Adapting Managed Care Strategies in the Era of Precision Medicine for Hypertrophic Cardiomyopathy
•
0 likes•5 views

Co-Chairs Milind Desai, MD, MBA, FACC, FAHA, FESC, and Andrew Willeford, PharmD, PhD, BCCP, prepared useful Practice Aids pertaining to hypertrophic cardiomyopathy for this CME/MOC/CPE/AAPA/IPCE activity titled “Adapting Managed Care Strategies in the Era of Precision Medicine for Hypertrophic Cardiomyopathy.” For the full presentation, downloadable Practice Aids, and complete CME/MOC/CPE/AAPA/IPCE information, and to apply for credit, please visit us at https://bit.ly/4bb7eKc. CME/MOC/CPE/AAPA/IPCE credit will be available until May 16, 2025.

Recommended
More Related Content
Similar to Adapting Managed Care Strategies in the Era of Precision Medicine for Hypertrophic Cardiomyopathy
Similar to Adapting Managed Care Strategies in the Era of Precision Medicine for Hypertrophic Cardiomyopathy (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Adapting Managed Care Strategies in the Era of Precision Medicine for Hypertrophic Cardiomyopathy
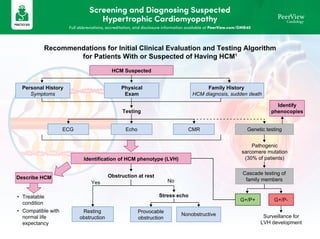
- 1. Screening and Diagnosing Suspected Hypertrophic Cardiomyopathy Full abbreviations, accreditation, and disclosure information available at PeerView.com/DMR40 Recommendations for Initial Clinical Evaluation and Testing Algorithm for Patients With or Suspected of Having HCM1 Testing ECG Resting obstruction Echo Provocable obstruction CMR Nonobstructive Identification of HCM phenotype (LVH) Obstruction at rest Stress echo Yes No HCM Suspected Personal History Symptoms Physical Exam Family History HCM diagnosis, sudden death Describe HCM • Treatable condition • Compatible with normal life expectancy Genetic testing Pathogenic sarcomere mutation (30% of patients) Cascade testing of family members Identify phenocopies G+/P+ G+/P- Surveillance for LVH development
- 2. Screening and Diagnosing Suspected Hypertrophic Cardiomyopathy Full abbreviations, accreditation, and disclosure information available at PeerView.com/DMR40 1. Maron BJ et al. J Am Coll Cardiol. 2022;79:372-389. 2. Ommen SR et al. Circulation. 2020;142:e533-e557. Cascade Screening and Longitudinal Follow-Up for HCM2 Selected HCM Genetic Screening Tests • Invitae: invitae.com – Hypertrophic Cardiomyopathy Panel (30-44 genes) – Cardiomyopathy Comprehensive Panel (82-112 genes) • GeneDx: genedx.com – Hypertrophic Cardiomyopathy (HCM) Panel (42 genes) – Cardiomyopathy Panel (102 genes) • Blueprint Genetics: blueprintgenetics.com – HCM Panel (92 genes) – Cardiomyopathy Panel (217 genes) HCM Suspected or Family Hx of HCM Diagnostic testing (ECG, imaging, genetic) Phenotype negative Phenotype positive Family with known P/LP variant? Patient has family variant? Further clinical or genetic testing is not recommended Reassess variant classification Screening ECG and echo (CMR if echo is inconclusive) at the intervals in the table below Treadmill or bike exercise testing • Stress echo if gradient <50 mmHg • CPET if considering advanced HF therapies Every 1-2 y or with change in symptoms Serial evaluation for clinical status, SCD risk (if no ICD present), or sooner with change in symptoms • Clinical assessment • Echo • Holter Every 2-3 y Treadmill exercise or cardiopulmonary exercise testing for assessment of functional status Every 3-5 y CMR for SCD risk assessment (if no ICD present) or to evaluate for any suspected morphologic changes Variant = P/LP Variant downgraded to VUS Asymptomatic Symptomatic No Yes No Yes or unknown Surveillance Interval Initiation of Screening Age of First-Degree Relative Every 1-2 y At the time of diagnosis in another family member Children and adolescents from genotype-positive family and/or family with early onset HCM Every 2-3 y At any time after the diagnosis in the family, but no later than puberty All other children and adolescents Every 3-5 y At the time of diagnosis in another family member Adults Screening Asymptomatic First-Degree Relatives of Patients With HCM 1 2 3 4 5 HCM Index Case Targeted Gene Testing Disease-causing P/LP variant VUS, B/LB, or no variant identified Regular follow-up See 2 Reclassified as P/LP Reclassified as VUS or B/LB Consider second tier testing in proband if no variant is identified Cascade genetic testing in family Clinical surveillance in family Variant positive Variant negative HCM diagnosed No evidence of HCM Regular evaluation for variant reclassification See 4 Regular follow-up See 2 Regular clinical surveillance See 5 Further clinical or genetic testing not recommended See 3
- 3. Distinguishing Imaging Features of Various Cardiomyopathies1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/DMR40 1. Galluzzo A et al. Life. 2023;13:171. Athlete’s Heart Hypertensive Cardiomyopathy Fabry Cardiomyopathy Amyloidosis Hypertrophic Cardiomyopathy Transthoracic Echocardiography • Harmonic, eccentric LVH • Enlargement of all cardiac chambers • Concentric LVH • LV wall thickness usually <15 mm • Concentric LVH • PM hypertrophy • RV hypertrophy • Concentric LVH with granular sparkling aspect • High-degree diastolic dysfunction • Apical sparing at STE • Asymmetric LVH • Possible LVOT obstruction Cardiac Magnetic Resonance • Normal findings (ie, harmonic LVH with no LGE) • LGE: mid-myocardium (arrow) and epicardium • LGE: typical basal inferolateral mid-wall (arrows); patchy areas may be present • LGE: subendocardial; in ATTR possible transmural pattern and RV involvement (arrow) • LGE: Frequent, often mid- myocardial and epicardial in the areas of maximal LVH (arrows)
- 4. Recognizing and Treating Common Comorbidities of Hypertrophic Cardiomyopathy1-8 Full abbreviations, accreditation, and disclosure information available at PeerView.com/DMR40 Consequences Prevalence Comorbidity • May increase LV mass, but rarely increases LV thickness >16 mm • HCM is accompanied by mitral valve abnormalities not found in hypertensive cardiomyopathy • Highly prevalent in the general population • May also be present in patients with unequivocal HCM Hypertension • Worsens hemodynamics of HCM, increases symptom burden • Reported in up to 70% of patients with HCM Sleep apnea • Increases LV mass, more rapid clinical progression, worsens HF symptoms, increases risk of AF (especially in middle-aged adults) • More common in HCM than in general population • oHCM observed in >50% with BMI >30 Obesity • Major prognostic indicator, associated with increased overall mortality, SCD, and cardiac events • Myocardial ischemia is often observed in patients with HCM CAD • Higher BMI, LA volume, and moderate-to-severe MR; increased risk of AF events • Common in HCM; more likely with MYH7 sarcomere variants Atrial fibrillation Optimizing treatment of comorbidities can reduce symptom severity in patients with oHCM Common Comorbidities of oHCM Encountered in Community Practice at Baseline 59% 35% 19% 9% 9% 9% 7% 6% 5% HTN CAD DM CKD Syncope Vt/VF PAD MI Stroke Proportion of Patients, % 80 60 40 20 0
- 5. Recognizing and Treating Common Comorbidities of Hypertrophic Cardiomyopathy1-8 Full abbreviations, accreditation, and disclosure information available at PeerView.com/DMR40 a The standards for control of modifiable CV risk factors should arguably recapitulate those used for secondary prevention in patients with CAD, in all genetic cardiomyopathies, based on the principle that superimposed ASCVD seems to have synergistic rather than additive effects. b 1 RM corresponds to the maximum weight that can be lifted throughout the entire exercise movement only one time. 1. Finocchiaro G et al. J Am Heart Assoc. 2017;6:e007161. 2. Kramer CM et al. J Am Coll Cardiol EP. 2021;7:1376-1386. 3. Lee SP et al. Circ Heart Fail. 2018;11:e005191. 4. Marstrand P et al. Circulation. 2020;141:1371-1383. 5. Butzner M et al. Am J Cardiol. 2022;174:120-125. 6. Arbelo E et al. Eur Heart J. 2023;44:3503-3626. 7. Finocchiaro G et al. J Am Heart Assoc. 2017;6:e007161. 8. Cavigli L et al. Eur J Prev Cardiol. 2021;28:1093-1099. Proposed Management of Modifiable Risk Factors in Patients With HCM Possible Effects Lifestyle/Clinical Variable ↓ risk of CAD ↓ risk of MI LDL <100 mg/dLa ↓ risk of secondary LVH caused by increased afterload BP <130/80 mmHga ↑ diastolic function ↑ exercise capacity ↓ risk of obesity Moderate exercise ↓ risk of obesity ↓ risk of development of a more marked LVH caused by increased afterload Weight management Key Recommendations for Exercise Prescription in HCM • From 150-300 min/wk of low-to-moderate endurance exercise, 3-5 d/wk, depending on weekly volume • All sessions must be preceded by a 5-min warm-up phase and end with a 5-min cool-down • Muscle-strengthening activities of low-to-moderate intensity that involve all major muscle groups on 2 d/wk • Flexibility training should be performed at least 2-3x/wk (eg, stretching muscle groups 4x for 10-20 s each) Frequency and duration • Low-to-moderate endurance training (training volume should be emphasized more than intensity) • Resistance training intensity should correspond to 40%-70% of 1 RMb • Repetition set should be stopped before the point at which it would be difficult to perform another repetition Intensity Tailor patient progression based on adaptation to exercise, previous training experience, age, and clinical characteristics Progression • Start with a weekly session and introduce the second session when the patient is adapted (optimal frequency is 3-4x/wk of endurance exercise) Frequency • Start with 10-30 min of endurance exercise and increase 10 min every week to reach the optimal weekly training duration (3-4 wk based on individual response to exercise) Duration • Start at low intensity during the first 3-4 wk, first increasing the volume and then intensity • Resistance exercises should start gradually with 1-3 sets of 8-10 exercises at slow-moderate velocity Intensity
- 6. Considerations for Using Approved Cardiac Myosin Inhibitors in the Management of HCM Full abbreviations, accreditation, and disclosure information available at PeerView.com/DMR40 First-line therapies Advanced therapies Mavacamten2,3,a (EXPLORER-HCM) + Yes No Still SRT eligible? No Yes Disopyramideb SRT willing? Functional capacity improves with mavacamten whether or not β-blockers are used4 Myectomy Myectomy or ablation Ablation Mavacamten3,5,a (VALOR-HCM) Re-evaluate in 1-2 years Symptoms with NYHA class III/IV or II with near or exertional syncope on maximally tolerated therapy? β-blockade Verapamil or diltiazem Treat comorbidities Symptoms? Avoid vasodilators and diuretics Other indication? Yes Yes Yes Yes Yes No No No No Surgical candidate? Where Do Approved Cardiac Myosin Inhibitors Fit in the Management of oHCM?1-6
- 7. Considerations for Using Approved Cardiac Myosin Inhibitors in the Management of HCM Full abbreviations, accreditation, and disclosure information available at PeerView.com/DMR40 Suggested Multidisciplinary Approach to the Management of Mavacamten in oHCM7 This multidisciplinary workflow can efficiently address cost limitations for most patients considering mavacamten. Use this template in your HCM center to initiate your own mavacamten program. Physician assesses patient for initiation with mavacamten Pharmacist assesses drug interactions and need for contraception Pharmacist counsels patient using the REMS brochure and enrolls patient into the REMS program online • Write initiation note Pharmacist / Nurse enrolls patient into support programs and submits prior authorization Pharmacist checks approval and cost Pharmacist discusses cost and sets treatment start date with patient Nurse / Echo Coordinator orders weeks 4, 8, and 12 echos • Use echo date calculator • Create echo due date reminders Pharmacist / Physician assesses echo report • Refer to PI for dosing Pharmacist calls the patient • Assess symptoms and adverse events • Assess new drug interactions • Submit REMS patient status form online • Write note and submit prescription Nurse / Echo Coordinator orders follow-up echocardiograms • Refer to PI for echo timing • Use echo date calculator Repeat for weeks 8 and 12 Repeat for all subsequent echos
- 8. Considerations for Using Approved Cardiac Myosin Inhibitors in the Management of HCM Full abbreviations, accreditation, and disclosure information available at PeerView.com/DMR40 Mavacamten: Examples of Known Drug-Drug Interactions8 Over-the-Counter Medications/Nutritional Supplements Grapefruit juice Esomeprazole (Nexium) Omeprazole (Prilosec) St. John’s wort Cimetidine (Tagamet) Prescription Medications Clarithromycin (Biaxin) Boceprevir Fluconazole (Diflucan) Phenytoin (Dilantin) Apalutamide (Erleada) Felbamate (Felbatol) Telaprevir (Incivek) Etravirine (Intelence) Telithromycin (Ketek) Phenobarbital (Luminal) Fluvoxamine (Luvox) Mitotane (Lysodren) Primidone (Mysoline) Nefazodone Esomeprazole (Nexium) Ketoconazole (Nizoral) Ritonavir (Norvir) Posaconazole (Noxafil) Omeprazole (Prilosec) Fluoxetine (Prozac) Rifampin (Rifadin) Itraconazole (Sporanox) Efavirenz (Sustiva) Troleandomycin (Tao) Cimetidine (Tagamet) Carbamazepine (Tegretol) Ticlopidine (Ticlid) Bosentan (Tracleer) Voriconazole (Vfend) Nelnavir (Viracept) Enzalutamide (Xtandi) Idelasib (Zydelig) This is not a comprehensive list. For more information, please refer to the full prescribing information.
- 9. Considerations for Using Approved Cardiac Myosin Inhibitors in the Management of HCM Full abbreviations, accreditation, and disclosure information available at PeerView.com/DMR40 a Mavacamten is a first-in-class cardiac myosin inhibitor that was FDA-approved after the 2020 AHA/ACC guidelines were published; for further information on this agent, please refer to its prescribing information. b AHA/ACC guidelines do not stipulate NYHA class or maximal therapy. 1. Ommen SR. ACC 2022. Oral presentation: 683-611. 2. Olivotto I et al. Lancet. 2020;396:759-769. 3. Camzyos (mavacamten) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/214998s001lbl.pdf. 4. Wheeler MT et al. Eur J Heart Fail. 2022;25:260-270. 5. Desai MY et al. J Am Coll Cardiol. 2022;80:95-108. 6. Arbelo E et al Eur Heart J. 2023;44:3503-3626. 7. Willeford A et al. Circulation. 2023;148:A15539. 8. https://www.camzyosrems.com/assets/commercial/us/camzyosrems/en/pdf/Camzyos-REMS-Patient-Brochure.pdf. 9. https://www.cms.gov/medicare/coding-billing/icd-10-codes/2024-icd-10-cm. oHCM Information Checklist for Mavacamten Approval Applications3,9 Use this checklist when working with the patient's insurance company to secure drug coverage (eg, prior authorization, letter of medical necessity, letter of appeal). Always check with the insurance company and their drug policies for specific requirements. Patient information (name, DOB, contact information, member ID, case #) ICD-10 code(s) oHCM: I42.1 HF: Choose the appropriate code from the I50 code section Confirmation the patient is 18 years or older and not pregnant Patient's history and current condition (eg, symptoms associated with symptomatic oHCM, signs of oHCM observed via echos, relevant comorbidities) Previous and/or current treatments for oHCM (eg, β blockers, CCBs) LVOT pressure documentation LVEF documentation Confirmation of no DDIs Confirmation the patient understands the requirements of and is enrolled in the REMS program Confirmation the provider and pharmacy are enrolled in the REMS program