Call Girls Horamavu WhatsApp Number 7001035870 Meeting With Bangalore Escorts
Liver abscess
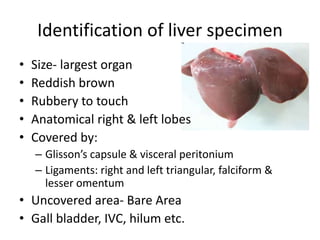
1. Identification of liver specimen
• Size- largest organ
• Reddish brown
• Rubbery to touch
• Anatomical right & left lobes
• Covered by:
– Glisson’s capsule & visceral peritonium
– Ligaments: right and left triangular, falciform &
lesser omentum
• Uncovered area- Bare Area
• Gall bladder, IVC, hilum etc.
2.
3. Identification of liver specimen..
• Cut surface/partial hepatectomy:
– Reddish brown/ tan pink/fleshy parenchyma
– Capsular surface smooth
– Multiple cut bile ducts:
• Variable sizes
• Bile stained
6. Liver abscess
• Space occupying lesions (SOL)
• Collection of:
– Pyogenic material- frank pus
– “Anchovy sauce” pus
– Greenish pus
• Number of SOL:
– Solitary
– Multiple
7.
8. Liver abscess
• What types of liver abscess you know?
• Commonly 2 types:
– Amoebic
– Pyogenic
• Others :
– Tubercular
– fungal
10. Liver abscess
• Aetiology of amoebic liver abscess?
1. Endemic to Entamoeba
Histolytica - tropical countries
Indian subcontinent & Africa
4. Diabetes Mellitus
2. Chronic alcohol intake 5. Immunosuppressed state
3. Liver cirrhosis 6. Reproductive age females
11. Liver abscess
• Aetiology of pyogenic liver abscess?
1. Biliary sepsis:
a. Empyema gallbladder.
b. Cholangitis.
c. After biliary tract surgery.
d. Instrumentation.
4. Super added infections:
a. Amoebic liver abscess.
b. Hydatid cyst.
2. Portal vein sepsis:
a. Appendicitis.
b. Diverticulitis.
c. any severe abdominal sepsis.
5. Cryptogenic liver abscess—No
identified primary infection. (m.c.c.)
3. Distant infections:
a. Pneumonia.
b. Upper U.T.I.
c. Endocarditis.
6. Trauma- becoming common cause
7. Diabetics
12. Liver abscess
• What is the clinical presentation?
• Amebic abscess- more common in males
• Symptoms:
– Pain- right upper abdomen (throbbing)
– Fever, with rigors with malaise
– Occasionally jaundice
– May be associated dysentery
– Weakness
– Decreased appetite/ loss of weight
– If complicated- difficulty breathing, fainting etc.
13. Liver abscess
• What signs can be found?
• Signs:
– Tenderness-right hypochondrium
– Intercostal tenderness- right
– Hepatomegaly: smooth, soft
– Icterus
– Signs of complications:
• Peritonitis, pleural effusion, ascitis, bronchopleural
fistula etc
– Signs of sepsis
14. Liver abscess
• What are the complications of liver abscess?
• Pleural effusion- right sided
• Ascites
• Jaundice
• Rupture-
– brochopleural fistula/ empyema (m.c.)
– peritonitis
– Retroperitonial abscess
– Subphrenic abscess
– Cardiac temponade
– Into intestines & skin (amoebic cutis)
15. Liver abscess
• What are other complications of liver abscess?
• Superinfection of amoebic abscess
• Budd Chiary syndrome
• Liver failure / Hepatic encephalopathy
• Septicemia, later shock
• Death
16. Liver abscess
• How does amoebic liver abscess develop?
1. Mature cyst (faeces)
2. Contaminate food & water
3. Ingestion of cyst
4. Pass through stomach undamaged
5. Cyst wall lysis occurs by trypsin (alkaline medium)
6. Excystation
7. Release of quadrinucleate amoebae
8. Metacyst trophozoites formed
9. Habitat in crypts of caecum commonly, often in sigmoid
colon as to form trophozoites.
17.
18.
19. Liver abscess
• How diagnosis is made?
• Ultrasound abdomen is diagnostic
– Space occupying lesion
– Altered echogenecity (anechoic, hypoechoic)
– Site, size, number & nature
– Associated complications
• CECT abdomen
• CXR-
– raised right hemidiaphragm, effusion, soft tissue
shadow
20. Liver abscess
• How do you investigate a patient with history
suggestive of liver abscess?
• Blood tests-
– CBC: may show low Hb, raised TLC
– LFT: altered bilirubin, liver enzymes, albumin
– Prothombin Time/INR: can be raised
• USG abdomen
• CXR
• CECT – chest & abdomen
21.
22. Liver abscess
• How do you investigate a patient with history
suggestive of liver abscess?
• Amoebic serology: ELISA/ Indirect
haemagglutination/ gel diffusion tests/
counter immuno-electrophoresis
• USG guided spirated Pus: culture & sensitivity
• Colonscopy/sigmoidoscopy: amoebic
typhilitis/ active ulcers- showing trophozoites
23. Liver abscess
• What is the treatment?
• Drugs:
– Amoebic abscess:
• Metronidazole- Tab. 800mg TDS/ Inj. 750mg i.v. TDS x 10d
• Or Tinidazole, Secnidazole, Ornidazole (nitroimidazoles)
• To control/ prevent secondary infection- cefotaxime,
ciprofloxacin, amoxycillin
• Cyst eradicators/ luminal amoebicides- Diloxanate furoate,
iodoquinol, paromonycin
• Other drugs- dihydroemetine, chloroquine (tissue
amoebicides)
24. Liver abscess
• What is the treatment?
• Drugs:
– Pyogenic liver abscess:
• Systemic antibiotics- Combination of third generation
cephalosporin+ metronidazole
• USG guided drainage:
– Percutaneous aspiration (therapeutic)
– Percutaneous Indwelling catheter drainage
• Open drainage
• Treat primary cause in case of pyogenic abscess
25. Liver abscess
• When & how is percutaneous drainage of liver
abscess done?
• Indication:
– Abscess not responding symptomatically to drugs
– Large abscess (>200cc, >10cm- RT)
– Any size in caudate lobe
– Seronegative abscess
– Abscess in pregnancy
– Diagnostic: in case of dilemma
26. Liver abscess
• When & how is percutaneous drainage of liver
abscess done?
• Prerequisite:
– Clinical diagnosis
– Patient’s consent
– Normal coagulation profile
– Abscess accessible
27. Liver abscess
• When & how is percutaneous drainage of liver
abscess done?
• Technique :
– Under real time USG guidance
• Wide bore needle with 10-50cc syringe
• Catheter tube: red rubber/malecot, pigtail catheter
– Introduced through abdomen (preferrably) or
intercostal space, under local anesthesia & sterility
– Pus sent: C/S, cytology, trophozoite detection
28. Liver abscess
• Is surgery even required?
• What are the indications?
• Non responsive (symptomatically) to
percutaneous drainage i.e. failure
– Thick pus
– Multiloculated abscess
– Multiple abscess
• Complications- rupture
• What is the approach? Transperitonial
29. Liver abscess
• What follow up advice will you give?
• Abstain from alcohol intake
• Complete course of drugs
• Repeat LFT
• Repeat USG abdomen, if symptoms recur or do
not resolve
30. Liver abscess
• What is the prognosis?
• Mortality in amoebic liver abscess is 4% & rises
with rupture esp. pericardia (30%)
• Poor prognostic factors
Rupture Diabetes
Serum bilirubi n >3.5 mg% Cirrhosis
Serum albumin <2.0 g/dl Multiple abscesses
Liver failure,, anaemia Volume of abscess >500 ml
Tinidazole 600 mg BD dose for 5 days.
• IV or oral antibiotics are essential to control secondary
infection (cefotaxime, ciprofloxacin, amoxycillin).
(Small abscesses < 3 cm respond to drugs).
• Other drugs:
1. Injection dihydroemetine 1.5 mg/kg/day IM for
5 days should be given under cardiac monitoring.
2. Chloroquine 250 mg BD given for 10-14 days.
Drugs used for amebic infection
• Metronidazole, Tinidazole, Secnidazole, Ornidazole
• Dihydroemetine injection
• Chloroquine, tetracycline
• Diloxanate furoate, iodoquinol, paromonycin—as
cyst eradicators
Tinidazole 600 mg BD dose for 5 days.
• IV or oral antibiotics are essential to control secondary
infection (cefotaxime, ciprofloxacin, amoxycillin).
(Small abscesses < 3 cm respond to drugs).
• Other drugs:
1. Injection dihydroemetine 1.5 mg/kg/day IM for
5 days should be given under cardiac monitoring.
2. Chloroquine 250 mg BD given for 10-14 days.
Drugs used for amebic infection
• Metronidazole, Tinidazole, Secnidazole, Ornidazole
• Dihydroemetine injection
• Chloroquine, tetracycline
• Diloxanate furoate, iodoquinol, paromonycin—as
cyst eradicators
Tinidazole 600 mg BD dose for 5 days.
• IV or oral antibiotics are essential to control secondary
infection (cefotaxime, ciprofloxacin, amoxycillin).
(Small abscesses < 3 cm respond to drugs).
• Other drugs:
1. Injection dihydroemetine 1.5 mg/kg/day IM for
5 days should be given under cardiac monitoring.
2. Chloroquine 250 mg BD given for 10-14 days.
Drugs used for amebic infection
• Metronidazole, Tinidazole, Secnidazole, Ornidazole
• Dihydroemetine injection
• Chloroquine, tetracycline
• Diloxanate furoate, iodoquinol, paromonycin—as
cyst eradicators
Tinidazole 600 mg BD dose for 5 days.
• IV or oral antibiotics are essential to control secondary
infection (cefotaxime, ciprofloxacin, amoxycillin).
(Small abscesses < 3 cm respond to drugs).
• Other drugs:
1. Injection dihydroemetine 1.5 mg/kg/day IM for
5 days should be given under cardiac monitoring.
2. Chloroquine 250 mg BD given for 10-14 days.
Drugs used for amebic infection
• Metronidazole, Tinidazole, Secnidazole, Ornidazole
• Dihydroemetine injection
• Chloroquine, tetracycline
• Diloxanate furoate, iodoquinol, paromonycin—as
cyst eradicators
Tinidazole 600 mg BD dose for 5 days.
• IV or oral antibiotics are essential to control secondary
infection (cefotaxime, ciprofloxacin, amoxycillin).
(Small abscesses < 3 cm respond to drugs).
• Other drugs:
1. Injection dihydroemetine 1.5 mg/kg/day IM for
5 days should be given under cardiac monitoring.
2. Chloroquine 250 mg BD given for 10-14 days.
Drugs used for amebic infection
• Metronidazole, Tinidazole, Secnidazole, Ornidazole
• Dihydroemetine injection
• Chloroquine, tetracycline
• Diloxanate furoate, iodoquinol, paromonycin—as
cyst eradicators
Tinidazole 600 mg BD dose for 5 days.
• IV or oral antibiotics are essential to control secondary
infection (cefotaxime, ciprofloxacin, amoxycillin).
(Small abscesses < 3 cm respond to drugs).
• Other drugs:
1. Injection dihydroemetine 1.5 mg/kg/day IM for
5 days should be given under cardiac monitoring.
2. Chloroquine 250 mg BD given for 10-14 days.
Drugs used for amebic infection
• Metronidazole, Tinidazole, Secnidazole, Ornidazole
• Dihydroemetine injection
• Chloroquine, tetracycline
• Diloxanate furoate, iodoquinol, paromonycin—as
cyst eradicators
Tinidazole 600 mg BD dose for 5 days.
• IV or oral antibiotics are essential to control secondary
infection (cefotaxime, ciprofloxacin, amoxycillin).
(Small abscesses < 3 cm respond to drugs).
• Other drugs:
1. Injection dihydroemetine 1.5 mg/kg/day IM for
5 days should be given under cardiac monitoring.
2. Chloroquine 250 mg BD given for 10-14 days.
Drugs used for amebic infection
• Metronidazole, Tinidazole, Secnidazole, Ornidazole
• Dihydroemetine injection
• Chloroquine, tetracycline
• Diloxanate furoate, iodoquinol, paromonycin—as
cyst eradicators
Tinidazole 600 mg BD dose for 5 days.
• IV or oral antibiotics are essential to control secondary
infection (cefotaxime, ciprofloxacin, amoxycillin).
(Small abscesses < 3 cm respond to drugs).
• Other drugs:
1. Injection dihydroemetine 1.5 mg/kg/day IM for
5 days should be given under cardiac monitoring.
2. Chloroquine 250 mg BD given for 10-14 days.
Drugs used for amebic infection
• Metronidazole, Tinidazole, Secnidazole, Ornidazole
• Dihydroemetine injection
• Chloroquine, tetracycline
• Diloxanate furoate, iodoquinol, paromonycin—as
cyst eradicators