9630942363 Genuine Call Girls In Ahmedabad Gujarat Call Girls Service
23205011
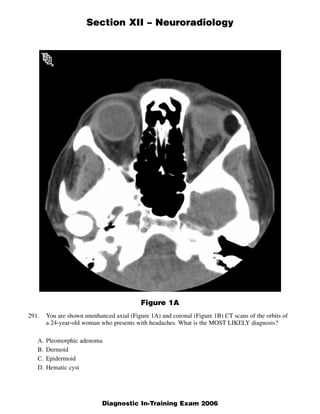
1. Section XII – Neuroradiology
Figure 1A
291. You are shown unenhanced axial (Figure 1A) and coronal (Figure 1B) CT scans of the orbits of
a 24-year-old woman who presents with headaches. What is the MOST LIKELY diagnosis?
A. Pleomorphic adenoma
B. Dermoid
C. Epidermoid
D. Hematic cyst
1
Diagnostic In-Training Exam 2006
2. Section XII – Neuroradiology
Figure 1B
2 American College of Radiology
3. Section XII – Neuroradiology
Question #291
Rationales:
A. Incorrect. Pleomorphic adenoma is the most common benign tumor of the lacrimal gland. There
may be cystic areas within the mass and lesions of long standing may remodel adjacent bone. Mild
enhancement is often present. However, fatty degeneration within this neoplasm would be exceed-
ingly unlikely.
B. Correct. Dermoids are the most common benign congenital orbital mass. Arising from epithelial
rests, most often at the frontozygomatic suture, they usually present in the first decade of life. CT
demonstrates a fat density extraconal mass which may have peripheral calcification and may remod-
el adjacent bone. MR demonstrates fat signal intensity and the lesion may also contain a fat fluid
level.
C. Incorrect. Similar to dermoids, epidermoids are congenital epithelial inclusion cysts in the extra-
conal space. However, epidermoids contain no fat. They are composed of squamous debris and cho-
lesterol. For that reason, epidermoids are of fluid density on CT and are approximately isointense to
CSF on T1 and T2 weighted MR images.
D. Incorrect. A hematic cyst is an incompletely resorbed hematoma which may remain clinically silent
for long periods of time. Patients usually present with diplopia and painless unilateral proptosis.
There may be history of prior orbital trauma or surgery. The cyst contains hematogenous debris sur-
rounded by a fibrous pseudocapsule. On imaging, the cyst is usually a well defined nonenhancing
extraconal mass. They are often hyperdense on CT secondary to their elevated protein content and
usually hyperintense on both T1 and T2 weighted MR sequences.
3
Diagnostic In-Training Exam 2006
4. Section XII – Neuroradiology
Figure 2A
Figure 2B
4 American College of Radiology
5. Section XII – Neuroradiology
Figure 2C
292. You are shown a FLAIR sagittal MR image of the brain (Figure 2A) and a sagittal T2-weighted
MR image of the cervical spine (Figure 2B) in a 35-year-old woman with extremity weakness. A
sagittal T2-weighted MR image of the cervical spine was obtained 3 years later (Figure 2C).
What is the MOST LIKELY diagnosis?
A. Lyme Disease
B. Multiple sclerosis
C. Infarction
D. Sarcoidosis
5
Diagnostic In-Training Exam 2006
6. Section XII – Neuroradiology
Question #292
Rationales:
A. Incorrect. While white matter changes can occur in the brain and spinal cord, the degree of involve-
ment seen in this case does not favor Lyme’s Disease.
B. Correct. The multiple “plaques” in the original cervical spine and brain images, particularly with
involvement of the corpus callosum, and the post ms atrophy is typical of this disorder.
C. Incorrect. The patient’s age, and the pattern make this diagnosis unlikely.
D. Incorrect. The severity of spinal cord involvement is atypical for sarcoid. Sarcoidosis usually pres-
ents with more extensive pachymeningeal disease.
6 American College of Radiology
7. Section XII – Neuroradiology
Figure 3A
Figure 3B
7 American College of Radiology
8. Section XII – Neuroradiology
Figure 3C
293. A 62-year-old man presents with chronic back pain. You are shown sagittal T1-weighted and T2-
weighted MR images (Figures 3A and 3B) and a transaxial proton density-weighted MR image
(Figure 3C). What is the MOST LIKELY diagnosis?
A. Synovial Cyst
B. Schwannoma
C. Abscess
D. Chondroblastoma
8
Diagnostic In-Training Exam 2006
9. Section XII – Neuroradiology
Question #293
Rationales:
A. Correct. The posterior lateral location, broad-based position on the facet joint, and classic T-1 and
T-2 weighted signal changes are diagnostic of a synovial cyst.
B. Incorrect. Schwannomas may be eccentric within the spinal canal but are usually more cephalad in
location. Ring enhancement is not uncommonly seen.
C. Incorrect. No contrast enhancement or specific clinical information suggests this diagnosis.
D. Incorrect. These tumors involve the osseous posterior elements of the spine.
9 American College of Radiology
10. Section XII – Neuroradiology
Figure 4A
Figure 4B
10 American College of Radiology
11. Section XII – Neuroradiology
Figure 4C
Figure 4D
294. An 85-year-old man presents with progressive inability to walk. You are shown sagittal T2-
weighted (Figure 4A), axial T2-weighted (Figure 4B), sagittal T1-weighted post-contrast (Figure
4C) MR images, and a source image for spinal MRA (Figure 4D). What is the MOST LIKELY
diagnosis?
A. Transverse myelitis
B. Dural arteriovenous fistula
C. Anterior spinal artery occlusion
D. Leptomeningeal carcinomatosis
11
Diagnostic In-Training Exam 2006
12. Section XII – Neuroradiology
Question #294
Rationales:
A. Incorrect. Transverse myelitis is an inflammatory condition of the spinal cord associated with rapid-
ly progressive neurologic dysfunction. The disease is associated with many conditions including
ADEM, MS, connective tissue disease, sarcoid, to name a few. Though the T2 appearance may be
consistent with transverse myelitis in this case, the dilated surface vessels evident on T2, T1 post
imaging and the spinal MRA are inconsistent with this diagnosis.
B. Correct. The combination of a spinal dural arteriovenous fistula in combination with myelopathy is
given the eponym Foix Alajouanine Syndrome. The lesions are generally supplied by a radicu-
lomeningeal artery with abnormal venous drainage to the perimedullary venous plexus. The lesions
become symptomatic due to shunting of blood leading to venous hypertension and chronic passive
venous congestion of the spinal cord.
C. Incorrect. Spinal cord infarction usually presents with acute onset of loss of bowel and bladder
function as well as moderate impairment of lower extremity motor and sensory function. Location is
usually in the conus with an enlarged conus associated with increased T2 signal. Occasionally
abnormal increased T2 signal in the neighboring vertebral body can be seen. Spinal MRA has not
been able to reliably demonstrate the anterior spinal artery secondary to its small size.
D. Incorrect. Metastatic disease in the subarachnoid space is seen as either discrete nodules on the sur-
face of the cord and cauda equine or as thick, frosting-like enhancement coating the cord.
Metastatic disease would not show flow signal on the MRA images. Lumbar puncture is the best
diagnostic procedure to confirm meningeal carcinomatosis.
12 American College of Radiology
13. Section XII – Neuroradiology
Figure 5A
Figure 5B
13 American College of Radiology
14. Section XII – Neuroradiology
Figure 5C
295. A 35-year-old woman presents with cranial nerve palsies on the left. You are shown axial
T2-weighted (Figure 5A), T1-weighted post-contrast (Figure 5B) and diffusion-weighted
(Figure 5C) MR sequences. What is the MOST LIKELY diagnosis?
A. Arachnoid cyst
B. Meningioma
C. Epidermoid
D. Schwannoma
14
Diagnostic In-Training Exam 2006
15. Section XII – Neuroradiology
Question #295
Rationales:
A. Incorrect. Though the fluid like signal identified on T1 and T2 as well as the lack of contrast
enhancement are all consistent with arachnoid cyst, the presence of marked hyperintensity in the
lesion on DWI separates epidermoid from archnoid cyst in this case. Arachnoid cysts are
hypointense on DWI secondary to free diffusion in the lesion.
B. Incorrect. Though a commonly found mass in this location, the signal characteristics and enhance-
ment characteristics argue against meningioma. Meningiomas are typically soft tissue signal on T1
and T2 and enhance homogeneously.
C. Correct. Epidermoid cysts are frequently found in this location. They follow fluid on all MR
sequences but the distinguishing feature is the bright signal on DWI as opposed to the arachnoid
cyst which is hypointense on DWI as a result of free diffusion.
D. Incorrect. Though again a commonly encountered lesion in this region, the lack of contrast
enhancement argues against schwannoma as the diagnosis as these lesions avidly enhance with con-
trast.
15 American College of Radiology
16. Section XII – Neuroradiology
Figure 6A
Figure 6B
16 American College of Radiology
17. Section XII – Neuroradiology
Figure 6C
296. You are shown an axial unenhanced CT image (Figure 6A) and sagittal unenhanced T1-weighted
(Figure 6B) and axial gadolinium-enhanced T1-weighted (Figure 6C) MR images of the brain on
a 50-year-old man with headaches. What is the MOST LIKELY diagnosis?
A. Craniopharyngioma
B. Giant internal carotid artery aneurysm
C. Rathke’s cleft cyst
D. Oligodendroglioma
17
Diagnostic In-Training Exam 2006
18. Section XII – Neuroradiology
Question #296
Rationales:
A. Correct. Craniopharyngioma is often intrasellar and suprasellar in location, as in this case. 90% of
craniopharyngiomas show cyst formation, calcification, and peripheral enhancement, as in this case.
B. Incorrect. Aneurysms may have peripheral calcification, but they do not have cystic components.
Enhancement is uniform , with peripheral blood products usually seen in giant aneurysms.
C. Incorrect. Rathke cleft cysts do not enhance. It would also be extremely rare for a Rathke cleft cyst
to enlarge enough produce hydrocephalus.
D. Incorrect. This is an extra-axial mass. Oligodendroglioma may have cystic components and calcifi-
cation, but it is a primary intra-axial tumor.
18 American College of Radiology
19. Section XII – Neuroradiology
297. An MRI fast-spin-echo (FSE) pulse sequence decreases the overall acquisition time compared to
a standard-spin-echo (SE) pulse sequence by using which one of the following?
A. Very short TR
B. Very short TE
C. Multiple frequency encode gradient variations per TE
D. Multiple phase encode gradient variations per TR
Question #297
Rationales:
A. Incorrect. The TR for FSE determines the image contrast weighting as it does in standard spin echo.
B. Incorrect. The TE for FSE determines the image contrast weighting as it does in standard spin echo.
C. Incorrect. Only one frequency encode gradient is applied for each TE period (although there are
multiple TE’s per TR interval in an FSE sequence).
D. Correct. Phase encode gradients determine the location of k-space data; for FSE imaging, this is
performed by changing the gradients and creating subsequent echoes to fill k-space faster per TR
interval.
19 American College of Radiology
20. Section XII – Neuroradiology
Which one of the following is the MOST common cause of cerebral spinal fluid otorrhea?
298.
A. Temporal bone fracture
B. Mondini dysplasia
C. Hyrtl’s canal fistula
D. Glomus tympanicum tumor
Question #298
Rationales:
A. Correct. Of the causes listed here, temporal bone fracture is the most common cause of CSF otor-
rhea. Patients usually have a history of severe head trauma, and they will have hemotympanum or
CSF otorrhea at presentation. As will all cases of CSF leak, these patients are at risk for meningitis.
CSF otorrhea in cases of trauma will frequently show spontaneous resolution.
B. Incorrect. Mondini dysplasia is the most common congenital cause for CSF otorrhea. In these cases,
CSF can leak through the internal auditory canal through a deformed osseous labyrinth with an asso-
ciated stapes deformity. Congenital CSF otorrhea is less common than temporal bone trauma.
C. Incorrect. A congenital fistula in Hyrtl’s canal (the tympanomeningeal fissure) is an extremely rare
cause of congenital CSF otorrhea. This represents an embryonic connection between the round win-
dow niche and the posterior fossa. Hyrtl’s canal is usually obliterated around 25 weeks gestation.
Very few cases of patent Hyrtl’s canal are reported in the literature.
D. Incorrect. Glomus tympanicum is a tumor of neural crest origin which originates on the cochlear
promontory. If it becomes large, the tumor can erode into the ossesous labyrinth and result in CSF
leakage. The middle ear is the least common location for glomus tumors, with the carotid bifurcation
and jugular foramen being more common. Again, temporal bone trauma is seen more frequently.
20
Diagnostic In-Training Exam 2006
21. Section XII – Neuroradiology
Which one of the following is the MOST common intra-axial posterior fossa neoplasm in
299.
adults?
A. Glioblastoma multiforme
B. Hemangioblastoma
C. Meningioma
D. Metastasis
Question #299
Rationales:
A. Incorrect. Glioblastoma multiforme is the most common primary supratentorial neoplasm in adults.
However, it is uncommon in the posterior fossa. Brainstem glioma, which is usually a lower-grade
astrocytoma, is the most common glial neoplasm found in the posterior fossa in adults.
B. Incorrect. Hemangioblastoma is one of the more common primary cerebellar neoplasms of adults. It
is associated with von Hippel-Lindau syndrome. Metastases are much more common overall.
C. Incorrect. Meningioma is the most common benign primary extra-axial neoplasm of the brain. The
location of meningiomas follows the anatomy of the meninges, with the cerebral convexity being
the most common location. This question is about intra-axial neoplasm.
D. Correct. Metastasis is the most common intra-axial posterior fossa neoplasm in adults. Lung and
breast carcinoma are the most common primary tumors.
21 American College of Radiology
22. Section XII – Neuroradiology
300. A patient with a history of atrial fibrillation presents with 1 hour of right-sided hemiparesis.
Which examination is MOST sensitive for acute cerebral infarction in this case?
A Non-contrast computed tomography
B. T2-weighted MRI
C. Diffusion-weighted MRI
D. Unenhanced T1-weighted MRI
Question #300
Rationales:
A. Incorrect. Non-contrast computed tomography is very sensitive to acute cerebral hemorrhage.
However, changes of ischemic infarction usually are not seen for one or two days.
B. Incorrect. Edema associated with cerebral infarction will be seen on T2-weighted images after one
to two days.
C. Correct. DWI shows abnormal signal within one hour of infarction in the majority of cases.
Diffusion weighted MRI is abnormal in over 90% of acute infarctions in adults within 6 hours.
These features make DWI the imaging modality of choice for detection of acute infarction.
D. Incorrect. Cortical necrosis is visible on unenhanced T1-weighted images after 5-7 days in some
cases. T1-weighted images are usually normal in the first 1-2 days after acute infarction, although
edema with sucal effacement may be seen in some cases.
22
Diagnostic In-Training Exam 2006
23. Section XII – Neuroradiology
Concerning hamartomas of the tuber cinereum, which one is TRUE?
301.
A. Intense uniform contrast enhancement
B. Associated with focal motor seizures
C. Cause precocious puberty
D. Hyperintense to gray matter on T1-weighted MR imaging
Question #301
Rationales:
A. Incorrect. Hamartomas of the tuber cinereum do not enhance as a rule. These lesions are immedi-
ately anterior to the mamillary bodies and may be broad based or pedunculated in configuration.
B. Incorrect. Hamartomas of the tuber cinereum produce gelastic seizures. This may result from con-
nections between the lesion and the limbic system.
C. Correct. Hamartomas of the tuber cinereum do in fact produce precocious puberty secondary to
secretion of luteinizing hormone-releasing hormone by the lesion.
D. Incorrect. Hamartomas of the tuber cinereum are typically isointense to gray matter on T1WI and
usually hyperintense to gray matter on T2WI.
23 American College of Radiology
24. Section XII – Neuroradiology
302. A CT scan is performed at 120 kV and 100 mAs. A region-of-interest measurement from the
CSF in the ventricles yields an average CT number of 10 with a standard deviation of 8.
The scan is repeated with 400 mAs. What is the expected CT number and standard deviation
of the CSF?
A. CT number of 10 with a standard deviation of 4
B. CT number of 10 with a standard deviation of 2
C. CT number of 40 with a standard deviation of 4
D. CT number of 40 with a standard deviation of 2
Question #302
Rationales:
A. Correct. Changing the mAs should have no effect on the measured CT number value. The fraction-
al standard deviation goes with one over the number of photons used to make the image. Hence,
quadrupling the mAs should halve the relative standard deviation.
B. Incorrect. See correct answer
C. Incorrect. See correct answer
D. Incorrect. See correct answer
24
Diagnostic In-Training Exam 2006
25. Section XII – Neuroradiology
Which one of the following is NOT located in the cavernous sinus?
303.
A. Oculomotor nerve
B. Third division of the trigeminal nerve
C. Internal carotid artery
D. Abducens nerve
Question #303
Rationales:
A. Incorrect. The oculomotor nerve courses within the lateral wall of the cavernous sinus and is the
most superiorly located of the cavernous sinus cranial nerves.
B. Correct. While both the first and second divisions of the trigeminal nerve are within the lateral wall
of the cavernous sinus, the third division exits the skull base via foramen ovale.
C. Incorrect. The internal carotid artery courses through the cavernous sinus medial to cranial nerves
III, IV, V1, V2, and VI.
D. Incorrect. The abducens nerve traverses the cavernous sinus and is the most medially located of the
cranial nerves of the cavernous sinus, lying immediately lateral to the internal carotid artery.
25 American College of Radiology
26. Section XII – Neuroradiology
304. Bilateral enhancing masses within the internal auditory canals are MOST consistent with which
one of the following?
A. Metastases
B. Neurofibromatosis type 1
C. Neurofibromatosis type 2
D. Multiple meningiomas
Question #304
Rationales:
A. Incorrect. While metastatic disease may involve the internal auditory canals, bilateral lesions in the
absence of other disease would be unlikely.
B. Incorrect. This entity is associated with optic glioma, plexiform neurofibroma, and peripheral neu-
rofibromas. However, lesions involving the seventh or eighth cranial nerves are not a feature of
NF1.
C. Correct. Bilateral enhancing masses within the internal auditory canals are virtually pathognomonic
for NF2. These lesions represent vestibular schwannomas. NF2 is also characterized by multiple
schwannomas in other locations as well as an increased incidence of meningiomas. An increased
incidence of ependymomas has also been reported.
D. Incorrect. While meningiomas may involve the internal auditory canal, their site of origin is usually
outside the canal with little, if any, soft tissue extending into the canal. Meningiomas may also have
a dural tail and usually make an obtuse angle with the adjacent petrous bone. Vestibular schwanno-
mas lack a dural tail and form an acute angle with the petrous bone.
26
Diagnostic In-Training Exam 2006
27. Section XII – Neuroradiology
305. Concerning the pituitary gland, which is TRUE?
A. Dynamic contrast-enhanced MRI is most useful for the diagnosis of macroadenomas.
B. There is a low (<5%) incidence of Rathke cleft cysts in autopsy series.
C. Enlargement of the pituitary stalk is seen in lymphocytic hypophysitis.
D. Pituitary apoplexy is characterized by a slowly progressive clinical syndrome.
Question #305
Rationales:
A. Incorrect. Dynamic CE MRI is useful for diagnosis of microadenomas.
B. Incorrect. The incidence is much higher, closer to 33%.
C. Correct.
D. Incorrect. Pituitary apoplexy is an acute clinical process.
27 American College of Radiology
28. Section XII – Neuroradiology
Concerning imaging of orbital infections, which one is TRUE?
306.
A. Contiguous spread from ethmoid sinus infection first presents as sub-periosteal phlegmon.
B. Erosion of the bony orbit is usually seen when adjacent infection spreads into the orbit.
C. The muscular cone separates the pre-septal from the post-septal space.
D. Infiltration of the retrobulbar fat is seen on CT as a mild decrease in attenuation.
Question #306
Rationales:
A. Correct. True statement.
B. Incorrect. Even with an intact bony margin, bacterial can enter the orbit through vascular foramina
for arteries and veins
C. Incorrect. The muscular cone defines the intra- and extra-conal spaces
D. Incorrect. There is a mild increase in the Hounsfield numbers
28
Diagnostic In-Training Exam 2006
29. Section XII – Neuroradiology
Concerning carcinoma of the nasopharynx, which one is TRUE?
307.
A. Nasopharyngeal carcinoma commonly spreads to level IV and V nodes in the neck.
B. Intracranial spread is usually through the hematogenous route.
C. Epstein-Barr virus infection is a risk factor.
D. Nasopharyngeal squamous cell carcinoma presents on MRI is typically not enhancing, with
hypo-intense signal on T2.
Question #307
Rationales:
A. Incorrect. Spread is to nodes more superiorly in the neck.
B. Incorrect. Intracranial involvement is typically from retrograde perineural spread through the skull
base foramina
C. Correct. Nasopharyngeal carcinoma is common in young adult men in Southeast Asia, and is
thought to be caused by EBV in this group.
D. Incorrect. Tumors mildly enhance and are hyper-intense on T2.
29 American College of Radiology
30. Section XII – Neuroradiology
Concerning the salivary apparatus associated with the oral cavity, which one is TRUE?
308.
A. Plunging ranulas are confined to the sublingual space.
B. Wharton’s duct drains the sublingual gland.
C. Stensen’s duct drains the parotid gland.
D. Calculi most commonly occur in the parotid gland or the duct associated with it.
Question #308
Rationales:
A. Incorrect. Plunging or diving ranulas extend from the sublingual into the submaxillary space as well.
B. Incorrect. It drains the submandibular gland.
C. Correct. True.
D. Incorrect. Calculi most commonly (80-90%) occur in the submandibular gland.
30
Diagnostic In-Training Exam 2006
31. Section XII – Neuroradiology
309. Anterior communicating artery aneurysms are characterized by which hemorrhagic pattern?
A. Diffuse subarachnoid hemorrhage in the basal cisterns
B. Diffuse cisternal subarachnoid hemorrhage with extension into the temporal lobe
C. Subarachnoid hemorrhage predominantly around the medulla with intraventricular hemorrhage
D. Interhemispheric subarachnoid hemorrhage and parenchymal frontal lobe hemorrhage
Question #309
Rationales:
A. Incorrect. This is more common with posterior communicating and basilar tip artery aneurysms.
B. Incorrect. This more common with posterior communicating or middle cerebral artery aneurysms.
C. Incorrect. This is more typical of PICA or vertebral aneurysms.
D. Correct. This is typical of anterior communicating artery aneurysmal rupture.
31 American College of Radiology
32. Section XII – Neuroradiology
310. Concerning olfactory neuroblastoma, what is the classic imaging and clinical presentation?
A. Involvement of the nasal cavity only in patients between the ages of 30 and 40
B. Cribriform plate, orbital, nasal involvement in patients older than 50
C. Maxillary sinus involvement in a child
D. Sphenoid and clivus involvement in the elderly
Question #310
Rationales:
A. Incorrect. This is the most common pattern for undifferentiated nasal carcinoma in Southeast Asia.
This tumor is associated with consumption of smoked and salted fish and Epstein-Barr virus
B. Correct. This is the classic pattern of olfactory neuroblastoma (esthesioneuroblastoma). The
intracranial component is often cystic.
C. Incorrect. Maxillary sinus neoplasms are rare in children. Inflammatory disease is much more com-
mon. The peak incidence of olfactory neuroblastoma
D. Incorrect. This is the classic imaging pattern of chordoma. Chordoma is seen across a broad age
range.
32
Diagnostic In-Training Exam 2006
33. Section XII – Neuroradiology
311. What is the MOST common primary orbital tumor in an adult?
A. Optic glioma
B. Optic nerve sheath meningioma
C. Cavernous hemangioma
D. Neurofibroma
Question #311
Rationales:
A. Incorrect. Histologically they are classified as juvenile pilocytic astrocytoma. They are much more
common in children with the mean age of presentation around ten years of age. Bilateral tumors
have a frequent association with Neurofibromatosis type 1.
B. Incorrect. May arise from the meninges of the optic nerve or extend from an intracranial location.
On MR imaging the nerve may be identified discrete within the tumor mass. Calcification is a fea-
ture. May be seen in middle-aged women. Also associated with NF1 and NF2 specifically in its
bilateral form.
C. Correct. Characterized by a gradual development of proptosis, this tumor is generally seen in mid-
dle-aged women. Visual loss is a feature. Lesion consists of dilated endothelial lined vascular chan-
nels encompassed by a fibrous pseudocapsule.
D. Incorrect. These lesions can arise from any of the cranial nerves that innervate the extra ocular mus-
cles, CN V, as well as sympathetic and parasympathetic nerves.
33 American College of Radiology
34. Section XII – Neuroradiology
Concerning the LeFort classification of facial injuries, which one is TRUE?
312.
A. All types involve the pterygoid plates and nasal region.
B. All types involve the orbital floors and zygomas.
C. The Type III injury is characterized by a free floating palate (transmaxillary fracture).
D. The type II injury is characterized by cranial facial dissociation.
Question #312
Rationales:
A. Correct. LeFort Fractures basically occur along weakness planes in the facial skeleton. These
include the two structures mentioned above.
B. Incorrect. The LeFort type I injury specifically does not involve the orbits with the blow and frac-
ture line occurring at the level of the maxilla. The fracture includes the entire palate, maxillary and
alveolus teeth and portions of the pterygoid plates. The zygoma is not included in the classification
of LeFort fractures.
C. Incorrect. This describes the Type I injury.
D. Incorrect. This describes the Type III injury.
34
Diagnostic In-Training Exam 2006
35. Section XII – Neuroradiology
Concerning diastematomyelia, which one is TRUE?
313.
A. Most commonly encountered neural tube defect
B. Commonly seen in infants of diabetic mothers
C. Complete duplication of the cord with sensory and motor roots originating from each cord
D. Split of the spinal cord separated by bone, cartilage or a fibrous septation
Question #313
Rationales:
A. Incorrect. Meningoceles and myelomeningoceles are the most commonly encountered neural tube
defects.
B. Incorrect. Caudal Regression Syndrome is commonly seen in infants of diabetic mothers.
Diastematomyelias are associated with other spinal anomalies including Chiari II and
myelomeningoceles.
C. Incorrect. This is actually the definition of diplomyelia which is a much more rare anomaly
D. Correct. Diastematomyelia involves a split of the cord into two separate components. As men-
tioned, the division may be the result of bone, cartilaginous or fibrous septation. The separate halves
so to speak may be enclosed in a single dural sac or the split may involve the dura as well.
35 American College of Radiology
36. Section XII – Neuroradiology
Concerning dementia, white matter predominance is the dominant feature in which one of the
314.
following?
A. Alzheimer disease
B. Binswanger disease
C. Multi infarct dementia (MID)
D. Pick disease
Question #314
Rationales:
A. Incorrect. AD is characterized by cortical atrophy most prominent in the temporal lobes. The dis-
ease is centered in the hippocampus and parahippocampal regions with temporal horn dilatation
appreciated.
B. Correct. Binswanger Disease is a demyelinating disease in patients greater than 55 years of age. It
is associated with hypertension in the vast majority of patient’s. Lack of focal stroke syndromes aids
in the differentiation from multi infarct dementia.
C. Incorrect. Though a disease that involves the white matter, severe deep grey matter infarction is a
major component of this disease as the pathophysiology is the result of atherosclerosis of the deep
penetrating arteries.
D. Incorrect. Similar to AD, Pick disease involves the anterior temporal lobes. However, Pick disease
involves the inferior frontal regions as well. There may be associated caudate atrophy as we
36
Diagnostic In-Training Exam 2006
37. Section XII – Neuroradiology
Concerning spinal dural arteriovenous fistulas, which one is TRUE?
315.
A. Men and women are affected equally.
B. The vertebral body is frequently involved.
C. It is the most common spinal vascular malformation.
D. Patients most commonly present with acute hemorrhage.
Question #315
Rationales:
A. Incorrect. Males are more commonly affected than females with age of onset somewhere in the fifth
to sixth decade.
B. Incorrect. This is a feature of the Juvenile AVM also termed type III in Spetzler classification.
C. Correct. SDAVF is the most common. There is usually a single feeding radicular artery draining
into pial surface veins. In most cases, treatment is endovascular unless the anterior spinal artery
arises from the same level.
D. Incorrect. Patients, most commonly elderly males, present with gradual onset of lower extremity
weakness. Myelopathy as opposed to hemorrhage is identified on imaging studies in combination
with subtle dilatation of spinal surface vasculature.
37 American College of Radiology
38. Section XII – Neuroradiology
316. Transtentorial herniation is associated with infarction in which one of the following vascular
territories?
A. Anterior cerebral artery
B. Posterior cerebral artery
C. Middle cerebral artery
D. Basilar artery
Question #316
Rationales:
A. Incorrect. The anatomy around the tentorium is such that the anterior cerebral artery is not vulnera-
ble when the temporal lobe shifts over the tentorium in transtentorial herniation. The anterior cere-
bral artery is more frequently compromised in subfalcine herniation.
B. Correct. In transtentorial herniation, as the temporal lobe moves over the tentorium, compression of
the 3rd nerve, the posterior cerebral and anterior choroidal arteries and the midbrain occurs.
Vascular compression of the posterior and anterior choroidal arteries by the medial temporal lobe
against the tentorium or by the petroclinoid ligament results in infarction.
C. Incorrect. The middle cerebral artery is not vulnerable in transtentorial herniation secondary to
anatomy in this region (See No.1).
D. Incorrect. The brainstem can be affected in transtentorial herniation but this is manifest by small
hemorrhages in the tegmentum of the pons and midbrain called Duret’s hemorrhages.
38
Diagnostic In-Training Exam 2006
39. Section XII – Neuroradiology
317. Which one of the following is NOT usually associated with a tethered cord?
A. Spinal lipoma
B. Chiari I malformation
C. Thick filum terminale
D. Diastematomyelia
Question #317
Rationales:
A. Incorrect. Spinal lipomas are frequently associated with all forms of spinal dysraphism, especially
those with a low conus and tethered cord
B. Correct. The Chiari I malformation is associated with syringo-hydromyelia in 20-60% but not with
meningomyelocele or other forms of cord tethering.
C. Incorrect. A thick filum terminale is the rule with tethered cords.
D. Incorrect. Diastematomyelia is characterized by a sagittal clefting of the spinal cord or filum termi-
nale. A low lying or tethered cord is present in about 40%.
39 American College of Radiology
40. Section XII – Neuroradiology
318. Progressive intracranial occlusive arteriopathy (Moyamoya syndrome) is associated with ALL of
the following conditions EXCEPT:
A. Sickle cell disease
B. Neurofibromatosis type 1
C. Tuberous sclerosis
D. Radiation therapy
Question #318
Rationales:
A. Incorrect. Moyamoya is seen in sickle cell disease secondary to stenosis/occlusion within the distal
internal carotid artery and proximal aspects of the middle and anterior cerebral arteries. These find-
ings are secondary to ischemia in the vasa vasorum with subsequent intimal and medial hyperplasia
B. Incorrect. Vascular dysplasia sometimes occurs in neurofibromatosis type 1. This most commonly
consists of intimal proliferation with resultant stenosis/occlusion involving the carotid, middle cere-
bral and anterior cerebral arteries. Moyamoya pattern is seen in 60-70% of these patients.
C. Correct. Tuberous sclerosis is a neurocutaneous syndrome characterized by subependymal nodules,
cortical hamartomas, giant cell astrocytomas, neuronal migration anomalies and many additional
findings outside the central nervous system. There is no known association with moyamoya.
D. Incorrect. Radiation therapy can produce arterial injury including medial hyperplasia, intimal fibro-
sis, and endothelial degeneration. These can then produce vascular stenosis/occlusion resulting in a
moyamoya pattern of collateral circulation.
40
Diagnostic In-Training Exam 2006