
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Bacterial keratitis
Similar to Bacterial keratitis (20)
Recently uploaded
Recently uploaded (20)
Bacterial keratitis
- 2. Contents Aetiology Pathogenesis Risk factors Clinical features Treatment Management Complication
- 3. Aetiology The Organisms that produce toxins causing tissue death and pus formation in the Cornea. StreptococciStaphylococcus aureus Pseudomonas aeruginosa Bacteria commensal of the upper respiratory tract commensal of the nares, skin and conjunctiva commensal of the gastrointestinal tract Normal Habit Infections with streptococci are often aggressive. present with a focal and fairly well- defined white or yellow–white infiltrate. The infection is typically aggressive and is responsible for over 60% of contact lens-related keratitis. Disease
- 4. Risk Factors Contact lens wear Trauma Ocular surface disease Other factors
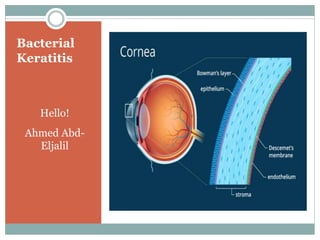
- 5. Pathogenesis 1- Progressive stage : A- Start with localized necrosis of the anterior layers of cornea “Epithelium & Bowman’s membrane”. Necrotic tissue partially cast off into the conjunctival sac and adheres to ulcer. B- Saucer-shaped Ulcer due to swelling of the surrounding Corneal lamellae and project . C-Surrounding area becomes packed with leucocytes as gray zone “ground glass appearance”. D- some toxins produced by the causative organisms cause irritation of the iris and ciliary body resulting in “ kerato-uveitis”. Hypopyon
- 6. Regressive stage PNL in the cornea ,Dissolve The necrotic tissues . Infiltration and swelling start disappear. Floor and edges of the ulcer become smooth and transparent. Superficial vascularization from limbus to restore tissue loss and supply Antibodies.
- 7. Healing stage Regeneration of Collagen and formation of fibrous tissue . Newly fibers not arranged regular and cause reflective error. Mild opacity due to Collagen remodeling Formed scar are opaque . Bowman’s membrane never regenerates. Formed scar tissue fills the tissue gap.
- 8. Clinical Features Symptoms : Diminution of Vision ,pain, photophobia, Ciliary injection , blurred vision and mucopurulent or purulent discharge.
- 9. Clinical Features Signs : Lid oedema. epithelial defect with infiltrate involving a larger area. Hypopyon. Chemosis. Loss corneal Lustre Ulcer can stained by 1% of Fluorescein sodium. Severe ulceration may lead to descemetocele formation and perforation, particularly in Pseudomonas infection .
- 11. Investigations 1-Corneal scraping Conjunctival swab Contact lens cases Gram staining
- 12. Culture media for corneal scrapings
- 13. Complication Corneal scarring “Nebula , Macula, Leucoma” Corneal facet formation. Keratoctasia. Descemetocele Perforation
- 14. Treatment 1-General considerations 2-Local therapy 3-Systemic Therapy
- 15. General considerations Hospital admission Discontinuation of contact lens wear is mandatory A clear plastic eye shield Decision to treat
- 16. Local therapy Can achieve high tissue concentration and initially should consist of broad-spectrum antibiotics that cover most common pathogens. Antibiotic monotherapy “Ciprofloxacin or ofloxacin”. Antibiotic duo therapy “combination of two fortified antibiotics, typically a cephalosporin and an aminoglycoside”. Subconjunctival antibiotics. Mydriatics. Steroids “are contraindicated until reepithelizition” reduce host inflammation, improve comfort, and minimize corneal scarring.
- 17. Systemic therapy Systemic antibiotics are not usually given, but may be appropriate in the following circumstances: 1-Potential for systemic involvement 2-Severe corneal thinning 3-Scleral involvement
- 18. Management of apparent treatment failure If no improvement. There’s no need to change the initial therapy if this has induced a favorable response. However, if Improvement still not accomplished. re-scraping performed with inoculation on a broader range of media. If cultures remains negative, it might be necessary to perform a corneal biopsy for histology and culture. Excisional keratoplasty.
Editor's Notes
- Contents Pathogenesis Risk factors Clinical picture “Presentation” Treatment Mangement Perforation