recurrences that developed marked vitreal condensation.
- 18. Drugs Dosage Precaution Sulfadiazine 1 gm QID for Adults, 50-100mg/kg for children G6PDH,Crystalluria, Hepato-renal failure,SJS, BM supp. Pyrimethamine 100 mg followed by 25- 50 mg/day, 1mg/kg/day Teratogenic, HR failure, BM suppression- Use of folinic acid Clindamycin 300 mg QID, 10-25 mg/kg/day HR failure,Psudomembranou s colitis Azithromycin 250-500 mg/day,5 mg/kg/day GI disturbances Sulfamethoxazole / Trimethoprim 800/160 mg BD,40- 50/8—10 mg/kg/day HR failure, G6PDH Deficiency, Sulfa hypersensitivity Spiramycin 1.5 million IU (500 mg)QID High levels in placenta,GI abnormailty Atovaquone (Mepron) 750 mg qid, 30 mg/kg/day Liver failure, not for lactation/gestation.
- 19. Cryotherapy of peripheral lesions : Excess may lead to condensation and membrane formation. Photocoagulation Anti – VEGF Vitrectomy and lensectomy HAART therapy.
- 20. • Avoiding ingestion of raw/undercooked meat ,(-20 to -4˚c) overnight destroys tissue cysts. • Drinking only filtered or boiled water. • Carefully washing vegetables/fruits before consumption. • Using gloves and washing hands after manipulating soil/meat. • Avoid contact with felines & their faeces.
- 21. Reference: - Nussenblatt and whitecup 4th edition - Myron yanoff 4th edition