
Recommended
Recommended
More Related Content
Similar to ASD Echolalia Treatment Review
Similar to ASD Echolalia Treatment Review (20)
More from AbramMartino96
More from AbramMartino96 (20)
Recently uploaded
Recently uploaded (20)
ASD Echolalia Treatment Review
- 1. Mastering Scholarly Writing Remove or Replace: Header Is Not Doc TitleOutline Worksheet Introduction In paper An opening statement that frames your focus Autism self-management treatment without child's vocalization. Inappropriate language replacement with verbal labeling will be more functional than the normal verballing. Who The psychologists are working towards developing a stimuli language that will help autistic students improve their learning and responding skills. Echolalia's language has always responded inappropriately to questions that should replace verbal representation for more effectiveness. What Children with autism are normally rejected and treated differently from others. Standardizing their learning skills or rather simplifying their response through verbal stimulation will, in turn, raise self-management. When The program generalization and maintenance will take place in phases. They are evolving from the initial settings to the new vocalization. Where
- 2. The research will be conducted in a wide range to ensure more participants are reached out. Why? The intended project will ease communication between autism- affected children and others as well as between themselves. Body Paragraph 1 In paper Topic sentence Coming up with the visual language entails the incorporation of knowledge from the physician to the verbal developer. Observation 1 In an experiment to test the language, the sequence wording in a sentence or a question must be repeated for emphasis regardless of verbalization. Support 1 Though verbalization may have considered most accurate concerning autism, errors may occur, which may amount to the incorrect response. Therefore, the tutor must proofread the question to ensure correctness. A combination of correct and incorrect verbiage will add up to an incorrect and inappropriate presentation. Conclusion The tutor should go through the verbalized questions to ensure no errors may lead to incorrect responses. This will improve the efficiency and effectiveness of audiotaped or videos as intended. Body Paragraph 2
- 3. In paper Topic sentence Young children diagnosed with autism made it necessary to come up with some ways for self-development. Observation 1 From the research, communication improvement will improve their learning skills and how the affected interact with other children. Autism children are frequently discriminated against due to a lack of mutual understanding. Support 1 On the conducted research, according to Karl, his module went through upon the third trial. This is a positive indication that verbalization can be depended upon when questioning. Conclusion Though the stimuli differed from one participant to the other, at least there is a mutual language used by both the tutor and the respondent. This indicates a positive step towards verbalization. Body Paragraph 3 In paper Topic sentence It's essential to note that it can lead to communication breakdown on echolalia treatment, thus causing stigmatization in autism-affected children. Observation 1
- 4. Autism Spectrum Disorder(ASD) can be reduced by treatment intervention, especially when examined at an earlier stage. Therefore, to enhance the treatment, participant features, echolalia type, research, and design indicators must be considered before prescribing any treatment. Support 1 Although there is no single treatment that can be fully described, physicians often combine several methods to achieve the set goal. After behavior analysis, the treatment endorsed is evaluated according to the despondence, mainly in visual cues and verbal modeling. Conclusion Due to the lack of a specific treatment, medics should examine the autism and describe the type of treatment to the patient. A follow-up on the method used is also necessary. Conclusion In paper Restatement of thesis statement The main aim is to attain a common verbalized method that can be recognized internationally and used during the examination. The method should also ensure communication between autism and other people. Summary of introduction (who, what, when, where, why, and how) 1 or two sentences For the research's success, the intended purpose, participant, research methods, and time must be observed. Summary of body paragraph 1
- 5. Dealing with autism disorder entails a collaboration from medics, parents, and the affected kids. This will help in verbalization or echolalia destruction and self-development and building self-esteem in the young affected children. Summary of body paragraph 2 Eradicating stigmatization among young children diagnosed with autism is the main goal. However, attaining a common language is complicated due to different responses from various participants. Thus verbalization stimuli must be tested regularly before approval as the official examination language. Summary of body paragraph 3 Through teamwork, the intended verbalization will work. This entails awareness through mass education and special training programs to the affected. Overall ending thought/sentence for the reader Society should learn to embrace and appreciate children with autism; this will reduce stigmatization. Engaging them in daily activism and motivation will boost their self-esteem as they are no less human beings. Learning verbalization to enhance communication is also necessary. � 1 4
- 6. REVIEW PAPER Treatment of Echolalia in Individuals with Autism Spectrum Disorder: a Systematic Review Leslie Neely1 & Stephanie Gerow2 & Mandy Rispoli3 & Russell Lang4 & Nathan Pullen4 Received: 15 October 2015 /Accepted: 25 November 2015 /Published online: 4 December 2015 # Springer Science+Business Media New York 2015 Abstract Echolalia can lead to communication breakdowns that increase the likelihood of social failure and stigmatization in children with autism spectrum disorder (ASD). In an effort to facilitate evidenced-based intervention and inform future research, this systematic review analyzes peer-reviewed stud- ies involving the treatment of echolalia in individuals with ASD. Using predetermined inclusion criteria, a total of 11 studies were identified, reviewed, and summarized in terms of the following: (a) participant characteristics (e.g., verbal and cognitive functioning), (b) type of echolalia (e.g., delayed or immediate), (c) intervention procedures, (d) intervention outcomes, (e) maintenance and generalization of outcomes, and (f) research design and other indicators of rigor (i.e., cer - tainty of evidence). Nine studies successfully reduced echola- lia in a total of 17 participants. However, only six of those nine studies met criteria to be classified as providing the highest level of certainty (i.e., conclusive). The findings of this review suggest that a number of treatment options can be considered promising practices for the treatment of echolalia in children with ASD. Although no single treatment package can be de- scribed as well-established evidence-based practice, all 11 studies involved behavior analytic intervention components, suggesting strong support for operant-based treatments. In
- 7. particular, behavior analytic interventions demonstrating conclusive levels of evidence included cues-pause-point, dif- ferential reinforcement of lower rates of behavior, script train- ing plus visual cues, and verbal modeling plus positive rein- forcement for appropriate responses. Implications for practi- tioners and directions for future research are offered. Keywords Autism spectrum disorder . Echolalia . Treatment . Systematic review Autism spectrum disorder (ASD) is a developmental disorder characterized by deficits in social communication skills and excesses in repetitive and restrictive patterns of behaviors (Diagnostic and Statistical Manual of Mental Disorders [5th ed.; DSM-5]; American Psychiatric Association [APA] 2013). The combination of behavioral excesses and deficits can man- ifest as a repetitive, restricted pattern of vocal behavior called echolalia (Stribling et al. 2007). Echolalia is typically defined as the socially awkward or inappropriate verbatim repetition of part or all of a previously spoken utterance (Karmali et al. 2005; Stribling et al. 2007; Valentino et al. 2012). The initial utterance, that is then repeated, may come from another per- son in the environment or from a recording (television or audio source) and maybe immediate or delayed. Immediate echolalia occurs when the latency between initial utterance and repetition is within a few seconds, whereas delayed echolalia occurs when the time between the initial utterance and the repetition involves longer durations, inclusive of repetitions occurring days after the initial utterance being echoed (Foxx et al. 2004; Hetzroni and Tannous 2004). Another form of echolalia is palilalia. Palilalia involves the repeating of one’s own words in a quiet whispered voice immediately following the initial typical volume utterance (Karmali et al. 2005).
- 8. * Leslie Neely [email protected] 1 Department of Educational Psychology, The University of Texas at San Antonio, 501 W. Cesar E. Chavez Blvd., San Antonio, TX 78207-4415, USA 2 Texas A&M University, College Station, TX, USA 3 Purdue University, West Lafayette, IN, USA 4 Texas State University, San Marcos, TX, USA Rev J Autism Dev Disord (2016) 3:82–91 DOI 10.1007/s40489-015-0067-4 http://crossmark.crossref.org/dialog/?doi=10.1007/s40489-015- 0067-4&domain=pdf Although language repetition is part of typical child development (Howlin 1982). some children with ASD en- gage in echolalia that persists past the early childhood developmental period (Barrera and Sulzer-Azaroff 1983; Neely 2014; Fay 1969). In addition, children with ASD often engage in echolalia that lacks social context Lovaas et al. 1973) and occurs at a higher rate than in typically developing children (Fay 1973). Echolalia may (a) complicate educational programs de- signed to improve speech, (b) contribute to communication breakdowns, (c) increase the likelihood of social failure or stigmatization, and (d) increase the risk of challenging behav- ior (Light et al. 1998; Valentino et al. 2012). For example, Valentino et al. (2012) identified a 3-year-old male with ASD who repeated the instruction Bsay^ during echoic train- ing. The immediate echolalia was interfering with instruction
- 9. and complicating the educational program aimed at teaching the child to tact. Previous research aimed at identifying the operant function of echolalia suggests that the complete range of functions found to maintain other behaviors (e.g., automatic reinforcement, socially mediated positive reinforcement, and socially mediated negative reinforcement) may also reinforce and maintain echolalia (Goren et al. 1977; Healy and Leader 2011). A descriptive review by Kavon and McLaughlin (1995) identified two interventions with preliminary support for the treatment of echolalia (i.e., cues-pause-point and more general verbal prompting interventions). Cues-pause-point is a behav- ioral intervention that has been evaluated for the treatment of immediate echolalia. Cues-pause-point was introduced by McMorrow and Foxx (1986) in their treatment of a 21-year- old male with ASD. The cues-pause-point intervention con- sists of a trainer providing a visual cue to the learner to remain silent (cue). The trainer then maintains the visual cue while providing instructions about the upcoming teaching session. The trainer poses a question and provides a short pause fol- lowing the question (pause). Finally, the trainer points to a card to prompt the learner to verbalize the answer to the ques - tion (point). For example, to teach the individual with ASD to respond appropriately to the question, BWhat is your name?,^ the trainer held up an index finger to cue silence (cue), stated, BI’m going to ask you some questions, do your best to answer them correctly^ (pause), asked the question, pointed to a card with the person’s name prompting the correct response (point), and then provided reinforcement contingent on the correct response. Following the initial study by McMorrow and Foxx, follow-up studies extended the procedure to indi- viduals with less developed language skills (McMorrow et al. 1987) and individuals with intellectual disabilities (Foxx, Faw, McMorrow, Kyle, & Bittle 1988) and then demonstrated that reductions of echolalia following cues-pause-point could
- 10. be maintained up to 57 months following the cessation of the intervention (Foxx and Faw 1990). Kavon and McLaughlin’s (1995) review categorized the remaining interventions as verbal prompting interventions. Studies in that category used a combination of reinforcement, prompting, and error correction to reduce echolalia but did not utilize the more specific sequence of cues-pause-point (e.g., Freeman et al. 1975; Lovaas 1977). For example, Freeman et al. (1975) used positive reinforcement for correct responding to questions and an error prevention procedure (consisting of interrupting the echolalia) to treat the echolalia of a 5-year-old male with autism. The intervention produced decreases in echolalia that maintained following the with- drawal of intervention. Although the review by Kavon and McLaughlin provides evidence in support of these interven- tions, additional studies have emerged over the last 20 years and an updated systematic review appears warranted. Therefore, the purpose of this review is to update and ex- tend the previous review by Kavon and McLaughlin by (a) utilizing broader inclusion criteria not limited to behavioral (operant) approaches, (b) conducting a systematic review of the literature, (c) rating each included study’s certainty of ev- idence (quality of research design and controls) so results can be considered in light of each study’s methodological rigor, and (d) identifying advances in treatment that may have de- veloped since the previous review. A review of this nature is intended to offer directions for future research and to provide guidance to practitioners interested in the use of evidence- based treatments for echolalia in children with ASD. Method Search Procedures
- 11. Four electronic databases were searched to identify potential studies for this review: ERIC (EBSCO), Medline, Psychology and Behavioral Sciences Collection, and PsycINFO. There were no limitations on publication year, but results were lim- ited to English language, peer-reviewed research. Terms to describe individuals with an ASD were combined with terms to describe echolalia. The terms for individuals with an ASD included BAsperger,^ Bautis*,^ Bdevelopmental disab*,^ BASD,^ and BPDD-NOS.^ The terms searched to describe echolalia included Becholal*,^ Brepetitive speech,^ Brepetitive verbal*,^ Brepetitive talking,^ Brepetitive communication*,^ and Bpalilalia.^ Following the initial search, the last name of the first author of each included study was also entered into PsychINFO to identify any other potentially relevant studies that had been published by that author. Finally, the reference list of Kavon and McLaughlin (1995) was examined for ad- ditional studies meeting inclusion criteria. These search procedures were conducted in May 2014, updated in April 2015, and yielded a total of 568 articles (534 from the original search and 34 from the updated search). Rev J Autism Dev Disord (2016) 3:82–91 83 The title and abstracts of the 568 articles were screened using the predetermined inclusion criteria (see BInclusion Criteria^ section) to identify articles for potential inclusion in this re - view. Following this screening of title and abstracts, a total of 46 articles were identified for further review. Inclusion Criteria The 46 articles were then downloaded and evaluated based on the pre-set inclusion criteria. Studies were included if they (a)
- 12. included a participant diagnosed with ASD or was described as an individual with Bautistic-like behaviors^ (included due to the age of the literature base), (b) implemented an interven- tion and reported outcomes for echolalia (inclusive of palilalia and defined as repetition of a previously spoken word or phrase) as a dependent variable, (c) employed an experimental design (inclusive of single-case and group experimental de- signs), and (d) echolalia outcomes for the individual with ASD could be disaggregated from participants without ASD and target behaviors other than echolalia. Studies which im- plemented interventions for individuals with ASD who uti - lized echolalic speech but did not present outcomes related to the echolalia were excluded (e.g., Barrera and Sulzer - Azaroff 1983; Charlop-Christy and Kelso 2003; Charlop 1983). Studies which evaluated echolalia under different con- ditions but did not implement an intervention to address echo- lalia were also excluded (e.g., Rydell and Mirenda 1994; Violette and Swisher 1992). In addition, studies which imple- mented interventions to treat other repetitive speech (i.e., noncontextual vocal stereotypy, such as a sound rather than a word or phrase) were excluded (e.g., Mancia et al. 2000; Ahearn et al. 2000; Taylor et al. 2005). Studies excluded because data on echolalia were not disaggregated from other outcomes in- volving other topographies of behavior were Arntzen et al. (2006) and Mancia et al. (2000). For example, Arntzen et al. (2006) taught a 44-year-old woman functional verbal responses and tracked subsequent decreases in aberrant verbal behavior. Although aberrant verbal behavior included repetitive echolalic responses, the aberrant verbal behavior also included Bpsychotic^ verbalizations and results for the two were collapsed into one dependent variable. Finally, Cohen (1981) was excluded because the figure referenced in the article was not included in the article and was not accessible to the authors after multiple attempts to locate the figure through university- based library services. Ultimately, a total of 11 studies met inclusion criteria and were included in this review.
- 13. Descriptive Synthesis Included studies were reviewed and summarized based on the following categories: (a) participant characteristics (e.g., ver- bal and cognitive functioning), (b) type of echolalia (e.g., de- layed or immediate), (c) intervention procedures, (d) intervention outcomes, (e) maintenance and generalization of outcomes, and (f) research design and other indicators of rigor (i.e., certainty of evidence). Participant description in- cluded the number of participants with ASD, their ages, and gender. Participant verbal and cognitive functioning was cod- ed using reported standardized assessments or was gleaned from detailed descriptions of participant functioning. Echolalia was coded as either immediate, delayed, or palilalia, and when noted in the reviewed study, the operant function of echolalia was noted. Various procedural aspects were coded to identify intervention protocols or components (e.g., cues- pause-point protocol, script training, or reinforcement procedures) Intervention outcomes were summarized and coded as nega- tive, mixed, or positive. As all 11 studies employed single-case research designs, study outcomes were determined based on vi- sual analysis criteria for single-case research outlined by Kennedy (2005). A study was rated as having negative results if there was no reduction observed in echolalia as indicated by a flat or increasing trend in the intervention phase as compared to the baseline phase. Studies were coded as having mixed results if some, but not all, of the participants demonstrated a reduction in echolalia during the intervention phase relative to the baseline phase. Positive results indicated that echolalia decreased in all participants during intervention phase as relative baseline.
- 14. The study’s capacity to provide a certainty of evidence was rated as suggestive, preponderant, or conclusive, with conclu- sive being the highest rating (Schlosser 2009; Simeonsson and Bailey 1991; Smith 1981). Studies rated as conclusive had the following: (a) an experimental design capable of establishing experimental control (e.g., ABAB, multiple-baseline design, alternating treatments design), (b) sufficient interobserver agreement (IOA) collected on the observed educator behav- iors (i.e., agreement coefficients above 80 % and IOA collect- ed for a minimum of 20 % of the sessions), (c) intervention procedures detailed enough to promote replication of the pro- cedures, (d) operationalized descriptions of the dependent var - iable, and (e) demonstrated convincing effects of the interven- tion for every participant (i.e., received a rating of positive results). A study rated as preponderant met most of the criteria for a Bconclusive^ study, but results may have demonstrated Bmixed^ effects of the intervention for some or all of the participants with ASD. Any study that (a) lacked an experi- mental design capable of establishing experimental control, (b) did not meet the minimum IOA criterion, (c) did not operationally define the intervention procedures, (d) or did not operationally define the dependent variable were auto- matically rated as offering suggestive evidence. Interrater Reliability Inclusion Criteria To ensure accurate application of the in- clusion criteria, two raters reviewed each of the 46 articles, 84 Rev J Autism Dev Disord (2016) 3:82–91 resulting from the systematic search and initial title/abstract review, for potential inclusion. Agreement was reached on
- 15. whether to include or exclude a study on 100 % of the articles. Descriptive Synthesis To establish interrater reliability (IRR) for the data summaries, two independent raters coded five of the 11 included articles (46 %). A third rater reviewed the independent data summaries and made a decision as to wheth- er the summaries agreed. IRR was calculated based on wheth- er the two raters agreed on the extracted data. There were a total of 30 items in which there could be agreement or dis- agreement (i.e., five studies with six data categories each). IRR was calculated using percent agreement by dividing the total number of agreements by the sum of the agreements and disagreements and multiplying by 100 % to convert to a per- centage. Initial agreement for the coding of studies was 90 %. In instances of disagreement, the raters discussed until 100 % agreement was reached. Results Table 1 created from the coded study summarizes and displays each study according to the following: (a) participant charac- teristics (e.g., verbal and cognitive functioning), (b) type of echolalia (e.g., delayed or immediate), (c) intervention proce- dures, (d) intervention outcomes, (e) maintenance and gener - alization of outcomes, and (f) research design and other indi - cators of rigor (i.e., certainty of evidence). Participant Characteristics The 11 studies included a total of 25 participants with ASD. Ten of the 11 studies reported the gender of their participants with 17 male and 5 female participants. One study did not report participants’ gender (Laski et al. 1988). All of the stud- ies reported the participants’ ages, with a mean reported age of 8 years (range 3–21 years) across studies.
- 16. Ten studies (90 %) reported information regarding partici - pants’ verbal or cognitive functioning. Four studies (36 %) reported results from standardized cognitive assessments (i.e., Stanford-Binet, Merrill-Palmer, and Peabody Picture Vocabulary Test (PPVT)) with three studies including four participants with extremely low cognitive functioning (16 %; Handen et al. 1984; McMorrow and Foxx 1986; Nientimp and Cole 1992) and one study including one participant with below-average to average cognitive functioning (4 %; Freeman et al. 1975). Three studies (27 %) reported results from standardized language assessments (i.e., Alpern-Boll and PPVT-III) indicating extremely low verbal abilities and below-average cognitive functioning for eight of the 25 par- ticipants (32 %; Foxx et al. 2004; Karmali et al. 2005; Palyo et al. 1979). Five of the studies reported descriptive information regarding the language functioning of partici- pants, all of which suggested below-average verbal abilities for 16 of the 25 participants (64 %; Ganz et al. 2008; Hetzroni and Tannous 2004; Karmali et al. 2005; Laski et al. 1988; Valentino et al. 2012). Type of Echolalia Across the 11 studies, five targeted immediate echolalia only (45 %; Foxx et al. 2004; McMorrow and Foxx 1986; Nientimp and Cole 1992; Palyo et al. 1979; Valentino et al. 2012), two targeted delayed echolalia only (18 %; Ganz et al. 2008; Handen et al. 1984), and three studies (27 %) targeted both immediate and delayed echolalia (Freeman et al. 1975; Hetzroni and Tannous 2004; Laski et al. 1988). Finally, one study targeted palilalia (Karmali et al. 2005). No study report- ed operant functions of target behaviors. Intervention Procedures
- 17. All of the 11 studies employed an intervention with behavioral analytic components (e.g., differential reinforcement, model - ing, prompting). Five of the 11 studies (45 %) evaluated the effects of specific treatment package on echolalia (i.e., cues - pause-point; Natural Language Paradigm, and computer- based intervention). Cues-pause-point was the most frequent treatment package evaluated (n=3; 27 %; Foxx et al. 2004; McMorrow and Foxx 1986; Valentino et al. 2012). For exam- ple, Valentino and colleagues (2012) evaluated the use of cues-pause-point to treat a 3-year-old male child who echoed the instruction say during echoic training. Decreased echolalia and increase appropriate responding (e.g., repeating the target word without echoing say) were noted. Laski et al. (1988) trained parents to implement the Natural Language Paradigm within a clinical setting and then assessed the effects of the parent implemented program on child com- munication outcomes. Parents were taught to use direct rein- forcement of verbal attempts, to promote turn-taking with play items, to vary stimuli and exemplars, and to utilize shared control (i.e., rotating between child-led and parent-led activi- ties). Although appropriate vocalizations were the primary dependent variable, child engagement in echolalia was mea- sured as an ancillary variable with mixed results noted for the effects of the Natural Language Paradigm on echolalia. The final treatment package was a computer program enti- tled BI Can Word It Too^ that was available in both Arabic and Hebrew (Hetzroni and Tannous 2004). The program presented participants with a simulated situation in which a parent asked the participant a question. The participant would then choose the appropriate sentence or question option, and an animation of their choice would be played. For example, if the question was Bwhat would you like to play with^ and the participant selected the option BI want to play ball with you,^ an
- 18. Rev J Autism Dev Disord (2016) 3:82–91 85 T ab le 1 In te rv en ti on s st ud ie s to d ec re as e ec h o la li a fo r
- 69. ar ia b le ) 86 Rev J Autism Dev Disord (2016) 3:82–91 T ab le 1 (c o n ti n u ed ) A rt ic le P ar ti ci p an
- 117. is re v ie w Rev J Autism Dev Disord (2016) 3:82–91 87 animation of a father and child playing ball would appear. The participant was then observed in their classroom, and data were collected on appropriate and inappropriate verbal behavior. Results were mixed with some participants demonstrating improvement in echolalia and some demon- strating no improvement. The remaining six studies employed a variety of behavior analytic interventions to treat echolalia. Behavioral compo- nents included error correction and differential reinforcement (n=2; Freeman et al. 1975; Palyo et al. 1979). differential reinforcement of lower rates (n=1; Handen et al. 1984). modeling and positive reinforcement (n=2; Karmali et al. 2005; Palyo et al. 1979). modeling (n=1; McMorrow and Foxx 1986). time delay and differential reinforcement (n=1; Nientimp and Cole 1992). and visual cues with differential reinforcement (n=1; Ganz et al. 2008). For example, Handen and colleagues (1984) implemented differential rein- forcement of lower rates (DRL) of behavior to decrease the echolalia of a 16-year-old male with ASD. The intervention occurred over an 18-month time frame and involved pro- viding the participant with tokens for engaging in lower rates of echolalia than a predetermined criterion. When the participant engaged in echolalia below the target rate, he exchanged the tokens for a tangible item from his reinforcement menu. The intervention was effective
- 118. in reducing the participant’s engagement in echolalia; however, after intervention was removed, the partici- pant’s echolalia returned to baseline levels. In another study, Ganz et al. (2008) taught two children with ASD who engaged in echolalia to engage in reciprocal social-communicative responses (e.g., compliments, ques- tions, and statements corresponding to the current activity). Responses were taught by providing visual scripts of the target response and systematically fading scripts over three phases. To reduce echolalia, a visual cue was presented which sig- naled to the participant that they should cease talking (i.e., a 3″×3″ line drawing of a face with a finger in front of the mouth indicating Bquiet^). This visual cue was introduced only if the participant engaged in echolalia. Results indicated clear decreases in echolalia. Intervention Outcomes The data from nine of the studies indicated that the results were positive for all participants (Foxx et al. 2004; Freeman et al. 1975; Ganz et al. 2008; Handen et al. 1984; Karmali et al. 2005; McMorrow and Foxx 1986; Nientimp and Cole 1992; Palyo et al. 1979; Valentino et al. 2012). Data from two of the studies suggested mixed results with some participants dem- onstrating improved behavior and some demonstrating no im- provement (Hetzroni and Tannous 2004; Laski et al. 1988). The first study( Laski et al. 1988) measured echolalia as an ancillary dependent variable and provided pre- and post- treatment means for echolalia, with no differences noted in one setting (i.e., the break room). The second study (Hetzroni and Tannous 2004) utilized a multiple baseline de- sign across settings to evaluate the effects of their technology- based intervention on participant echolalia. However, de- creases in echolalia were not demonstrated for all three set-
- 119. tings for any of the participants undercutting the experimental control of the multiple baseline design. The two studies with mixed results represented 8 of the 25 participants. Maintenance and Generalization Five of studies assessed maintenance of behavior change (Foxx et al. 2004; Handen et al. 1984; Nientimp and Cole 1992; Palyo et al. 1979; Valentino et al. 2012). and one study was published as a long-term follow-up to the McMorrow and Foxx study (1986; Foxx and Faw 1990). The timing of the collection of maintenance data ranged from immediately fol- lowing the conclusion of the intervention (Foxx et al. 2004; McMorrow and Foxx 1986; Nientimp and Cole 1992) to 57 months after the intervention (Foxx and Faw 1990). All studies reported that echolalia levels at maintenance were be- low baseline levels. Seven studies assessed stimulus general - ization (Foxx et al. 2004; Hetzroni and Tannous 2004; Karmali et al. 2005; McMorrow and Foxx 1986; Nientimp and Cole 1992; Palyo et al. 1979; Valentino et al. 2012) in- cluding generalization across settings, people, materials, and different preceding utterances (questions). Four studies report- ed positive results for generalization (Foxx et al. 2004; Karmali et al. 2005; Palyo et al. 1979; Valentino et al. 2012). Two studies reported that generalization occurred for some participants but not for all (Hetzroni and Tannous 2004; Nientimp and Cole 1992). One study found that results did not generalize for the participants (McMorrow and Foxx 1986). Certainty of Evidence Six of the studies were categorized as offering a conclusive level of evidence with positive results, sufficient research de - sign and IOA data, and detailed procedural descriptions (Foxx et al. 2004; Ganz et al. 2008; Handen et al. 1984; Karmali et al. 2005; McMorrow and Foxx 1986; Valentino et al. 2012). Five
- 120. studies were categorized as suggestive (Freeman et al. 1975; Hetzroni and Tannous 2004; Laski et al. 1988; Nientimp and Cole 1992; Palyo et al. 1979). Of the five studies, three did not demonstrate experimental control (Freeman et al. 1975; Nientimp and Cole 1992; Palyo et al. 1979). two studies had mixed results (Hetzroni and Tannous 2004; Laski et al. 1988). and one study did not assess IOA (Freeman et al. 1975). None of the studies was classified at the preponderant level of evidence. 88 Rev J Autism Dev Disord (2016) 3:82–91 Discussion The purpose of this review was to identify promising practices for decreasing echolalia in individuals with ASD. This sys- tematic literature review synthesized 11 studies which employed a variety of behavioral interventions. Of the 11 studies, nine reported positive results for 17 participants, and two of the studies reported mixed results for two participants. When examining the quality of the literature base, six of the 11 studies were classified as providing conclusive evidence. Ultimately, the findings of this review indicate that the litera- ture base cannot conclusively support any one approach for the treatment of echolalia in individuals with ASD. Implications for Research The first purpose of this review was to update the previous review by Kavon and McLaughlin (1995) to identify effective interventions for the treatment of echolalia in individuals with ASD. Although no single intervention procedure or package met any of the commonly used criteria for classification as a well-established or evidence-based practice (e.g., Chambless
- 121. and Holland 1998; Odom and Wolery 2003). a number of themes emerged. First, of the six studies classified as conclu- sive, all contained behavioral analytic intervention compo- nents (e.g., programmed reinforcement contingencies) sug- gesting support for operant-based treatments in the reduction of echolalia for individuals with ASD. When considering im- mediate echolalia, the cues-pause-point intervention was iden- tified as effective in three studies (Foxx et al. 2004; McMorrow and Foxx 1986; Valentino et al. 2012). This con- clusion supports the previous descriptive review identifying cues-pause-point as a potentially effective intervention for im- mediate echolalia. Of note, only two studies have evaluated the effects of cues-pause-point since the previous review (Kavon and McLaughlin 1995) highlighting the need for more research in this area. Conclusive studies evaluating interventions for delayed echolalia also utilized behavioral analytic components. Three interventions, DRL of behavior (Handen et al. 1984). script training plus visual cues (Ganz et al. 2008). and tact modeling plus positive reinforcement for appropriate responses (Karmali et al. 2005). were all identified as effective for de - layed echolalia. Of particular interest is the study by Ganz et al. (2008) which utilized visual cues to signal to the partic - ipant that they should cease talking. In addition, visual scripts were provided to prompt the target response. Although not inclusive of all the elements of cues-pause-point, Ganz et al. did implement a cue to remain silent and a point to prompt the correct answer. In addition, the DRL of behavior intervention by Handen et al. (1984) utilized differential reinforcement which was a contingency in effect in the cues-pause-point interventions. Overall, the research combined provides preliminary support for operant-based behavioral interven- tions in general and cues-pause-point in particular.
- 122. As the interventions evaluated in these studies align with the operant conditioning paradigm, it is alarming that none of the studies assessed the operant function of echolalia. In other forms of challenging behavior (e.g., aggression, property de- struction, and self-injury), identifying the function of the be- havior via a functional analysis procedure (Iwata et al. 1982/1994; Lydon et al. 2012) is associated with better re- sponse to treatment (e.g., Didden et al. 2006). Of particular concern is that echolalia may serve various social as well as non-social communicative functions for individuals with ASD (Goren et al. 1977; Healy and Leader 2011). If echolalia is reduced during treatment but a functionally equivalent re- placement behavior is not taught, this could limit the mainte- nance and generalization of the behavioral change (Schreibman and Carr 1978). In addition, as there is diver - gence within the field regarding whether echolalia is nonfunc- tional (e.g., Lovaas, Schreibman, and Koegel 1974). a neces- sary part of developing functional communication (e.g., Roberts 2014). or serves a social function (e.g., Prizant and Duncan 1981). identifying the function of echolalia would help guide future research and practice. One potential strength of this literature base is the assess- ment of maintenance of behavioral change following cessa- tion of the intervention phase. Of the six articles that assessed the maintenance of behavioral change, all reported positive results indicating levels of echolalia maintained below base- line levels during follow-up sessions. However, although sev- en of the studies did evaluate the generalization of the results across stimuli, people, and settings, results were mixed with only four reporting successful generalization. Future re- searchers might consider evaluating interventions to promote sustained behavioral change (e.g., fading, multiple exemplar training; Valentino et al. 2012). Implications for Practice
- 123. A second purpose of this review was to offer guidance to practitioners interested in the use of evidence-based treatments for individuals with ASD. Given the limited number of con- clusive studies, recommendations as to an evidence-based in- tervention for decreasing echolalia cannot be drawn. However, the results of this review did suggest that cues- pause-point, which was investigated by three different studies with positive results and conclusive levels of evidence, is po- tentially effective for immediate echolalia (Foxx et al. 2004; McMorrow and Foxx 1986; Valentino et al. 2012). Although these results support the conclusions from previous research that cues-pause-point is potentially effective (Kavon and McLaughlin 1995). practitioners should use caution when implementing this intervention due to the limited number of studies. In particular, practitioners should closely monitor the Rev J Autism Dev Disord (2016) 3:82–91 89 intervention effects through ongoing progress monitoring and rely on objective data to evaluate the effectiveness of the intervention. Limitations of this Review There are a couple of limitations of this review to consider. First, the definition of echolalia used by the authors was intended to distinguish echolalia from vocal stereotypy. However, it was difficult to identify a definition of echolalia that was accepted throughout the literature base. In addition, as none of the studies reported the function of the target echo- lalia behavior, it is uncertain whether echolalia was isolated from other forms of vocal stereotypy. A second limitation is the age of the literature base. Of the 11 studies reviewed, six of
- 124. the studies were published over 20 years ago. As research quality indicators have evolved dramatically in the past 20 years, the age of this literature base may have been a factor in the conclusiveness of the evidence. In addition, since the review by Kavon and McLaughlin (1995). only five additional studies have been published on this topic. Therefore, there is a need to update and expand this literature base to promote the use of evidence-based practices in the treatment of echolalia for individuals with ASD. A third limitation is the procedures used to code intervention outcomes as applied to this literature base. Study results were rated as Bpositive,^ mixed, or Bnegative^ with mixed indicating that some but not all partic- ipants demonstrated improvements in behavior. Five of the 11 included studies contained only one subject with ASD, there- fore restricting the rating of the outcomes to either negative or positive. Although restricted codes could have negatively im- pacted intervention outcome ratings, all of the studies with one subject received positive ratings. However, the limited num- ber of subject limits the external validity of the conclusions. A fourth limitation is the absence of large-scale randomized con- trol trials in the resulting literature base. Although this might be a reflection of the exceptionality of the population, the exclusive use of single-subject designs limits the external va- lidity of this literature base. A fifth limitation of this review is the focus on individuals with ASD. Future researchers might consider expanding to include other developmental disabil - ities to ensure a more comprehensive review. Such an analysis might allow for distinctions relevant to the presentation and/or treatment of echolalia in children with ASD relative to indi - viduals with other forms of disability. Compliance with Ethical Standards Funding The authors report no funding for this manuscript. Conflict of Interest The authors report no conflicts of interest.
- 125. Ethical Approval This article does not contain any studies with human participants performed by any of the authors. References *Indicates studies which were included in this review Ahearn, W. H., Clark, K. M., Macdonald, R. P., & Chung, B. I. (2000). Assessing and treating vocal stereotypy in children with autism. Journal of Applied Behavior Analysis, 40, 263–275. doi:10.1901/ jaba.2007.30-06. American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing. Arntzen, E., Tonnessen, I. R., & Brouwer, G. (2006). Reducing aberrant verbal behavior by building a repertoire of rational verbal behavior. Behavioral Interventions, 21, 177–193. doi:10.1002/bin.220. Barrera, R. D., & Sulzer-Azaroff, B. (1983). An alternating treatment comparison of oral and total communications training programs with echolalic autistic children. Journal of Applied Behavior Analysis, 16, 379–394. doi:10.1901/jaba.1983.16-379. Chambless, D. L., & Holland, S. D. (1998). Defining empirically sup- ported therapies. Journal of Consulting and Clinical
- 126. Psychology, 66, 7–18. Charlop-Christy, M. H., & Kelso, S. E. (2003). Teaching children with autism conversational speech using cue card/written script program. Education and Treatment of Children, 26(2), 108–127. Retrieved from: http://www.educationandtreatmentofchildren.net/. Charlop, M. H. (1983). The effects of echolalia on acquisition and gen- eralization of receptive labeling in autistic children. Journal of Applied Behavior Analysis, 16, 111–126. doi:10.1901/jaba.1983. 16-111. Cohen, M. (1981). Development of language behavior in an autistic child using total communication. Exceptional Children, 47, 379–381. Retrieved from: http://journals.cec.sped.org/ec/. Didden, R., Korzilius, H. K., Oorsouw, W. V., & Sturmey, P. (2006). Behavioral treatment of challenging behaviors in individuals with mild mental retardation: meta-analysis of single-subject research. American Journal of Mental Retardation, 111, 290–298. Fay, W. H. (1969). On the basis of autistic echolalia. Journal of Communication Disorders, 2, 31–41. doi:10.1016/0021- 9924(69) 90053-7.
- 127. Fay, W. H. (1973). On the echolalia of the blind and of autistic children. The Journal of Speech and Hearing Disorders, 38, 478–489. Retrieved from: http://www.ncbi.nlm.nih.gov/pubmed/4754881. *Foxx, R. M., & Faw, G. D. (1990). Long-term follow-up of echolalia and question answering. Journal of Applied Behavior Analysis, 23, 387–396. doi: 10.1901/jaba.1990.23-387. Foxx, R. M., Faw, G. D., McMorrow, M. J., Kyle, M. S., & Bittle, R. G. (1988). Replacing maladaptive speech with verbal labeling responses: an analysis of generalized responding. Journal of Applied Behavior Analysis, 21, 411–417 *Foxx, R. M., Schreck, K. A., Garito, J., Smith, A., Weisenberger, S. (2004). Replacing the echolalia of children with autism with func- tional use of verbal labeling. Journal of Developmental and Physical Disabilities, 16, 307–320. doi: 10.1007/s10882-004-0688-5. *Freeman, B. J., Ritvo, E., Miller, R. (1975). An operant procedure to teach an echolalic autistic child to answer questions appropriately. Journal of Autism and Childhood Schizophrenia, 5, 169–176. doi: 10.1007/BF01537933. *Ganz, J., Kaylor, M., Bourgeois, B., Hadden, K. (2008). The impact of social scripts and visual cues on verbal communication in three
- 128. children with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 23, 79–94. doi: 10.1177/ 1088357607311447. 90 Rev J Autism Dev Disord (2016) 3:82–91 http://dx.doi.org/10.1901/jaba.2007.30-06 http://dx.doi.org/10.1901/jaba.2007.30-06 http://dx.doi.org/10.1002/bin.220 http://dx.doi.org/10.1901/jaba.1983.16-379 http://www.educationandtreatmentofchildren.net/ http://dx.doi.org/10.1901/jaba.1983.16-111 http://dx.doi.org/10.1901/jaba.1983.16-111 http://journals.cec.sped.org/ec/ http://dx.doi.org/10.1016/0021-9924(69)90053-7 http://dx.doi.org/10.1016/0021-9924(69)90053-7 http://www.ncbi.nlm.nih.gov/pubmed/4754881 http://dx.doi.org/10.1901/jaba.1990.23-387 http://dx.doi.org/10.1007/s10882-004-0688-5 http://dx.doi.org/10.1007/BF01537933 http://dx.doi.org/10.1177/1088357607311447 http://dx.doi.org/10.1177/1088357607311447 Goren, E. R., Romanczyk, R. G., & Harris, S. L. (1977). A functional analysis of echolalic speech. Behavior Modification, 1, 481– 498. doi:10.1177/014544557714003. *Handen, B. L., Apolito, P. M., Seltzer, G. S. (1984). Use of differential reinforcement of low rates of behavior to decrease repetitive speech in an autistic adolescent. Journal of Behavior Therapy and Experimental Psychiatry, 15, 359–364. doi: 10.1016/0005-
- 129. 7916(84)90102-2. Healy, O., & Leader, G. (2011). Assessments of rituals and stereotypy. In J. L. Matson & P. Sturmey (Eds.), International handbook of autism and pervasive developmental disorders (pp. 233–245). New York: Springer. Hetzroni, O. E., & Tannous, J. (2004). Effects of a computer - based inter- vention program on the communicative functions of children with autism. Journal of Autism and Developmental Disorders, 34, 95– 113. doi:10.1023/B:JADD.0000022602.40506.bf. Howlin, P. (1982). Echolalic and spontaneous phrase speech in autistic children. Journal of Child Psychology and Psychiatry, 23, 281– 293. doi:10.1111/j.1469-7610.1982.tb00073.x. Iwata, B. A., Dorsey, M. F., Slifer, J. J., Bauman, K. E., & Richman, G. S. (1994). Toward a functional analysis of self-injury. Journal of Applied Behavior Analysis, 27, 197–209. doi:10.1901/jaba.1994. 27-197 (Reprinted from Analysis and Intervention in Developmental Disabilities, 2, 3–20, 1982). *Karmali, I., Greer, R. D., Nuzzlo-Gomez, R., Ross, D. E., Rivera- Valdes, C. (2005). Reducing palilalia by presenting tact corrections
- 130. to young children with autism. Analysis of Verbal Behavior, 21, 145–153. Retrieved from: http://www.ncbi.nlm.nih.gov/pmc/ journals/609/ Kavon, N. M., & McLaughlin, T. F. (1995). Interventions for echolalic behaviour for children with autism: a review of verbal prompts and the cues pause point procedure. B.C. Journal of Special Education, 19(2–3), 39–45. Retrieved from: http://eric.ed.gov/?id=EJ519927. Kennedy, C. H. (2005). Single-case designs for educational research. Boston, MA: Allyn and Bacon. *Laski, K. E., Charlop, M. H., Schriebman, L. (1988). Training parents to use the natural language paradigm to increase their autistic chil - dren’s speech. Journal of Applied Behavior Analysis, 21, 391– 400. doi: 10.1901/jaba.1988.21-391. Light, C., Roberts, B., Dimarco, R., & Greiner, N. (1998). Augmentative and alternative communication to support receptive and expressive communication for people with autism. Journal of Communication Disorders, 31, 153–180. doi:10.1016/S0021-9924(97)00087-7. Lovaas, O. I., Koegel, R. L., Simmons, J. Q., & Long, J. S. (1973). Some generalization and follow-up measures on autistic children in behav-
- 131. ior therapy. Journal of Applied Behavior Analysis, 6, 131–166. doi: 10.1901/jaba.1973.6-131. Lovaas, O. I., Schreibman, L., & Koegel, R. L. (1974). A behavior mod- ification approach to the treatment of autistic children. Journal of Autism and Developmental Disabilities, 4, 111–129. doi:10.1007/ BF02105365. Lovaas, O. I. (1977). The autistic child: language development through behavior modification. New York: Irvington. Lydon, S., Healy, O., O’Reilly, M. F., & Lang, R. (2012). Variations in functional analysis methodology: a systematic review. Journal of Developmental and Physical Disabilities, 24, 301–326. Mancia, C., Tankersley, M., Kamps, D., Kravits, T., & Parrett, J. (2000). Brief report: reduction of inappropriate vocalizations for a child with autism using a self-management treatment program. Journal of Autism and Developmental Disorders, 30, 599–606. doi:10.1023/ A:1005695512163. *McMorrow, M. J., & Foxx, R. M. (1986). Some direct and generalized effects of replacing an autistic man’s echolalia with correct responses to questions. Journal of Applied Behavior Analysis,
- 132. 19, 289–297. doi: 10.1901/jaba.1986.19-289. McMorrow, M. J., Foxx, R. M., Faw, G. D., & Bittle, R. G. (1987). Cues- pause-point language training: teaching echolalics functional use of their verbal labeling repertoires. Journal of Applied Behavior Analysis, 20, 11–22. doi:10.1901/jaba.1987.20-11. Neely, L. C. (2014). Echolalia. In C. R. Reynolds, K. J. Vannest, & E. Fletcher-Janzen (Eds.), Encyclopedia of special education: a refer- ence for the education of children, adolescents, and adults with disabilities and other exceptional individuals (4th ed.). Hoboken, NJ: John Wiley & Sons. *Nientimp. E. G., & Cole, L. (1992). Teaching socially valid social inter- action responses to students with severe disabilities in a school set- ting. Journal of School Psychology, 30, 343–354. doi: 10.1016/ 0022-4405(92)90002-M. Odom, S. L., & Wolery, M. (2003). A unified theory of practice in early intervention/early child special education: evidence-based practices. Journal of Special Education, 37, 164–173. *Palyo, W. J., Cooke, T. P., Schuler, A. L., Apolloni, T. (1979). Modifying echolalic speech in preschool children: training and gen- eralization. American Journal of Mental Deficiencies, 83, 480–
- 133. 489. Prizant, B. M., & Duncan, J. F. (1981). The functions of immediate echolalia in autistic children. The Journal of Speech and Hearing Disorders, 46, 241–249. Retrieved from: http://www.ncbi.nlm.nih. gov/pubmed/7278167. Roberts, J. M. A. (2014). Echolalia and language development in children with autism. In J. Arciuli & J. Brock (Eds.), Communication in autism (pp. 53–74). Philadelphia: John Benjamins Publishing Company. Rydell, P. J., & Mirenda, P. (1994). Effects of high and low constraint utterances on the production of immediate and delayed echolalia in young children with autism. Journal of Autism and Developmental Disorders, 24, 719–735. doi:10.1007/BF02172282. Schlosser, R. (2009). The role of evidence-based journals as evidence- based information sources. Applied Behavior Analysis International Annual Convention (Conference). Phoenix: Az. Schreibman, L., & Carr, E. G. (1978). Elimination of echolalic responding to questions through the training of a generalized verbal response. Journal of Applied Behavior Analysis, 11, 453–463. doi: 10.1901/jaba.1978.11-453.
- 134. Simeonsson, R., & Bailey, D. (1991). Evaluating programme impact: levels of certainty. In D. Mitchell & R. Brown (Eds.), Early inter- vention studies for young children with special needs. New York: Chapman and Hall. Smith, N. (1981). The certainty of evidence in health evaluations. Evaluation and Program Planning, 4, 273–278. Retrieved from: http://www.journals.elsevier.com/evaluation-and-program- planning/. Stribling, P., Rae, J., & Dickerson, P. (2007). Two forms of spoken rep- etition in a girl with autism. International Journal of Language & Communication Disorders, 42, 427–444. doi:10.1080/ 13682820601183659. Taylor, B. A., Hoch, H., & Weissman, B. (2005). The analysis and treat- ment of vocal stereotypy in a child with autism. Behavioral Interventions, 20, 239–253. doi:10.1002/bin.200. *Valentino, A. L., Schillingsburg, M. A., Conine, D. E., & Powell, N. M. (2012). Decreasing echolalia of the instruction Bsay^ during echoic training through use of the cues-pause-point procedure. Journal of Behavioral Education, 21, 315–328. doi: 10.1007/s10864-012- 9155-z.
- 135. Violette, J., & Swisher, L. (1992). Echolalic responses by a child with autism to four experimental conditions of sociolinguistic input. Journal of Speech and Hearing Research, 35, 139–147. doi:10. 1044/jshr.3501.139. Rev J Autism Dev Disord (2016) 3:82–91 91 http://dx.doi.org/10.1177/014544557714003 http://dx.doi.org/10.1016/0005-7916(84)90102-2 http://dx.doi.org/10.1016/0005-7916(84)90102-2 http://dx.doi.org/10.1023/B:JADD.0000022602.40506.bf http://dx.doi.org/10.1111/j.1469-7610.1982.tb00073.x http://dx.doi.org/10.1901/jaba.1994.27-197 http://dx.doi.org/10.1901/jaba.1994.27-197 http://www.ncbi.nlm.nih.gov/pmc/journals/609/ http://www.ncbi.nlm.nih.gov/pmc/journals/609/ http://eric.ed.gov/?id=EJ519927 http://dx.doi.org/10.1901/jaba.1988.21-391 http://dx.doi.org/10.1016/S0021-9924(97)00087-7 http://dx.doi.org/10.1901/jaba.1973.6-131 http://dx.doi.org/10.1007/BF02105365 http://dx.doi.org/10.1007/BF02105365 http://dx.doi.org/10.1023/A:1005695512163 http://dx.doi.org/10.1023/A:1005695512163 http://dx.doi.org/10.1901/jaba.1986 .19-289 http://dx.doi.org/10.1901/jaba.1987.20-11 http://dx.doi.org/10.1016/0022-4405(92)90002-M http://dx.doi.org/10.1016/0022-4405(92)90002-M http://www.ncbi.nlm.nih.gov/pubmed/7278167 http://www.ncbi.nlm.nih.gov/pubmed/7278167 http://dx.doi.org/10.1007/ BF02172282 http://dx.doi.org/10.1901/jaba.1978.11-453 http://www.journals.elsevier.com/evaluation-and-program- planning/ http://www.journals.elsevier.com/evaluation-and-program-
- 136. planning/ http://dx.doi.org/10.1080/13682820601183659 http://dx.doi.org/10.1080/13682820601183659 http://dx.doi.org/10.1002/bin.200 http://dx.doi.org/10.1007/s10864-012-9155-z http://dx.doi.org/10.1007/s10864-012-9155-z http://dx.doi.org/10.1044/jshr.3501.139 http://dx.doi.org/10.1044/jshr.3501.139 Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Treatment of Echolalia in Individuals with Autism Spectrum �Disorder: a Systematic ReviewAbstractMethodSearch ProceduresInclusion CriteriaDescriptive SynthesisInterrater ReliabilityResultsParticipant CharacteristicsType of EcholaliaIntervention ProceduresIntervention OutcomesMaintenance and GeneralizationCertainty of EvidenceDiscussionImplications for ResearchImplications for PracticeLimitations of this ReviewReferences*Indicates studies which were included in this review ment program to reduce stereotypic (repetitive) behav- iors. Four children diagnosed with autism were referred because of high frequency of stereotypic behaviors (e.g., arm flapping, finger flexing, humming, nonsense vocal- izations). After self-management procedures were taught, stereotypic behaviors decreased to zero levels for all chil - dren, however, the two children with vocal stereotypies required a longer period of self-management before de- creases were noted. Similarly, Stahmer and Schreibman (1992) investigated the effects of self-management pro- cedures for a variety of target behaviors including in-
- 137. creasing appropriate play skills, and reducing stereotypic behaviors of three children with autism. Participants were 7 to 13 years old and were referred for treatment by their parents due to destructive and obsessive behavior with toys in unsupervised settings. Appropriate play increased for all three children during treatment, fading, posttreat- ment, and follow-up observations and self-stimulatory behavior decreased to zero levels. Results from these studies indicated the successful use of self-management to reduce inappropriate behaviors (R. L. Koegel & Koegel, 1990), to increase schedule following (Newman, Buffington, O’Grady, Poulson, & Hemmes, 1995), and INTRODUCTION Self-management procedures, as reported in the literature, have incorporated components of self- assessment, self-recording, and self-reinforcement (R. L. Koegel & Frea, 1993). Applications of self-management to children with autism have evolved from procedures to (a) improve on task behaviors of children with retarda- tion, learning disabilities, and behavior disorders; and (b) to decrease disruptive, inappropriate, or stereotypic behaviors (Gardner, Clees, & Cole, 1983; L. K. Koegel, Koegel, Hurley, & Frea, 1992; Reese, Sherman, & Shel- don, 1984; Shapiro, McGonigle, & Ollendick, 1980; Stah- mer & Schreibman, 1992). In an exemplary study, R. L. Koegel and Koegel (1990) assessed whether children with autism could be taught to use a self-management treat- Brief Reports Brief Report: Reduction of Inappropriate Vocalizations for a Child with Autism Using a Self-Management Treatment Program
- 138. Catherine Mancina,1 Melody Tankersley,2 Debra Kamps,1,4 Tammy Kravits, 1 and Jean Parrett3 Self-management procedures that incorporate elements of self- assessment, self-recording, and self-reinforcement have reduced stereotypic (i.e., repetitive) behaviors in children with autism in clinical settings. This study examined the effects of a self- management program used to re- duce high rates of inappropriate vocalizations (e.g., humming, tongue clucking, perseverative and echolalic words/phrases) in a 12-year-old girl having autism served in a public school classroom. When self-management was applied to inappropriate vocalizations in a multiple- baseline design during leisure, prevocational, and reading tasks, the occurrence of vocaliza- tions decreased. Implications for teaching these procedures in classroom settings are discussed. KEY WORDS: Self-management procedures; autism; inappropriate vocalization. Journal of Autism and Developmental Disorders, Vol. 30, No. 6, 2000 599 0162-3257/00/1200-0599$18.00/0 © 2000 Plenum Publishing Corporation 1 University of Kansas, Kansas City. 2 Kent State University, Kent, Ohio. 3 Kansas City, Kansas Public Schools, Kansas City. 4 Address all correspondence to Debra M. Kamps, Juniper
- 139. Gardens Children’s Project, 650 Minnesota Avenue, 2nd floor, Kansas City, Kansas 66101. to increase social behaviors (R. L. Koegel & Frea, 1993; Stahmer & Schreibman, 1992). The purpose of the present study was to extend the literature on classroom-based self-management procedures. The investigation examined the effects of self-management procedures for a 12-year-old girl di- agnosed with autism and moderate mental retardation. Three inappropriate behaviors were identified for the participant (i.e., vocalizations, facial movements, body movements); however, self-management proce- dures were applied to only one behavior (i.e., vocal- izations) and collateral effects were observed for the others. Because studies indicated that the reduction of vocalizations requires longer durations of treatment in children with autism (R. L. Koegel & Koegel, 1990), the amount of time required to teach the self- management procedures and the levels to which tar- get behaviors decreased were investigated.The present study, therefore, focused on the reduction of vocaliza- tions with effects noted for (a) change in the target be- havior, (b) change in collateral behaviors, (c) the treatment effects across tasks, (d) the accuracy of the student’s self-recording, and (e) time required to teach the procedures. METHOD, STUDY 1
- 140. Participant and Settings Target student.The participant, Keri, a 12-year- old African American girl, was diagnosed with autism and moderate mental retardation. Keri attended sum- mer school in a self-contained, special education classroom located in an urban, elementary school set- ting. On the Wecshler Intelligence Scale for Children (Wecshler, 1974), Keri scored a 46 on the perfor- mance subtest. No information concerning her verbal subtest was provided. Her estimated full IQ range was between 42 and 55. She read sight words and simple sentences, had good verbal comprehension, and re- sponded correctly to yes/no questions. She indepen- dently participated in prevocational and leisure activities. Of primary concern to her teacher was her verbal behavior. Keri’s verbal communication (two- to-three-word phrases) was continuously interrupted by noises (humming, whistling, tongue clucking); and per- severative vocalizations. She also exhibited stereotypic body and facial movements. Assessments and inter- views indicated that these behaviors were primarily maintained by sensory stimulation. Keri’s teachers re- ported that her vocalizations were very disruptive, and interfered with her academic and social learning. Keri 600 Mancina, Tankersley, Kamps, Kravits, and Parrett was most attentive in quiet environments with one-to-one teaching situations. Treatment Providers/Observers.All three indi- viduals who participated in this study including the first author, a research associate, and a doctoral student had at least 5 years experience using behavioral techniques to teach children with autism, behavior disorders,
- 141. and/or other developmental disabilities. Treatment providers also served as observers for the study. Setting. The experimental sessions were con- ducted in a special education classroom (20 × 40 m), located in a public school, 4 to 5 days a week. Sessions lasted 5 minutes each. Four to six sessions were con- ducted every morning within a 3-hour period. Keri fol- lowed her regular morning schedule of activities with self-management sessions conducted during typical tasks (i.e., leisure, prevocational, and reading). Keri was seated at her own desk located in the back of the classroom. One treatment provider and one observer sat in chairs placed on each side of her, and five stu- dents were also working at individual desks. Dependent Variables and Measurement Dependent Variable/Target Behavior.The ob- server recorded occurrence or nonoccurrence of three categories of behavior: (a) vocalizations, (b) facial movements, (c) and body movements during 10-second intervals for 5 minutes. Occurrence of self-injurious be- havior within 10-second intervals was also recorded. The occurrence of vocalizations was identified as the tar - get behavior, however, all three behaviors were mea- sured to examine collateral effects of the self-management procedures. Vocalizations were defined as (a) noises such as humming, whistling, tongue clucking, and (b) perse- verative (repeated) and echolalic words or phrases. Fa- cial movements were recorded as any nonfunctional movements of the face including exaggerated eye blinks, rolling eyes, noncontextual smiling, tongue pro- trusions, and raising and lowering of eyebrows. Body movements were defined as any nonfunctional body movements including hand and finger manipulations,
- 142. stomping feet, head butts, elbow jabs, and head jerks. Any occurrence of self-injury, such as hand biting or hitting her head, was recorded. Observations.Data were collected by the treat- ment providers. They randomly rotated between teach- ing and supervising the self-management procedures and recording the data. Data were collected using a 10- second whole interval recording procedure to record the occurrence or nonoccurrence of (a) target vocal - izations, (b) facial movements, (c) and body move- ments. When a self-injurious behavior was observed, the observer placed a circle around the interval to in- dicate the occurrence of a self-injurious behavior. Data were recorded during leisure, prevocational, and read- ing tasks. Data were not taken during self-reinforcement (see Procedures). Reliability. Interobserver reliability was collected for each behavior during baseline and treatment phases, for 38% (n = 36) of all sessions, using video- tapes of sessions. The primary observer and the treat- ment provider viewed the tapes simultaneously, while scoring independently. An agreement was scored if both observers recorded a “+” or when both recorded a “−” for each behavior in an interval. Reliability was measured by calculating the number of agreements be- tween the two observers divided by the number of agreements and disagreements, multiplied by 100. The mean percentage of reliability for vocalizations was 95% (R = 63–100%), 87% (R = 63–100%) for facial movements, and 89% (R = 75–100%) for body move- ments.
- 143. Experimental Design and Procedures, Study 1 A multiple-baseline design (Kazdin, 1984) across tasks was used to teach Keri to use self-management procedures. Occurrences of the inappropriate vocal- izations and collateral behaviors were recorded during experimental conditions: baseline (A) and treatment phases (B). Treatment (self-management) was only ap- plied to inappropriate vocalizations, as the teacher de- termined this to be the most problematic behavior. Baseline (A).Data were collected during Keri’s participation in leisure, prevocational, and reading tasks, as included in her IEP and presented to her by the class- room teacher. Baseline data were collected over 11 days for the leisure task, 20 days for the prevocational task, and 32 days for the reading task, Leisure task materials included coloring and sticker books, drawing boards, memory match games, photograph albums, and puzzles. Prevocational materials/activities included sorting, stamping, and collating items. Materials used during the reading tasks included flash cards, worksheets, and the student’s Edmark® reading book. Treatment Phases (B).Self-management proce- dures, adapted from a training manual by R. L. Koegel, Koegel, and Parks (1990), were implemented first dur- ing leisure tasks followed by, prevocational, and read- ing tasks. The treatment procedures incorporated the use of (a) the same classroom materials as used in baseline tasks, (b) self-management materials, and (c) the teach- ing of self-management including: identification of be- Reduction of Inappropriate Vocalizations 601
- 144. haviors, self-recording, self-reinforcement, independent use of the program, and assessing student accuracy. Teaching the self-management programtook place in Keri’s summer school classroom. Self-management materials served as stimuli for Keri to perform the self–management procedures and included a Timex dig- ital watch with a repeat alarm to signal 10-second in- tervals, self-recording sheets (i.e., a sheet of paper with 12 empty boxes with the words “quiet” and “noisy” written beside them), visual prompts (i.e., 4 inch × 6 inch quiet card), and reinforcers. Keri was taught to correctly identify her target behavior (i.e., vocaliza- tions) through modeling. The treatment provider mod- eled quiet and noisy behavior, asked Keri “Was I quiet or noisy?” (with gestures toward cards with the words quiet and noisy), reinforced correct responses and cor - rected errors. When Keri responded correctly during 8 of 10 trials for five consecutive sessions, Keri was then required to model quiet and noisy behavior in 8 of 10 trials (emphasis on quiet behavior), for three consecu- tive sessions (emphasis on quiet). Keri was then taught to assess target behavior using the self-recording sheet. Training and continued practice followed the instruction (i.e., “Get ready, show me quiet.”) and an instruction to record in the quiet box (or noisy box). Once Keri consistently marked the box that described the behavior she was modeling, she was taught self-recording using the watch, with initial intervals of 5 seconds, as the longest observed dura- tion that Keri could work, play, or sit without dis- playing the target behavior (vocalizations). The watch was started when the treatment provider gave the in- struction to work quietly (“Get ready. Show me quiet when you color.”). When the watch beeped, the treat-
- 145. ment provider stopped the watch, and Keri was asked “Were you quiet or noisy?”. When Keri responded (“quiet” or “noisy”) she was instructed to check that particular box (e.g., “That’s right. You were quiet. Check the quiet box.”). If Keri was incorrect in her re- sponse, she was verbally corrected and instructed to mark the appropriate box. Keri often said the word “quiet” during the interval. This was considered an ap- propriate verbalization. During intervals when Keri was noisy, the treatment provider prompted her to be quiet (e.g., “That’s noisy. Show me quiet. That’s bet- ter. That’s quiet.”). After Keri could successfully self-record her be- haviors when signaled by the watch, she was taught self-reinforcement.Before presentation of each new self-recording sheet, a variety of rewards (e.g., pop- corn, cereal, stickers, raisins,) were shown to Keri. Keri was instructed to (a) select six small rewards (six 602 Mancina, Tankersley, Kamps, Kravits, and Parrett in the interval beeps from 5 seconds to 10 seconds. The prompt-fading sequence was faded to, “Were you quiet or noisy?,” to “Check it,” and finally to a gestural prompt (a point to the paper). Also, verbal prompts to be quiet during the interval were only given during the intervals after Keri was noisy, and prompts were tied to the self-management procedure and materials. Cri- teria for implementation to the second (third) task was completion of the self-management steps, successful in- crease to 10-second intervals, and decreases in vo- calizations to 50% or less of the intervals for five sessions.
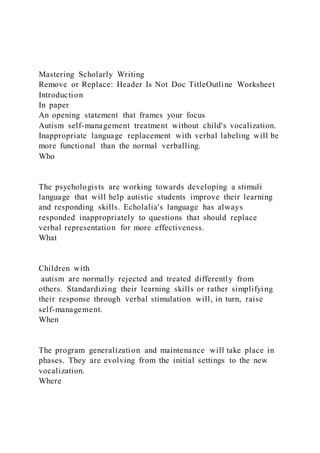
- 146. pieces of cereal, popcorn, raisins), (b) write the name of the reward at the top of the self-recording sheet, and (c) put the rewards on her desk above her self- recording sheet. Edibles were earned for quiet boxes. She was instructed to do the same for the one “spe- cial” reward (tape player, sticker, soda, or several pieces of the smaller rewards), which she selected to earn for reaching performance criteria (3 of 6 quiet intervals, then 4 of 6). Teaching independence in self-recordingfollow- ing successful self-management, consisted of (a) gradual fading of verbal prompts, and (b) an increase Fig. 1. Percentage occurrence of vocalizations during leisure, prevocational, and reading tasks for Study 1. Results and Discussion Overall the target behavior, vocalizations, decreased while collateral behaviors, facial and body movements, showed variable changes with minimal generalization of effects (Fig. 1 and Table I). During all tasks, the occur - rence of vocalizations, facial movements, and body movements ranged from 80–100% during baseline. Dur- ing the treatment phase for leisure tasks (28 sessions), self-management decreased vocalizations to 50% of the intervals or less after 18 sessions. When self-management was applied during prevocational tasks, the vocalizations decreased to less than 50% occurrence after four sessions, and continued to decrease to 20% occurrence or less. Dur- ing reading tasks, the occurrence of vocalizations once more decreased below 50% occurrence within the first
- 147. three sessions of self-management. Though vocalizations remained below 50% oc- currence, facial and body movements continued to occur at higher rates than the target behavior. As de- picted in Table I (means by condition, and last five ses- sions of treatment), no change in facial movements occurred following treatment for vocalizations during leisure tasks, with some generalization of effects to final sessions during prevocational and reading tasks. Limited generalization was noted in the occurrence of body movementsfollowing treatment for vocalizations. Keri’s self-injurious behavior was recorded during baseline and intervention. A total of 49 instances of self-injury were noted during sessions. The frequency was similar during baseline and treatment. Results from Self-Management Procedures Keri’s accuracy in self-recording her quiet and noisy behavior was recorded during treatment phases (5 sessions for leisure tasks, 3 sessions for prevocational Reduction of Inappropriate Vocalizations 603 tasks, and 4 sessions for reading tasks). She averaged 85% accuracy per session with a range of 78–92%. The initial teaching of the self-management steps required 6 days of intensive instruction for an average of 3 hours a day, with training continuing during the leisure tasks until Keri’s vocalizations decreased to 50% occurrence or less. Keri required 2 days of teaching before vocal - izations decreased to 50% occurrence during the prevo- cational tasks, and required only 1 day of teaching during reading. While vocalizations decreased, she did not reach independence, still needing verbal and gestural prompts
- 148. to use the program. STUDY 2: SELF-MANAGEMENT WITH THE TEACHER AS TREATMENT PROVIDER A continuation of self-management was conducted with Keri in Study 2, beginning in the fall term with in- corporation of the following procedures: (a) training the classroom teacher as treatment provider in the self-man- agement procedures, (b) lengthening the duration of the interval for quiet behavior, (c) increasing the number of intervals on the self-recording sheet, (d) gradually fad- ing verbal prompts to increase independence, (e) fading tangibles to natural reinforcers, and (f) fading the prox- imity and presence of the treatment provider. Participant, Setting, Design, and Procedures The teacher, a paraprofessional, and five students with autism, were present in the classroom. The class- room teacher had 11 years of teaching experience in special education classroom settings. Self-management procedures were implemented during scheduled class- room tasks involving leisure, prevocational, and read- ing activities, as in Study 1. Self-management procedures were conducted approximately 20–30 minutes a day, four to five times a week. Dependent Measures and Design.Dependent mea- sures were identical to those in Study 1 with the same definitions for the target and collateral behaviors. Oc- currence of inappropriate vocalizations, facial and body movements were recorded during continuous 10-second observations for 5-minute sessions. Observers for Study 2 included the first author and a research assistant with 9 years of teaching experience with children with
- 149. autism. Reliability was computed for 9% of the data files (14 of 137 sessions). Mean agreement was 91% (R = 83–100%) for vocalizations, 83% (R = 52–100%) for facial movements, and 80% (R = 67–100%) for body movements. A multiple-baseline design was used to evaluate treatment effects across tasks. Table I. Means for Facial and Body Movement, Self-Injurious Behavior Across Conditions During Study 1 Task Baseline Treatment for vocalizations Mean percentage occurrence—Facial Movements Leisure 89 83 (87, final 5 sessions) Pre-Voc 92 74 (68, final 5 sessions) Reading 94 84 (73, final 5 sessions) Mean percentage occurrence—Body Movements Leisure 83 84 (79, final 5 sessions) Pre-Voc 87 79 (82, final 5 sessions) Reading 95 89 (81, final 5 sessions) Frequency of self-injurious behavior Leisure 0.250 0.285 (0.00, final 5 sessions) Pre-Voc 0.060 0.625 (0.00, final 5 sessions) Reading 0.176 0.100 (0.20, final 5 sessions) Baseline. Baseline observations occurred during Keri’s regular leisure, prevocational and reading tasks with the same materials used in Study 1 and no self- management procedures. Self-Management Procedures.In Study 2, the role of the treatment provider was transferred to the class-
- 150. room teacher. Teacher training included (a) task analy- sis of each component of self-management procedures, (b) videotaped examples of the student using self-man- agement procedures, (c) modeling of prompting and self- management procedures by the first author, and (d) 604 Mancina, Tankersley, Kamps, Kravits, and Parrett monitoring and feedback concerning her performance as treatment provider for 5 days of training. Once the teacher training was completed, self-management pro- cedures identical to those used in Study 1 were imple- mented: (a) identification of target behavior, (b) recording of the target behavior, (c) self-recording using the watch, and (d) self-reinforcement. During the treatment phase, the number of self- recording boxes per page was increased from 6 to 10. The duration of intervals ranged from 10–40 seconds, and was variable throughout all treatment phases. If Keri Fig. 2. Percentage occurrence of vocalizations during leisure, prevocational, and reading tasks for Study 2. Reduction of Inappropriate Vocalizations 605 exhibited vocalizations and was not successful (i.e., did not earn a reward using the self-management procedures) on three consecutive self-recording sheets, the duration of the interval was lowered. Also, the number of suc- cessful (i.e., quiet) intervals required to receive a reward was increased to 8 of 10 quiet intervals. In Study 2, limited independence with self-man-
- 151. agement procedures was obtained. Verbal prompts and gestural prompts were faded; however, Keri frequently required gestural prompts toward the end of the ses- sions. Because Keri continued to require prompts to re- main on-task, proximity by the treatment provider was limited to the area within the classroom. Results and Discussion In Study 2, vocalizations decreased, facial move- ments remained unchanged, and body movements de- creased. As depicted in Figure 2, baseline levels of vocalizations were high (76–97%), with a decrease to 41% occurrence in the first treatment session, and con- tinued decreases to near zero levels. Self-management during prevocational tasks decreased vocalizations to below 20% after the first treatment session, with zero levels during several sessions of the treatment phase. During reading, vocalizations decreased to lower lev- els; however, the decrease was variable, ranging from 0–60% occurrence. An increase in final sessions ap- peared to be related to task difficulty. Facial movements showed some variability but continued to occur at higher rates than vocalizations. Body movements de- creased to lower levels during treatment for vocaliza- tions, indicating some generalization of treatment effects. Self-injurious behavior was somewhat lower during the Study 2 period, except during frustrating tasks (see Table II). GENERAL DISCUSSION Similar to positive findings in prior research (e.g., R. L. Koegel & Koegel, 1990; Reese, Sherman, & Shel- don, 1984), self-management was highly effective in
- 152. decreasing inappropriate vocalizations. In general, treatment effects were slower during the initial program (Study 1, Task 1) with quicker results for the second and third tasks and during Study 2. In addition, both teachers reported that Keri was much quieter with more appropriate behavior when using the self-management program. Generalization of treatment effects were noted for one of two collateral behaviors. Though the findings were encouraging, a limitation was that Keri did not learn complete independence, nor were procedures able to be faded within the period of study. Larger changes in tar- get and collateral behaviors may have been obtained with (a) the use of behavioral programming to address behav- iors such as noncompliance, (b) an augmentative com- munication system, and (c) programs to increase social competencies. Longer treatment may also be necessary for students with (a) lower cognitive ability, (b) high rates of challenging behaviors, rates, and (c) a long his- tory of behaviors with insufficient interventions (R. L. Koegel, Koegel, Van Voy, & Ingham, 1988). ACKNOWLEDGMENT This research was supported by the Office of Spe- cial Education and Rehabilitation Services, U.S. De- partment of Education, Grant H023C00024 to the University of Kansas. REFERENCES Gardner, W. I., Clees, T. J., & Cole, C. L. (1983). Self- management of disruptive verbal ruminations by a mentally retarded adult. Applied Research in Mental Retardation, 4, 41–58. Kazdin, A. E. (1984). Behavior modification in applied settings
- 153. (3rd ed.). Homewood, IL: Dorsey. Koegel, L. K., Koegel, R. L., Hurley, C., & Frea, W. D. (1992). Im- proving social skills and disruptive behavior in children with autism through self-management. Journal of Applied Behavior Analysis, 25, 341–354. Koegel, R. L., & Frea, W. D. (1993). Treatment of social behavior in autism through the modification of pivotal social skills. Jour - nal of Applied Behavior Analysis, 26, 367–377. Koegel, R. L., & Koegel, L. K. (1990). Extended reductions in stereo- typic behavior of students with autism through a self-manage- ment treatment package. Journal of Applied Behavior Analysis, 23, 119–128. Table II. Means for Facial and Body Movements, Self-Injurious Behavior Across Conditions During Study 2 Task Baseline Treatment for vocalizations Mean percentage occurrence—Facial Movements Leisure 71 72 (62, final 5 sessions) Pre-Voc 84 82 (89, final 5 sessions) Reading 83 80 (78, final 5 sessions) Mean percentage occurrence—Body Movements Leisure 71 52 (35, final 5 sessions) Pre-Voc 82 66 (58, final 5 sessions) Reading 85 74 (59, final 5 sessions) Frequency of self-injurious behavior Leisure 0.000 0.090 (0.00, final 5 sessions)
- 154. Pre-Voc 0.000 0.000 (0.00, final 5 sessions) Reading 0.420 1.500 (2.80, final 5 sessions) 606 Mancina, Tankersley, Kamps, Kravits, and Parrett munity group homes: The role of self-recording and peer- prompted self-recording. Analysis and Intervention in Develop- mental Disabilities, 4, 91–107. Shapiro, E. S., McGonigle, J. J., & Ollendick, T. (1980). An analy- sis of self-assessment and self-reinforcement in a self-managed token economy with mentally retarded children. Applied Re- search in Mental Retardation, 1, 227–240. Stahmer, A. C., & Schreibman, L. (1992). Teaching children with autism appropriate play in unsupervised environments using a self-management treatment package. Journal of Applied Be- havior Analysis, 25, 447–459. Wechsler, D. (1974). Manual for the Wechsler Intelligence Scale for Children-Revised. San Antonio: Psychological Corp. Koegel, R. L., Koegel, L. K., & Parks, D. R. (1990). How to teach self-management skills to people with severe disabilities: A training manual. Unpublished manuscript, University of Cali- fornia, Santa Barbara. Koegel, R. L., Koegel, L. K., Van Voy, K., & Ingham, J. C. (1988). Within-clinic versus outside-of-clinic self-monitoring of artic-
- 155. ulation to promote generalization. Journal of Speech and Hear - ing Disorders, 53, 392–399. Newman, B., Buffington, D. M., O’Grady, M. A., Poulson, C. L., & Hemmes, N. S. (1995). Self-management of schedule following in three teenagers with autism. Behavior Disorders, 20, 190– 196. Reese, R. M., Sherman, J. A., & Sheldon, J. (1984). Reducing agi- tated-disruptive behavior of mentally retarded residents of com- Copyright of Journal of Autism & Developmental Disorders is the property of Springer Science & Business Media B.V. and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. 3
- 156. Academic Journal Observations Cassandre Moise Capella University Description of the Writing in Journals 1. Scope; Main Ideas The combined objectives of ABA field journals reviewed is to predict and control behaviours regarded crucial socially. Each of the journal articles contend to sufficiently cover the various subfields of ABA field of study .They are all aligned to the basic goal of enhancing performance through alteration of environmental factors influencing socially important behaviours. In addition, the articles covers components of ABA field for instance, shaping, prompting, chaining and prompt fading. Lastly, the articles covers the dimensions of ABA and their relevance.
- 157. 2. Structure APA format is effectively applied in the Journal articles to clearly provide significant understanding of the field’s diverse and complex topics. The ideas concerning ABA field are presented with optimal clarity for a wide range of readers to conceptualize the basics. Paragraphs are written long to detailed but a brief to the point description of the individual subject. An average the articles have 4 to 6 sentences paragraphs (APA style).In addition, the article bodies are well structured with suitable introduction and conclusions of their topic coverage. 3. Comparison of Ideas and Styles in the Journals Application of other styles apart from APA facilitates broad presentation of the main ideas covered in the journal articles. In contrast, the content of particular theme of ABA may slightly vary from one journal to another. Furthermore authors have highlighted their ideas through cautious, well researched and convincing discussions that genuinely captures the reader’s attention. It is evident that the nature of content presentation quietly affects the reader’s morale and captivation to continue reading about a certain article topic. References Averina, M., Nilssen, O., Brenn, T., Brox, J., Arkhipovsky, V. L., & Kalinin, A. G. (2005). Social and lifestyle determinants of depression, anxiety, sleeping disorders and self-evaluated quality of life in Russia. Social Psychiatry and Psychiatric Epidemiology, 40(7), 511-518. Kodak, T., & Piazza, C. C. (2008). Assessment and behavioral treatment of feeding and sleeping disorders in children with autism spectrum disorders. Child and adolescent psychiatric clinics of North America, 17(4), 887-905. Van Tongerloo, M. A., Bor, H. H., & Lagro-Janssen, A. L. (2012). Detecting autism spectrum disorders in the general practitioner’s practice. Journal of autism and developmental
- 158. disorders, 42(8), 1531-1538. Drafting Your Text Scoring Guide Due Date: Unit 5 Percentage of Course Grade: 10%. CRITERIA NON-PERFORMANCE BASIC PROFICIENT DISTINGUISHED Introduce thesis within context for appropriate audience. 25% Does not introduce thesis within context for appropriate audience. Introduces thesis, but the context is not clearly connected to
- 159. the appropriate audience. Introduces thesis within context for appropriate audience. Introduces thesis within context for appropriate audience, providing a clear connection to the topic, purpose, and aspects. Incorporate evidence with coherent placement that supports structure of arguments. 25% Does not incorporate evidence with coherent placement that supports structure of arguments. Incorporates evidence in only a basic fashion, lacking evidence- based reasoning.
- 160. Incorporates evidence with coherent placement that supports structure of arguments. Incorporates evidence with coherent placement that supports the structure of arguments, using clear and direct reasoning. Present a clear and complete argument. 25% Does not present a clear and complete argument. Presents only a basic argument. Presents a clear and complete argument. Presents a well-developed, clear and complete argument. Utilize proper mechanics including spelling, grammar,
- 161. and APA formatting 25% Does not utilize proper mechanics including spelling, grammar, and APA formatting. Utilizes most, but not all, proper mechanics including spelling, grammar, and APA formatting. Utilizes proper mechanics including spelling, grammar, and APA formatting. Utilize proper mechanics including spelling, grammar, and APA formatting in a comprehensive and informed fashion.