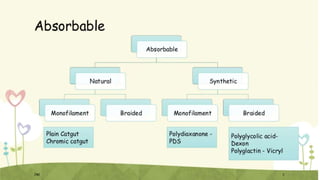
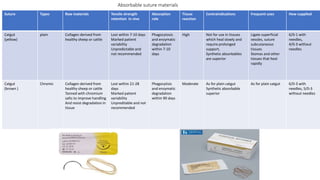
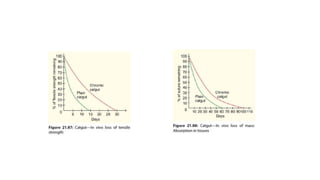
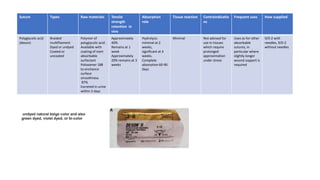
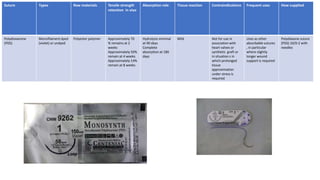
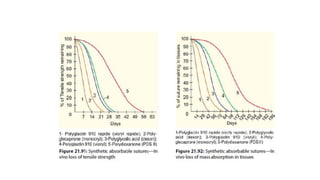
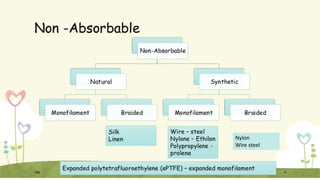
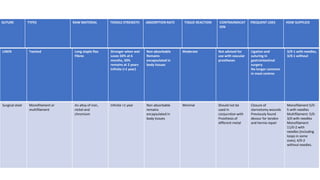
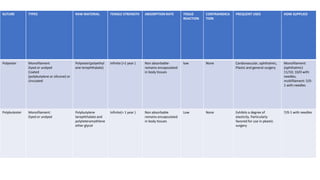
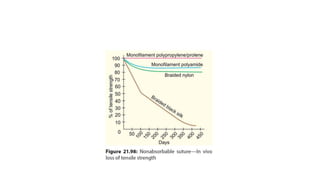
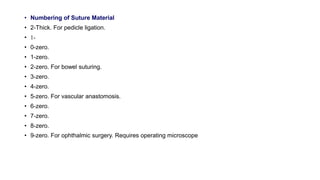
This document discusses various suture materials including absorbable and non-absorbable options. Absorbable materials such as catgut, polyglactin 910 (Vicryl), and polyglycolic acid (Dexon) are broken down by the body over time through processes like hydrolysis and enzymatic degradation. Non-absorbable materials like silk and nylon provide long-term tensile strength but can cause tissue reactions. The ideal suture is strong, minimally reactive, easy to use, and affordable. Sutures are available with or without needles in a range of sizes for different surgical applications.