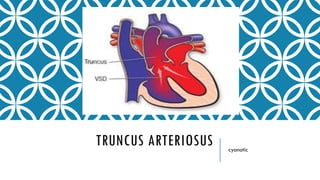
2. DEFINITION
A single trunk arising from the heart
Supplying the coronary, pulmonary, and systemic circulations
No remnants of an atretic aorta or pulmonary artery, attached to
both ventricles
Overriding the ventricular septum due to failure of the Truncus
arteriosus to divide during in the embryonic period
3. HISTORY
Wilson : 1st description in 1798
Buchannan : Clinical & autopsy report in 1864
Collett & Edwards : Classification in 1949
Van Praagh : Alternative classification in 1965
McGoon : 1st repair with homograft in 1967
4. QUICK ANATOMY
Single artery arising from the two ventricles which gives rise to both the aortic and
pulmonary vessels
Abnormal truncal valve
Right sided aortic arch in about 30% of cases (not shown)
Large ventricular septal defect
Pulmonary hypertension
Complete mixing occurring at level of the great vessel
Right-to-left shunting of blood
5. BLAMED
Baltimore-Washington Infant Study: maternal cigarette smoke(odds ratio [OR]: 1.9,
95% CI 1.04-3.45)
Texas Birth Defects Registry (1999 to 2004): advancing maternal age
22q11.2 deletions: Deletions in three genes in this locus (TBX1, CRKL, and ERK2)
cause neural crest cell and anterior heart anomalies seen in patients with DiGeorge
syndrome
Retinoic acid
Bismuth
6. EMBRYOLOGY
Defect in the development of the truncoconal[more conal than Truncus] septum result
in Conotruncal abnormalities including Truncus arteriosus
Neural crest hypothesis
Bulbar septum is deficient just below the singular truncal=semilunar valve
7. INCIDENCE
40% trunk connects predominantly with the right ventricle
40% overriding is symmetrical
20% trunk connects mainly with the left ventricle
Prevalence:0.3:10,000 births
12 times higher in women with pregestational diabetes mellitus
Sibling recurrence is 1/100
6 to 10 per 100,000 live births
0.7 percent of all CHD
4 % of all critical CHD.
10. HOW THE PULMONARY ARTERY IS CONNECTED TO
THE TRUNCUS?
Type 1: a single pulmonary vessel originates from the arterial trunk and bifurcates
in left and right pulmonary arteries.
Type 2: the pulmonary arteries originate from the back of the Truncus
Type 3: the pulmonary arteries originate on each side of the Truncus
Type 4: absent pulmonary arteries; collaterals originate from the systemic
circulation, most frequently from the descending aorta
Collet RW, Edwards JE. Persistent truncus arteriosus: a classification according to anatomic types.
Surg Clin North Am 1949;29:501-10
11. VSD OR NO VSD[SOCIETY OF THORACIC
SURGEONS (STS) ]
TYPE A[VSD+] TYPE B[VSD-]
A1: As CE type 1, in which a main pulmonary artery is present, and
arises from the left side of the truncal root.
A2: h CE types II and III, as the two CE types do not differ
embryologically and the surgical approach is the same. Type A2
consists of right and left branch pulmonary arteries with separate
origins (regardless of the distance separating the two pulmonary
arteries) from the truncal root.
A3: Unilateral pulmonary atresia with collateral supply to the
affected lung.
A4:Interrupted aortic arch
Van Praagh R, Van Praagh S. The anatomy of common aorticopulmonary trunk (truncus arteriosus communis) and its
embryologic implications: a study of 57 necropsy cases. Am J Cariol 1965;16:406-26
15. HEMODYNAMIC
Hemodynamic is not affected during intrauterine life
Cardiac failure occurs after birth because of the fall in blood pressure in the
pulmonary circulation leads to medical emergency
Pulmonary vascular obstructive disease may develop in surgically uncorrected
patients with large pulmonary blood flow, with changes noted as early as six months
of age
Coronary under perfusion due to AR and pulmonary run off
16. NATURAL HISTORY
a mean age of death at five weeks
survival of only 15 percent at one year of age
beyond the first year of life develop severe pulmonary vascular obstructive disease
17. SYMPTOMS
Bluish skin (cyanosis)
Delayed growth or growth failure
Fatigue
Lethargy
Poor feeding
Rapid breathing (tachypnea)
Shortness of breath (dyspnoea)
Widening of the finger tips (clubbing)
18. SIGNS
Cyanosis presents at birth
Heart failure may occur within weeks
Systolic ejection murmur is heard at the left sternal border
Widened pulse pressure
Bounding arterial pulses
Loud second heart sound
Biventricular hypertrophy
Cardiomegaly
Increased pulmonary vascularity
Hypocalcemia (if associated with DiGeorge syndrome)
19. ASSOCIATED
Up to 50% of the cases, including unilateral renal agenesis or hypoplasia, absent
gallbladder, pulmonary hypoplasia and cleft palate
DiGeorge, velocardiofacial (DFG/VCFS) and conotruncal anomaly face syndromes
(CTAFS) are associated with conotruncal anomalies
Aortic arch anomalies :Right aortic arch – 21 to 36%,Interrupted aortic arch – 11
to 19 percent,Hypoplastic aortic arch (with or without coarctation of the aorta) – 3
percent
Secundum ASD:9 to 20%, mild tricuspid stenosis:6%, aberrant subclavian arteries: 4
to 10%, persistent LSVC :4 to 9% and PDA :50%
21. TREATMENT
Initial medical management Surgery
Treat heart failure due to large left to right shunt Connect pulmonary artery[right ventricle to
pulmonary artery (RV-PA) conduits ] to right
ventricle
Primary surgical repair during the neonatal period
(less than 30 days of age) has led to an improved
survival rate at one year of age of greater than
80 percent compared with the 15 percent rate
observed in uncorrected patients