Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Effects of CTGF Overexpression on Fibrosis-Related Phenotypes
Similar to Effects of CTGF Overexpression on Fibrosis-Related Phenotypes (20)
Recently uploaded
Recently uploaded (20)
Effects of CTGF Overexpression on Fibrosis-Related Phenotypes
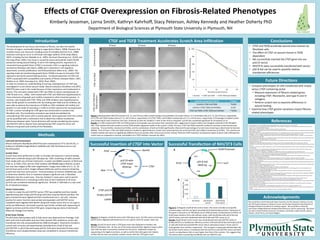
- 1. 0 0.02 0.04 0.06 0.08 No Vector pSV B-Gal & pUC19 pSV B-Gal & CTGF pUC19 Absorbance(405nm) Methods Acknowledgements Successful Insertion of CTGF into Vector Conclusions Future Directions Department of Biological Sciences at Plymouth State University in Plymouth, NH References CTGF and TGFβ Treatment Accelerates Scratch Area Infiltration • CTGF and TGFβ accelerate wound area invasion by fibroblast cells • The effect of CTGF on wound closure is TGFβ dependent • We successfully inserted the CTGF gene into our pUC19 vector • NIH/3T3s were successfully transfected with vector • pSV β-Gal can be used to quantify relative transfection efficiencies Effects of CTGF Overexpression on Fibrosis-Related Phenotypes Kimberly Jesseman, Lorna Smith, Kathryn Kahrhoff, Stacy Peterson, Ashley Kennedy and Heather Doherty PhD Introduction The development of scar tissue, also known as fibrosis, can alter the healthy function of organs, eventually leading to organ failure (Wynn, 2008). Diseases that manifest excess scar tissue are a leading cause of mortality (Gurtner et al., 2008). Excessive scarring can occur in all tissues and organ systems of the body (Wynn, 2007), including the liver (Bataller et al., 2005), the heart (Krenning et al., 2010), and the lungs (Phan, 2002). Scar tissue is caused by excess extracellular matrix (ECM) production during wound healing. To aid in the healing process, expression of connected tissue growth factor (CTGF) is increased. CTGF is a signaling molecule secreted by fibroblast cells (Wynn, 2008) and is important in cell migration, attachment, survival, proliferation, and ECM production (Blom et al., 2002). The signaling molecule transforming growth factor (TGFβ) is known to stimulate CTGF expression during the wound healing process. Increased expression of CTGF and TGFβ is associated with susceptibility and severity of fibrotic diseases (Wynn, 2007; Bataller et al., 2005; Krenning et al., 2010; Phan, 2002). In order to increase our understanding of scarring, overexpression of CTGF was investigated in a cell culture wound model. Mouse embryonic fibroblast cells (ATCC NIH/3T3) were used in this model because of their importance and involvement in fibrosis. The cells were treated with CTGF and TGFβ, to induce overexpression of CTGF (Frazier et al., 1996). Cells treated with CTGF and TGFβ were hypothesized to show enhanced cell growth and motility compared to other treatment groups. In contrast, cells treated with CTGF, TGFβ, and TGFβ inhibitor were hypothesized to show similar growth to untreated cells. By treating with TGFβ and the inhibitor, we were able to observe the importance of TGFβ on CTGF-mediated cell motility and growth in a cell model of wounding. In order to further examine the overexpression of CTGF, a vector including the CTGF gene was constructed to transfect into fibroblast cells. The transfection procedure was tested and validated by cotransfecting CTGF vector with a control plasmid. Gene expression from this control can be quantified with a colorimetric test to determine relative transfection efficiencies between wells. Future directions will include transfecting the vectors into NIH/3T3 cells to observe how overexpressing CTGF using this vector will influence the growth and motility of the fibroblasts. Control(untreated)CTGFandTGFβCTGFandTGFβWith TGFβInhibition D E F A B C J G H II 0 hours 12 hours 24 hours Successful Transfection of NIH/3T3 Cells Ampr 0 20 40 60 80 100 0 6 12 18 24 %ScratchAreaRemaining Time Post-Scratch (Hours) Control CTGF and TGFB CTGF TGFB and Inhibitor Post-Hoc Comparison (24 H) P-Value Control v CTGF and TGFβ *0.050 Control v CTGF, TGFβ and Inhibitor 0.233 CTGF and TGFβ v CTGF, TGFβ and Inhibitor **0.001 K B CTGF pUC19 Empty pUC19 Ladder 3000 6000 A B Ampr pSV β-Gal 6820 bp LacZ SV40 PromoterA 1 2000 400040004000 6000 CTGF pUC19 with CTGF insert 6934 bp XbaI 1 2000 6000 4000 BamHI Cells and Cell Environment: Mouse embryonic fibroblasts (NIH/3T3s) were maintained at 37C and 5% CO2 in Dulbecco’s Modified Eagle Medium (DMEM) with 10% fetal bovine serum and Pen/Strep/Glut. Scratch Tests: Scratch tests were performed in order to simulate cell response in wound healing. Wells were scratched using a p10-100 pipet tip. After scratching, all wells received fresh media with one of three treatments: 1) water and DMSO (control), 2) TGF and CTGF or, 3) TGF, CTGF, and the TGF inhibitor GW788388 (Sigma-Aldrich). Scratch test area was imaged at 40x total magnification. Images were taken at 0, 6, 12, 18 and 24 hours post scratch. ImageJ software (NIH) was used to measure remaining scratch test area from each picture. Factorial analysis of variance (ANOVA) was used to determine whether hour or treatment played a significant role in fibroblast infiltration into the scratch area. Post-hoc Student’s t-tests were used to test for significant differences in remaining scratch area of each treatment at 24 hours (p<0.05 was considered statistically significant). Minitab 17 (Minitab Inc.) was used for all statistical analyses. Vector Construction: In order to create the pUC19/CTGF vector, CTGF was amplified and then double digested along with empty pUC19 using restriction enzymes BamHI and XbaI. The gene and plasmid were ligated and then transformed into E. coli cells. Colonies positive for vector insertion were picked and expanded. pUC19/CTGF vector candidates were digested with BamHI along with empty vector and run on a gel to verify size differences. Successful insertion was further verified with sequencing of ligation junctions and the entire CTGF gene. Sequencing was done at Dartmouth Molecular Biology Core Facility. β-Gal Assay Testing: The pSV-beta-Galactosidase (pSV -Gal) vector was obtained from Promega. Cells were split onto 6 well plates and once they reached 70% confluence, vector was transfected into cells using lipofectamine 2000 (Invitrogen). Treatments included a control with no vector and experimental cotransfections of pSV -Gal and pUC19/CTGF or pSV -Gal and empty pUC19. Cells were harvested 24 hours post- transfection and a β-galactosidase assay was completed to measure transfection efficiency. Figure 1: Representative NIH/3T3 pictures at 0, 12, and 24 hours after scratch testing and quantitation of scratch closure. A-C) Untreated cells at 0, 12, and 24 hours, respectively. D-F) CTGF and TGFβ treated cells at 0, 12, and 24 hours, respectively. G-I) CTGF, TGFβ, and inhibitor treated cells at 0, 12, and 24 hours, respectively. J) Percentage of original scratch area remaining for each treatment over time. K) Results of post-hoc Student’s t-tests at the 24 hour timepoint. p<0.05 was considered significant for all analyses (n=3). Results: A-I) Cells treated with CTGF and TGFβ proteins show greater wound invasion than untreated cells, suggesting increased motility and mitogenic potential of the fibroblast cells. Cells treated with both proteins and the TGFβ inhibitor appeared similar to the control. J) After 24 hours, CTGF and TGFβ treatment resulted in the least scratch wound area remaining. Time (p<0.001), treatment (p=0.001), and the combination of both (p=0.002) significantly influenced the percentage of scratch area remaining as determined by factorial ANOVA. K) At 24 hours, CTGF and TGFβ treatment resulted in significantly less scratch area remaining than the control (p=0.05) and inhibitor treatments (p=0.001). The controls and inhibitor treated cells were not significantly different from one another after 24 hours (p=0.233). Overall, TGF and CTGF treatment increased the speed at which cells infiltrated the scratch area as compared to controls, and addition of a TGF inhibitor reversed this effect. Figure 2: A) Diagram of pUC19 vector with CTGF gene insert. B) CTGF vector and empty pUC19 vector digested with BamHI and run on a gel to check for proper insert size. Results: A) pUC19 vector with a CTGF gene insert was designed to transfect into NIH/3T3 fibroblast cells. B) The size of the band produced after digestion helps confirm that CTGF has been successfully inserted into the vector. Additional analysis by sequencing at the ligation junctions, as well as within the entire gene (not shown), verifies that we have successfully created a vector with the CTGF gene insert. Figure 3: A) Diagram of pSV β-Gal control vector. This vector includes an ampicillin resistance gene and the LacZ gene encoding the β-Galactosidase protein. Expression of this gene is induced in our fibroblasts via an SV40 promoter. B) Absorbance at 405nm of β-Gal assay reactions from cells without vector, cells transfected with pSV β-Gal and pUC19 vector, and cells transfected with pSV β-Gal and CTGF vector (n=1). Results: B) pSV β-Gal control vector was cotransfected with pUC19/CTGF vector or empty pUC19 as a transfection efficiency control. Cells with pSV β-Gal and empty pUC19 or with pSV β-Gal and pUC19/CTGF vector had an absorbance about 7 times and 5.5 times greater than controls, respectively. The LacZ gene is expressed robustly when the pSV β-Gal control vector is transfected with the pUC19 or pUC19/CTGF vector, and both result in an absorbance that is much higher than that of the controls. This suggests that the vectors were successfully transfected into our NIH/3T3 cells. • Compare phenotypes of cells transfected with empty versus CTGF-containing vector • Measure expression of fibrosis-related genes including CTGF, fibronectin, and type III and IV collagens • Perform scratch test to examine differences in wound healing • Examine how CTGF genetic variations impact fibrosis- related phenotypes We would like to thank Plymouth State University, the PSU Research Advisory Council, the PSU Student Research Advisory Council, and the New Hampshire Idea Network of Biological Research Excellence for funding support. We would like to thank the Dartmouth College Molecular Biology Shared Resources Lab for sequencing. We would also like to thank Kimberly Amerson, Jon Bairam, Joel Dufour, Hailey Gentile, Zachary Stevens, Amed Torres, and Alycia Wiggins. 1.Abou-Shady M, Friess H, et al. (2000) Connective tissue growth factor in human liver cirrhosis. Liver 20: 296-304. 2.Ahmed MS, Oie E, et al. (2004) Connective tissue growth factor--a novel mediator of angiotensin II-stimulated cardiac fibroblast activation in heart failure in rats. J Mol Cell Cardiol 36(3): 393-404. 3.Bataller, Ramon., Brenner, David A. (2005) Liver Fibrosis. J Clin Invest 115(2):209-218. 4.Blom, Ingrid E., Goldschmeding, Roel., Leask, Andrew. (2002) Gene Regulation of connective tissue growth factor: new targets for antifibrotic therapy. Matrix Biology 21. 473-482. 5.Brigstock DR (1999) The connective tissue growth factor/cysteine- rich 61/nephroblastoma overexpressed (CCN) family. Endocrine Reviews 20: 189-206. 6.Broughton G, Janis JE, Attinger CE (2006) The Basic Science of Wound Healing. Plastic and Reconstructive Surgery 117: 12S-34S. 7.Chen MM, Lam A, et al. (2000) CTGF expression is induced by TGF- beta in cardiac fibroblasts and cardiac myocytes: a potential role in heart fibrosis. J Mol Cell Cardiol 32(10): 1805-1819. 8.Chuva De Sousa Lopes SM, Feijen A, et al. (2004) Connective tissue growth factor expression and Smad signaling during mouse heart development and myocardial infarction. Developmental dynamics 231(3): 542-550. 9.Dean RG, Balding LC, et al. (2005) Connective tissue growth factor and cardiac fibrosis after myocardial infarction. Journal of Histochemistry and Cytochemistry 53: 1245-1256. 10.Diegelmann RF, Evans MC (2004) Wound healing: An overview of acute, fibrotic and delayed healing. Frontiers in Bioscience 9: 283-289. 11.Doherty, H (2010) The Role of Quantitative Variations in Connective Tissue Growth Factor Gene Expression in Cardiac Hypertrophy and Fibrosis. Chapel Hill :11-12. 12.Fonseca C, Lindahl GE, et al. (2007) A polymorphism in the CTGF promoter region associated with systemic sclerosis. New England Journal of Medicine 357: 1210-1220. 13.Frazier K, Williams S, et al. (1996) Stimulation of fibroblast cell growth, matrix production, and granulation tissue formation by connective tissue growth factor. Journal of Investigative Dermatology 107: 404-411. 14.Gurtner, G. C., Werner, S., Barrandon, Y., & Longaker, M. T. (2008). Wound repair and regeneration. Nature, 453(7193), 314-321. 15.Igarashi A, Nashiro K, et al. (1995) Significant correlation between connective tissue growth factor gene expression and skin sclerosis in tissue sections from patients with systemic sclerosis. Journal of Investigative Dermatology 105: 280-284. 16.Igarashi A, Okochi H, et al. (1993) Regulation of connective tissue growth factor gene expression in human skin fibroblasts and during wound repair. Molecular Biology of the Cell 4: 637-645. 17.Ito Y, Aten J, et al. (1998) Expression of connective tissue growth factor in human renal fibrosis. Kidney international 53: 853-861. 18.Lasky J, Ortiz L, et al. (1998) Connective tissue growth factor mRNA expression is upregulated in bleomycin-induced lung fibrosis. American Journal of Physiology: 275(2 Pt 1): L365-371. 19.Leask A, Abraham DJ (2003) The role of connective tissue growth factor, a multifunctional matricellular protein, in fibroblast biology. Biochemistry and Cell Biology 81(6): 355-363. 20.Matsui Y, Sadoshima J (2004) Rapid upregulation of CTGF in cardiac myocytes by hypertrophic stimuli: implication for cardiac fibrosis and hypertrophy. Journal of molecular and cellular cardiology 37(2): 477-481. 21.Minitab 17 Statistical Software (2010). State College, PA: Minitab, Inc. (www.minitab.com 22.Mori T, Kawara S, et al. (1999) Role and interaction of connective tissue growth factor with transforming growth factor‐β in persistent fibrosis: A mouse fibrosis model. Journal of cellular physiology 181: 153-159. 23.Ohnishi H, Oka T, et al. (1998) Increased expression of connective tissue growth factor in the infarct zone of experimentally induced myocardial infarction in rats. J Mol Cell Cardiol 30: 2411–2422. 24.Paradis V, Dargere D, et al. (1999) Expression of connective tissue growth factor in experimental rat and human liver fibrosis. Hepatology 30: 968-976. 25.Phan SH. (2002) The myofibroblast in pulmonary fibrosis. Chest T122(6): 286S-289S. 26.Ponticos M, Holmes AM, et al. (2009) Pivotal role of connective tissue growth factor in lung fibrosis: MAPK-dependent transcriptional activation of type I collagen. Arthritis & Rheumatism 60: 2142-2155. 27.Porter KE, Turner NA (2009) Cardiac fibroblasts: at the heart of myocardial remodeling. Pharmacology & therapeutics 123(2): 255-278. 28.Rasband, W.S., ImageJ, U. S. National Institutes of Health, Bethesda, Maryland, USA, http://imagej.nih.gov/ij/, 1997-2016. 29.Shi-Wen X, Leask A, Abraham D (2008) Regulation and function of connective tissue growth factor/CCN2 in tissue repair, scarring and fibrosis. Cytokine & growth factor reviews 19: 133-144. 30.Sonnylal S, Shi-Wen X, et al. (2010) Selective expression of connective tissue growth factor in fibroblasts in vivo promotes systemic tissue fibrosis. Arthritis & Rheumatism 62: 1523-1532. 31.Sun Y, Zhang JQ, et al. (2000) Cardiac remodeling by fibrous tissue after infarction in rats. J Lab Clin Med 135(4): 316-323. 32. Wynn, Thomas A. (2007) Common and unique mechanisms regulate fibrosis in various fibroproliferative diseases. Journal of Clinical Investigation 117: 524-529. 33.Wynn TA (2008) Cellular and molecular mechanisms of fibrosis. Journal of Pathology 214: 199-210.