1. TYPES OF MEDICAL STUDIES
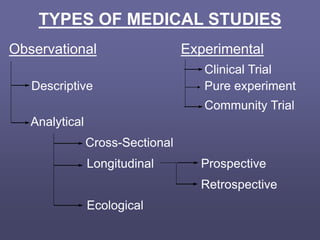
Observational Experimental
Clinical Trial
Descriptive Pure experiment
Community Trial
Analytical
Cross-Sectional
Longitudinal Prospective
Retrospective
Ecological
2. • Investigator exercises control over
allocation of exposure
• More powerful than observational studies
for testing etiological hypotheses
• For ethical reasons the possibilities of
conducting experiments in humans is
limited
Experimental Studies
4. Clinical trial
- Gold standard in medicine – provides the
greatest justification for concluding causality
and is subject to the least number of problems or
biases
- Involves people
- Controlled trials are studies in which the
experimental dug or procedure is compared with
another drug or procedure, sometimes a placebo
and sometimes the previously accepted
treatment
- Uncontrolled trials – no comparison group
5. Controls
- Independent concurrent controls
- Double-blind trials
- Trials with self-controls
- Trials with external (historical) controls
6. Did investigator
assign exposures?
Observational Study
Experimental Study
comparison group?
randomize allocation?
Randomized
Controlled
Trial
Non-
Randomized
Controlled
Trial
Analytical
Study
Descriptive
Study
direction?
Cross-
sectional
Study
Case-
Control
Study
Cohort
Study
no
yes
yes no yes no
7. Observational Studies
• Investigator observes occurrence of
condition/s in “self”-assigned groups of
people
• Often most practical and feasible
• Carried out in more natural settings
• Less control over study situation
results more susceptible to distorting
influence
8. Descriptive Survey
• Sets out to describe a situation
ex. Distribution of depression in a
population in relation to sex, age and other
characteristics
Analytical Survey
• Sets out to test hypotheses or detect
associations
ex. Identify factors that explain higher rates
of depression among women
9. OBJECTIVES OF DESCRIPTIVE
EPIDEMIOLOGiC STUDIES
• To permit evaluation of trends in health and
disease and comparisons among countries and
subgroups within countries; this objective
includes monitoring of known diseases as well
as the identification of emerging problems
• To provide a basis for planning, provision, and
evaluation of health services
• To identify problems to be studied by analytic
methods and suggest areas that may be fruitful
for investigation
(Friis & Seelers, 1999)
12. Prospective Study
• The first step in a prospective study
design is to identify the relevant group/s
of people and collect information about
their exposure history.
• We then follow these people over time
and measure the incidence of the
outcome/s of interest.
15. Cohort study of British Doctors
Current smoker Non smoker
(1951) (1951)
Yes a b
Death of lung cancer 4180 224
No c d
45820 39776
# at beginning of study 50000 40000 90000
17. The main limitation of the
prospective design is the time and
cost involved especially when
studying chronic diseases that
may only become apparent years
after the exposure/s of interest
or may require years of exposure
to “cause” the outcome.
18. Example:
To investigate the risk of bowel cancer
(annual incidence = 100-300/100,000
persons) would require a cohort of
thousands of individuals to be followed for
10-15 years in order to identify a
sufficient number of outcomes for a
reliable estimation of the association.
19. Historical Prospective Design
• An alternative strategy for the concurrent
prospective study design in order to reduce
time and costs.
• This design requires identifying a defined
cohort from some time in the past. The follow-
up period is the time that elapsed since
exposure status was determined until the
present.
• Incidence and risk measures can be estimated
in the same manner as in a concurrent
prospective study.
20. Historical Prospective Design
Particularly useful when the exposure under
investigation is “unique” in some way. e.g.,
occurred only in the past, occurred in specific
group of people. Therefore this design is
often applied to the study of acute
environmental exposures.
Example: thyroid cancer risk among people
exposed to the Chernobyl nuclear-reactor
accident
21. Historical Prospective Design
Possible sources of information about
exposure status:
• industrial worker records
• military records
• insurance companies or health care
provider companies
• registries of persons receiving specific
medical treatment
22. Historical Prospective Design
• Often difficult to obtain information
about other exposures in the cohort.
• Sometime difficult to obtain
comprehensive list of those who
experienced the outcome (less
problematic in a mortality study)
23. Historical and concurrent cohort studies
PAST PRESENT FUTURE
Historical cohort
Cases Follow-up
assembled
Concurrent cohort
Cases Follow-up
assembled
24. Historical Cohort Study
Non-concurrent Cohort Study
Retrospective Cohort Study
Retrolective Study
Example: X-rays among TB patients and lung cancer
2000
1985
1945
1925
TB
treatment
Follow-up period
P
r
e
s
e
n
t
25. Time
Direction of Inquiry
Start with:
EXPOSED
CASES
(people with
EXPOSED disease)
POPULATION
EXPOSED
CONTROLS
(people without
EXPOSED disease)
Design of a CASE-CONTROL Study
27. comparative strengths of cohort and
case-control studies
CASE-CONTROL
• Well suited to study rare
outcomes
• Can easily study multiple
exposures
• Efficient if long delay
between exposure and
outcome
COHORT
• Well suited to study rare
exposures
• Can easily study multiple
outcomes
• Provides direct measure
of risk of outcome
among exposed and
unexposed persons
• Begins with healthy
persons thereby
preventing “selective
survival” bias
28. comparative limitations of cohort
and case-control studies
CASE-CONTROL
• Inefficient for rare
exposures
• Not well suited to study
multiple outcomes
• Unable to provide data
on absolute risk
• Time sequence of
exposure and outcome
can be unclear
COHORT
• Inefficient for rare
outcomes
• Not well suited to study
multiple exposures
• Difficult if long delay
between exposure and
outcome*
• Lost-to-follow-up
problem
• Can be costly*
29. comparative limitations of cohort
and case-control studies
CASE-CONTROL
• Relies on information
about past exposures
that may be prone to
bias
COHORT
• Assessment of exposure
status may influence
participant’s behavior
• Changing diagnostic
criteria may introduce
bias
30. Design of a CROSS-SECTIONAL Study
Begin with:
DEFINED
POPULATION
gather data on exposure and disease
Exposed Exposed Exposed Exposed
Disease Disease Disease Disease
31. Cross Sectional Study
• Involves a random sample of a dynamic population
• Efficient for describing characteristics of the population
• Efficient for generating new hypotheses
• Provides prevalence estimates of the outcome
• Not useful design for determining causal effects
• Not efficient for studying rare outcomes or those
of short-duration
• Repeat cross-sectional surveys are useful for
assessing the impact of a service
• Relatively inexpensive and quick
32. • Cannot provide direct estimates of risk
• Difficult to interpret temporality between
exposure and outcome
Cross Sectional Study