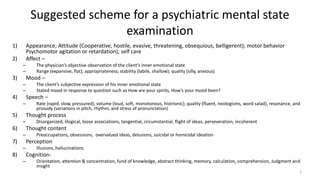
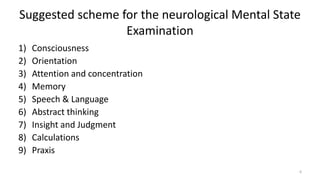
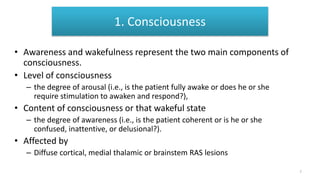
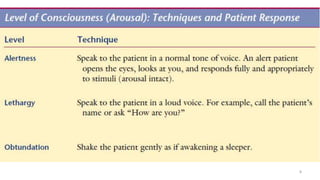
This document provides an overview of a presentation on mental state examinations. It outlines learning objectives, suggested schemes for psychiatric and neurological examinations, and details on specific components of the neurological examination including consciousness, orientation, attention, memory, speech and language, abstract thinking, and calculations. Examples of tests that can be used to evaluate each component are also described.