

Recommended
More Related Content
What's hot
Viewers also liked
Viewers also liked (20)
Similar to 23205039
Similar to 23205039 (20)
23205039
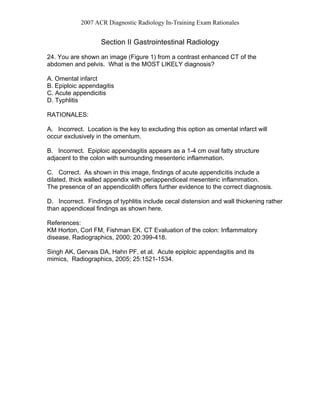
- 1. 2007 ACR Diagnostic Radiology In-Training Exam Rationales Section II Gastrointestinal Radiology 24. You are shown an image (Figure 1) from a contrast enhanced CT of the abdomen and pelvis. What is the MOST LIKELY diagnosis? A. Omental infarct B. Epiploic appendagitis C. Acute appendicitis D. Typhlitis RATIONALES: A. Incorrect. Location is the key to excluding this option as omental infarct will occur exclusively in the omentum. B. Incorrect. Epiploic appendagitis appears as a 1-4 cm oval fatty structure adjacent to the colon with surrounding mesenteric inflammation. C. Correct. As shown in this image, findings of acute appendicitis include a dilated, thick walled appendix with periappendiceal mesenteric inflammation. The presence of an appendicolith offers further evidence to the correct diagnosis. D. Incorrect. Findings of typhlitis include cecal distension and wall thickening rather than appendiceal findings as shown here. References: KM Horton, Corl FM, Fishman EK. CT Evaluation of the colon: Inflammatory disease, Radiographics, 2000; 20:399-418. Singh AK, Gervais DA, Hahn PF, et al. Acute epiploic appendagitis and its mimics, Radiographics, 2005; 25:1521-1534.
- 2. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 25. You are shown two images from a contrast enhanced CT (Figures 2A and 2B). What is the diagnosis? A. Acute hepatic infarction B. Confluent hepatic fibrosis C. Focal hepatic steatosis D. Hepatic metastasis RATIONALES: A. Incorrect. Although hepatic infarcts will be wedge shaped in contour, the presence of fat attenuation is not characteristic. B. Incorrect. Confluent hepatic fibrosis radiates from the porta hepatis to the hepatic dome and causes retraction of the overlying capsule. C. Correct. As is this example, focal hepatic steatosis demonstrates a wedge- shaped contour, produces no mass effect, and portal and hepatic veins course through the lesion in a normal pattern. D. Incorrect. Metastases are usually more rounded in contour, would usually be of higher attenuation, and would cause distortion, displacement of nearby vasculature. References: Computed Body Tomography with MRI Correlation, Lee JKT, Sagel SS, Stanley RJ, Heiken JP, eds. Philadelphia, PA: Lippincott-Raven, 1998; 705-711
- 3. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 26. You are shown an image from an abdominal CT (Figure 3) performed in a 42 year-old man with a long history of Crohn’s disease, who now presents with abdominal pain and distention. What is the MOST LIKELY diagnosis? A. Crohn’s colitis B. Metastatic adenocarcinoma C. Abscess perforation with peritonitis D. Small bowel obstruction RATIONALES: A. Incorrect. The ascending and descending colon are opacified by oral contrast and are unremarkable. The irregular band of soft tissue density in the anterior periphery of the peritoneal cavity is an omental cake. B. Correct. The images show ascites and an omental cake compatible with peritoneal carcinomatosis. The most likely primary in a male patient of this age with this history of Crohn’s disease is a small bowel adenocarcinoma. The heterogeneous mass anterolateral to the left iliac vessels is a surgically proven ileal adenocarcinoma, though I would not expect the observer to recognize this from this single image. “The risk for the development of small bowel adenocarcinoma is greater in patients with Crohn’s disease than in the general population although the magnitude of this increased risk is unclear. Risk factors associated with the development of small bowel carcinoma in Crohn’s disease include male sex, duration of disease, associated fistulous disease, and the presence of surgically excluded loops of bowel. Crohn’s colitis has been associated with an increased risk of colorectal carcinoma in patients with long- standing colitis, strictures, fistulae, and right-sided colonic disease.” (1) C. Incorrect. While intraperitoneal perforation of abscess with infection may complicate Crohn’s disease, this is extremely rare. While it would cause free fluid, it would not cause an omental cake. D. Incorrect. While small bowel obstruction may complicate Crohn’s disease, the bowel dilatation in this patient is due to short gut and not obstruction. It does not account for the signs of peritoneal carcinomatosis. References: Bernstein D, Rogers A. Malignancy in Crohn’s disease. Am J Gastroenterol 1996;91(3):434-40. Greenstein AJ, Sachar DB, Mann D, et al. Spontaneous free perforation and perforated abscess in 30 patients with Crohn's disease. Ann Surg 1987;205(1):72-6.
- 4. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 27. You are shown CT images (Figures 4A and 4B) from a 24-year-old woman who presented with acute onset severe mid-epigastric pain, nausea, vomiting and fever. What is the diagnosis? A. Perforated duodenal ulcer B. Pancreatic laceration and hemoperitoneum C. Hemorrhagic pancreatitis D. Acute pancreatitis with necrosis RATIONALES: A. Incorrect. The CT images demonstrate fluid surrounding the pancreas in the retroperitoneum. There is intraperitoneal fluid as well, but there is no free intraperitoneal air to suggest a perforated duodenal ulcer. B. Incorrect. While peripancreatic and intrapancreatic fluid may be seen in patients with pancreatic trauma and laceration, history is not compatible. C. Incorrect. The patient does have hemorrhagic pancreatitis, but the salient feature is the nonenhancing glandular parenchyma that indicates the presence of pancreatic necrosis. Intravenous contrast enhanced CT is essential in the evaluation of patients with severe acute pancreatitis, because it is used to evaluate local pancreatic morphology, most importantly to identify and quantify pancreatic glandular necrosis. D. Correct. The CT images demonstrate a large amount of retroperitoneal and intraperitoneal fluid along with focal, geographic areas of pancreatic necrosis, indicating that this patient has severe acute pancreatitis. References: Balthazar EJ. Acute pancreatitis: assessment of severity with clinical and CT evaluation. Radiology 2002;223:603-613
- 5. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 28. You are shown CT images of the liver (Figures 5A and 5B) in a 76 year-old man. What is the MOST LIKELY diagnosis? A. Pneumobilia B. Portal vein thrombosis C. Biliary obstruction D. Portal venous gas RATIONALES: A. Incorrect. The CT demonstrates branching structures filled with gas ramifying throughout the liver. The extensive involvement extending to the subcapsular liver is, however, unusual for pneumobilia. The second, more inferior image, shows the portal vein bifurcation to be filled with gas, establishing the diagnosis of portal vein gas. B. Incorrect. The portal vein and its branches are abnormally hypodense. The extreme intraluminal low density is consistent with gas, not thrombus. The extensive involvement, to include very peripheral small branches, is more likely to be from gas than clot. Portal vein thrombus is macroscopically more limited in distribution, and usually involves more central branches near the hepatic hilum. C. Incorrect. Biliary obstruction can cause widespread, bilobar dilation of intrahepatic bile ducts. Although small biliary radicles can be distended with bile, these are usually inconspicuous compared to small peripheral portal venules filled with gas, which is extremely hypoattenuating. Morphologic evaluation of the dilated structures from the hilum into the hepatic parenchyma can help to differentiate abnormal bile ducts from portal venules. D. Correct. This CT scan demonstrates extensive portal venous gas. The dilated structures are filled with gas, not bile, which would be of fluid density. The portal vein bifurcation is outlined with gas. This helps to confirm that the gas is in the portal vein rather than the biliary tree. The subcapsular distribution is typical of portal vein gas, as opposed to biliary dilation, which tends to have a less peripheral distribution. The portal vein gas was found at surgery to be from ischemia of the entire small and large bowel. This was thought to be secondary to hypotension and sepsis associated with the patient’s multisystem organ failure. References: Paran H, Epstein T, Gutman M, et al. Mesenteric and portal vein gas: computerized tomography and clinical significance. Dig Surg 2003;20:127-32
- 6. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 29. You are shown an image from a small bowel series (Figure 6) on a 35-year- old man with abdominal pain and diarrhea. What is the MOST LIKELY diagnosis? A. Lymphoma B. Carcinoid C. Graft versus host disease D. Sprue RATIONALES: A. Incorrect. Lymphoma while producing a diffuse abnormality in the small bowel, it most commonly dilates and ulcerates (aneurismal dilatation) the intestine. B. Incorrect. Carcinoid usually produces asymmetric fold thickening and a tethered appearance due to metastatic disease in the small bowel mesentery. C. Correct. This is a classic appearance of graft versus host disease, a ribbon bowel. D. Incorrect. While sprue can produce changes in the small bowel with total absence of mucosal folds, the moulage sign, sprue usually produces dilatation of the bowel and the findings are usually more common in the jejunum not the ileum. References: Herlinger H, Jones B, Jacobs JE. Miscellaneous Abnormalities of the Small Bowel. In: Gore RM, Levine MS, eds. Textbook of Gastrointestinal Radiology, Philadelphia: W.B. Saunders 2000;865-883
- 7. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 30. During fluoroscopy in a 90 degree LAO projection, which operator location has the highest scatter radiation exposure levels? A. Next to the patient, adjacent to the image receptor B. Behind the image receptor C. Behind the x-ray tube D. Next to the patient, adjacent to the x-ray tube RATIONALES A. Incorrect. The primary source of radiation is scatter from the entrance surface of the exposed patient volume which is attenuated by patient tissue at this location B. Incorrect. The image receptor attenuates nearly all primary radiation incident on it C. Incorrect. Leakage radiation from the x-ray tube is minor compared to scatter radiation from the patient D. Correct. Scatter radiation emanating from the entrance surface of the exposed patient volume results in the highest stray radiation location here References: Balter S. Interventional Fluoroscopy: Physics, Technology and Safety, p.189
- 8. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 31. What is the most common primary appendiceal neoplasm detected on imaging studies? A. Carcinoid B. Lymphoma C. Ganglioneuroma D. Epithelial tumors RATIONALES: (This Test Items Was Partially Scored) A. Carcinoid tumors are the most common tumors detected on surgical pathology series. B. Lymphomatous involment of the appendix is rare, although the gastrointestinal tract is the most common site for extranodal non-Hodgkin’s lymphoma. C. Ganglioneuroma and other neuroendocrine tumors are rare. D. Although less common than carcinoid tumors of the appendix, these tumors are more likely to be diagnosed at imaging because of their large size and higher rate of complications. References: Pickhardt PF, Levy AD, Rohrman CA, et al. Primary neoplams of the appendix: Radiologic spectrum of disease with pathologic correlation. Radiographics, 2003; 23:645-662.
- 9. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 32. What is the “transient hepatic attenuation difference” during the arterial phase in patients with right portal venous thrombosis? A Increased enhancement of the left hepatic lobe B. Increased enhancement of the right hepatic lobe C. Decreased enhancement of the left hepatic lobe D. Decreased enhancement of the right hepatic lobe RATIONALES B. Correct. This transient increased enhancement is secondary to multiple factors. There is increased hepatic arterial flow to segments or lobes with decreased portal venous flow. In addition, the only blood flowing to this segment in the late arterial phase is from the hepatic artery and is therefore all enhanced arterial blood, while the normal segments, are still receiving 80% or their blood supply form the unopacified portal venous blood. References: Computed Body Tomography with MRI Correlation, Lee JKT, Sagel SS, Stanley RJ, Heiken JP, eds. Philadelphia, PA: Lippincott-Raven, 1998; 705-714. 33. Concerning hepatic metastatic tumors, which one is typically hypovascular? A. Melanoma B. Adenocarcinoma C. Renal cell carcinoma D. Sarcoma Answer: B RATIONALES: B. Correct. Colorectal adenocarcinomas have lower attenuation compared with normal liver and are most conspicuous on hepatic venous phase imaging. Melanoma, sarcoma, and renal cell carcinoma metastasis to the liver are characteristically hypervascular and are best visualized on late arterial phase images. References: Liver and Biliary System: Evaluation by Multidetector CT, IR Kamel, Liapi E, Fishman EK. Radiol Clin North Am 2005 Nov;43(6) 977-997.
- 10. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 34. Regarding achalasia, which of the following is CORRECT? A. It may be characterized by high-amplitude, simultaneous, and repetitive contractions of the esophagus B. Ganglionic cells are decreased in number, with a characteristic narrow aganglionic segment present C. It is more common in men than in women D. A diverticular defect may be seen following pneumatic dilatation RATIONALES: A. Correct. Achalasia is usually characterized by absence of primary peristalsis, elevated or normal resting LES pressures, and incomplete or absent LES relaxation. However, vigorous achalasia a variant presentation of primary achalasia presents with high-amplitude, simultaneous, and repetitive contractions of the esophagus. B. Incorrect. While it is true that ganglionic cells are decreased in number in achalasia, compatible with a neurogenic disorder, a narrow aganglionic segment is characteristic of Hirshsprung’s disease and NOT of achalasia. C. Incorrect. It occurs equally among males and females. Carcinoma arising in achalasia is more common in men than in woman. D. Incorrect. A diverticular defect may be seen following Heller myotomy. References: Ott DJ. Motility Disorders (of the Esophagus). In: Gore RM, et al., eds. Textbook of Gastrointestinal Radiology Vol. 1. Philadelphia, PA: W.B. Saunders Co, 1994; 349-352. Brucher BL, Stein HJ, Bartels H, et al. Achalasia and esophageal cancer : incidence, prevalence, and prognosis. World J Surg 2001; 25(6):745-749.
- 11. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 35. Regarding internal hernias, which of the following is TRUE? A. They can often be managed with NG tube decompression. B. Transmesenteric hernias in children are usually due to trauma. C. Pericecal hernias account for 13% of internal hernias. D. Broad ligament hernias usually involve the sigmoid colon. RATIONALES: A. Incorrect. These are closed-loop obstructions that require surgical repair. They most commonly present as a strangulated small bowel obstruction. B. Incorrect. Transmesenteric hernias in children are usually due to a congenital mesenteric defect. C. Correct. D. Incorrect. Broad ligament hernias usually involve the small bowel. References: Takeyama N, Gokan T, Ohgiya Y, et al. CT of internal hernias. RadioGraphics 2005; 25:997-1015
- 12. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 36. Concerning acute pancreatitis, which of the following is TRUE? A. The degree of pancreatic necrosis is best prognostic indicator. B. Severe acute pancreatitis is found in approximately 50% of patients. C. It is commonly caused by hypertriglyceridemia in the United States. D. The initial diagnostic test should be abdominal ultrasonography. RATIONALES: A. Correct. The degree of pancreatic necrosis corresponds to the severity of the patient’s acute pancreatitis episode. Early assessment is critical for predicting which patients are likely to suffer lethal attacks, which occur in 2-10% of cases. The increased frequency of death in acute pancreatitis is directly correlated with the development and extent of pancreatic necrosis. B. Incorrect. Of all patients who present with acute pancreatitis, 70-80% have mild episodes and 20-30% have severe attacks. C. Incorrect. Acute pancreatitis in the U.S. is most commonly associated with choledocholithiasis and ethanol abuse, with other etiologic factors such as metabolic disorders (hypercalcemia and hyperlipidemia), trauma, including ERCP-induced pancreatitis, medications (azathioprine, sulfonamides), and structural abnormalities such as pancreas divisum and tumors being much less common. D. Incorrect. Abdominal ultrasound should not be the first diagnostic test ordered for patients presenting to the emergency department with acute pancreatitis. Dynamic contrast enhanced CT (creatinine permitting) is the diagnostic test of choice because it allows characterization of the inflammation and calculation of the degree of pancreatic glandular necrosis (see A above). References: Balthazar EJ. Acute pancreatitis: assessment of severity with clinical and CT evaluation. Radiology 2002;223:603-613. Mortele KJ, Weisner W, Intriere L, et al. A modified CT Severity Index for evaluating acute pancreatitis: improved correlation with patient outcome. AJR 2004;183:1261-1265.
- 13. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 37. In digital radiography, the kV and mAs are selected to provide optimal ________ at the lowest possible dose to the patient. A. signal to noise ratio B. optical density C. spatial resolution D. Image contrast RATIONALES: A. Correct: Unlike screen-film detectors that have a fixed film contrast and typically require low kV to ensure adequate subject contrast that is mapped to radiographic contrast by the film characteristic curve, digital detectors have extremely wide exposure latitude (also known as dynamic range). This permits flexibility in determining the best combination of kV and mAs to achieve proper signal to noise ratio that subsequently can be adjusted (contrast and spatial resolution enhancement) with image processing algorithms. B. Incorrect: Optical density is a feature of the screen-film detector, and is the log of the opacity of the film. C. Incorrect: In most instances where there is sufficient exposure and within the range of typical diagnostic techniques, the kV and mAs do not affect the spatial resolution characteristics of the image. Spatial resolution is chiefly determined by the detector element area (dimensions) and by the sampling pitch (distance between detector elements D. Incorrect: Image contrast with a digital system is freely adjustable as long as there is sufficient signal to noise ratio of the statistical information in the image. That is why the digital detectors are often referred to as “SNR limited” while screen-film detectors are referred to as “contrast limited.” References: Bushberg JT, Seibert JA, Leidholdt EM, Boone JM. The Essential Physics of Medical Imaging, 2nd Edition, Chapter 11, p. 308.
- 14. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 38. Concerning CT findings in the pancreas following blunt abdominal trauma, which of the following is TRUE? A. Injury typically involves the pancreatic head region. B. Contusion appears as low attenuation fluid separating enhancing pancreatic parenchyma. C. Presence of fluid surrounding the pancreas is highly specific of glandular injury. D. Focal glandular enlargement indicates injury. RATIONALES: A. Incorrect. Injury to the pancreas after blunt abdominal trauma typically involves the midline or the neck portion of the pancreas. B. Incorrect. Low attenuation fluid separating two portions of the enhancing pancreatic parenchyma is consistent with laceration, not contusion. C. Incorrect. The presence of fluid surrounding the pancreas is not specific for glandular injury. Fluid surrounding the pancreas may be due to injury (post traumatic pancreatitis or acute hemorrhage) but can also be seen in patients with aggressive fluid resuscitation. D. Correct. Subtle changes of pancreatic injury include focal pancreatic enlargement. References: Novelline R, Rhea JT, Bell T. Helical CT of abdominal trauma. Radiol Clin North Am 1999;37:591-612
- 15. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 39. Concerning primary biliary cirrhosis, which of the following is TRUE? A. Predominately affects the extrahepatic bile ducts B. Associated with antimitochondrial antibodies C. More common in males than females D. Rapidly progresses to liver failure RATIONALES: A. Incorrect. Primary biliary cirrhosis (PBC) does not affect the extrahepatic bile ducts. PBC is characterized by the necroinflammatory destruction of medium to small intrahepatic bile ducts. Periportal fibrosis and cirrhosis can ensue. B. Correct. PBC is highly associated with antimitochondrial antibodies (AMA). These autoantibodies are found in 95% of PBC patients. C. Incorrect. PBC affects females rather than males in 90% of cases. D. Incorrect. The natural history of PBC is one of slow progression. At least 25% of patients are initially asymptomatic. End-stage liver disease (ESLD) occurs over the course of 10-15 years. References: Chung RT, Podolsky D: Cirrhosis and its complications. In: Braunwald E, Fauci AS, Kasper DL, et al, eds. Harrison’s principles of internal medicine. 15th ed. New York, NY:McGraw-Hill, 2001;1754-1767. Lindor KD: Primary biliary cirrhosis: clinical spectrum and mechanisms of disease. In: Bacon BR, Goodman ZD, Brunt EM, course directors. Liver disease in the 21st century: clinico-pathologic correlates. AASLD postgraduate course syllabus, 2003; 168-171.
- 16. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 40. Concerning amebiasis, which of the following is TRUE? A. It is caused by the protozoan Entamoeba dispar. B. It is the most common parasitic cause of death worldwide. C. It most commonly affects the right colon. D. Extraintestinal complications of amebiasis are uncommon. RATIONALES: A. Incorrect. Although 10% of the world’s population is infected by Entamoeba, most are infected by the noninvasive species E. dispar, which results in an asymptomatic carrier state or self-limited infection. Amebiasis is caused by the invasive species Entamoeba histolytica. B. Incorrect. Amebiasis is the third most deadly parasitic infection worldwide, after schistosomiasis and malaria. C. Correct. Amebiasis most frequently involves the cecum and ascending colon. The rectum and sigmoid can be involved. The terminal ileum is spared. D. Incorrect. Extraintestinal infection by E. histolytica is not uncommon and often involves the liver. The genitourinary tract can be involved by direct extension or by hematogenous spread. Amebiasis can cause genital ulcers and fallopian tube infection. Cerebral involvement occurs in 0.1% of patients, and can be rapidly fatal. References: Reed S: Amebiasis and infection with free-living amebas. In: Braunwald E, Fauci AS, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine, 15th ed. New York, NY:McGraw-Hill, 2001;1199-1203. Rubesin SE, Bartram CI, Laufer I: Inflammatory bowel disease. In: Levine MS, Rubesin SE, Laufer I, eds. Double contrast gastrointestinal radiology, 3rd ed. Philadelphia, PA:W.B. Saunders, 2000;417-470. Horga MA, Naparst TR, Dhawan VK: Amebiasis. In: eMedicine. March 30, 2006.(http://www.emedicine.com/ped/topic80.htm)
- 17. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 41. Concerning nonalcoholic steatohepatitis, which one of the following is CORRECT? A. Noninvasive imaging can distinguish between nonalcoholic steatohepatitis and nonprogressive nonalcoholic fatty liver disease. B. Noninvasive imaging can detect mild (< 30%) fatty infiltration of the liver. C. Histopathology reveals necroinflammatory changes and eventually fibrosis of the liver. D. It does not result in cirrhosis. RATIONALES: A. Incorrect. Noninvasive imaging can detect moderate to severe fatty liver disease. However, it can not distinguish between nonprogressive, noninflammatory nonalcoholic fatty liver disease, and progressive, inflammatory nonalcoholic steatohepatitis. B. Incorrect. Noninvasive imaging can not detect fatty infiltration that is < 30% of hepatic mass. C. Correct. By definition, NASH is a necroinflammatory condition of the liver with hepatocyte injury and lobular inflammation. These histopathologic changes are associated with the eventual development of hepatic fibrosis. D. Incorrect. Hepatic fibrosis in NASH can evolve into cirrhosis. Like all cirrhotic livers, NASH- related cirrhosis is associated with an increased risk of hepatocellular carcinoma, which is estimated to occur in about 7% of cases. References: Brunt EM: Primary biliary cirrhosis: clinical spectrum and mechanisms of disease. In: Bacon BR, Goodman ZD, Brunt EM, course directors. Liver disease in the 21st century: clinico-pathologic correlates. AASLD postgraduate course syllabus, 2003;65-74. Park SH, Kim PN, Kim KW, et al: Macrovesicular hepatic steatosis in living liver donors: use of CT for quantitative and qualitative assessment. Radiology 2006;239:105-112. Saadeh S, Younossi ZM, Remer EM, et al: The utility of radiological imaging in nonalcoholic fatty liver disease. Gastroenterology 2002 123:745-750. Shimada M, Hashimoto E, Taniai M, et al: Hepatocellular carcinoma in patients with non-alcoholic steatohepatitis. J Hepatol 2002 37:154-160.
- 18. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 42. Concerning pseudomembranous colitis, which one of the following is TRUE? A. Clostridium difficile is the most common cause of antibiotic-related diarrhea. B. Pseudomembranous colitis caused by C. difficile does not typically occur with administration of cephalosporins and penicillins. C. Pseudomembranous colitis usually spares the sigmoid colon. D. Pseudomembranous colitis is mediated by the release of C. difficile toxins. RATIONALES: A. Incorrect. Antibiotic-related diarrhea is common, but only 10-20% of antibiotic-related diarrhea is caused by C. difficile. B. Incorrect. Pseudomembranous colitis caused by C. difficile can occur with any antibiotic, especially clindamycin, cephalosporins and penicillins. C. Incorrect. Pseudomembranous colitis is most often a pancolitis, but can be a segmental colitis. The sigmoid colon is spared in about 10% of cases. D. Correct. Pseudomembranous colitis caused by C. difficile is toxin-mediated. The production of both an enterotoxin (Toxin A) and a cytotoxin (Toxin B) is required to cause pseudomembranous colitis. References: Watanabe JM, Surawicz CM: Colitis: pseudomembranous, microscopic, and radiation. In: McNally PR, ed. GI/liver Secrets, 3rd ed. Philadelphia, PA:Elsevier Mosby, 2006;435-442. Kawamoto S, Horton KM, Fishman EK: Pseudomembranous colitis: spectrum of imaging findings with clinical and pathologic correlation. Radiographics 1999;19:887-897.
- 19. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 43. Concerning angiosarcoma of the spleen, which one of the following is TRUE? A. The spleen is not typically enlarged. B. Malignant fibrous histiocytoma is more common than angiosarcoma. C. Spontaneous rupture occurs in approximately 10% of patients. D. Prognosis is very poor with only 20% survival rate at 6 months. RATIONALES: A. Incorrect. The spleen is usually enlarged. B. Incorrect. Angiosarcoma is the most common non-lymphoid primary malignant of the spleen. C. Incorrect. Spontaneous rupture occurs in 30%, not 10%. D. Correct. The prognosis is very poor. References: Mortele KJ, Mergo PJ, Kunnen M, Ros PR. Tumoral Pathology of the Spleen. In: Baert AL, Heuck FHW, Youker JE, eds. Medical Imaging of the Spleen. Berlin: Springer 2000;101-122.
- 20. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 44. Which of the following statements about duodenal adenocarcinoma is TRUE? A. The jejunum is a more common site for primary adenocarcinoma than the duodenum. B. The classic appearance on upper gastrointestinal examination is an apple core lesion. C. There is an increased risk of adenocarcinoma in patients with a duodenal web. D. Duodenal carcinoid is more common than duodenal adenocarcinoma. RATIONALES: A. Incorrect. The duodenum is a more common site than the jejunum. B. Correct. A short annular constricting ulcerative (apple core) lesion is the classic radiographic appearance. C. Incorrect. D. Incorrect. Duodenal carcinoid is rare. References: Gourtsoyiannis NC. Primary Malignant Neoplasms. In: Imaging of Small Intestinal Tumours. Gourtsoyiannis NC, Nolan DJ, eds. Amsterdam: Elsevier, 1997;105- 189 45. Which one of the following usually involves the proximal small bowel? A. Lymphoma B. Sprue C. Giardiasis D. Yersenia RATIONALES: A. Incorrect. Lymphoma most commonly involves the ileum. B. Incorrect. Sprue involves the entire small bowel. C. Correct. Giardiasis commonly involves the proximal small bowel. D. Incorrect. Yersenia usually involves just the terminal ileum. References: Herlinger H, Ekberg OT. Other Inflammatory Conditions of the Small Bowel. In: Gore RM, Levine MS, eds. Gastrointestinal Radiology, (2nd ed). Philadelphia: W.B. Saunders 2000; 746-758
- 21. 2007 ACR Diagnostic Radiology In-Training Exam Rationales 46. Concerning Peutz-Jeghers Syndrome, which one of the following is TRUE? A. It is an autosomal-recessive inherited trait. B. It is associated with a high risk for the development of adenocarcinoma of the pancreas. C. It represents 50% of hereditary gastrointestinal polyposis syndromes. D. Approximately 80% of patients have gastric polyps. RATIONALES: A. Incorrect. Peutz-Jeghers is inherited as an autosomal dominate trait. B. Correct. There is an increased risk of a number of malignancies. C. Incorrect. It represents about 10% of the hereditary polyposis syndromes. D. Incorrect. Approximated 30% of patients have gastric polyps. References: Gourtsoyiannis NC, Nolan DJ. Polyposis Syndromes. In: Gourtsoyiannis NC, Nolan DJ, eds. Imaging of Small Intestinal Tumours. Amsterdam: Elsevier 1997;213-229.