Downloaded 12 times
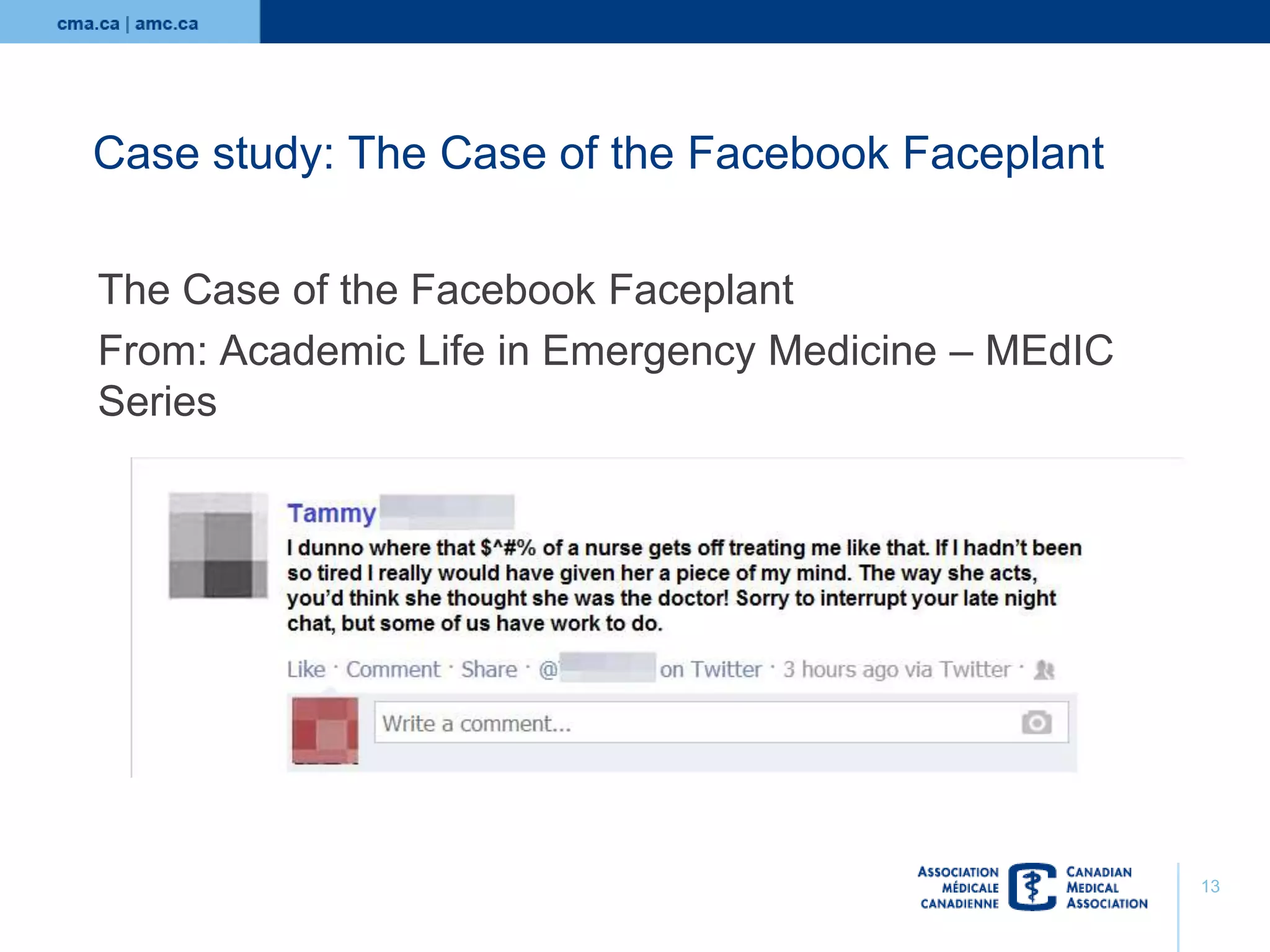
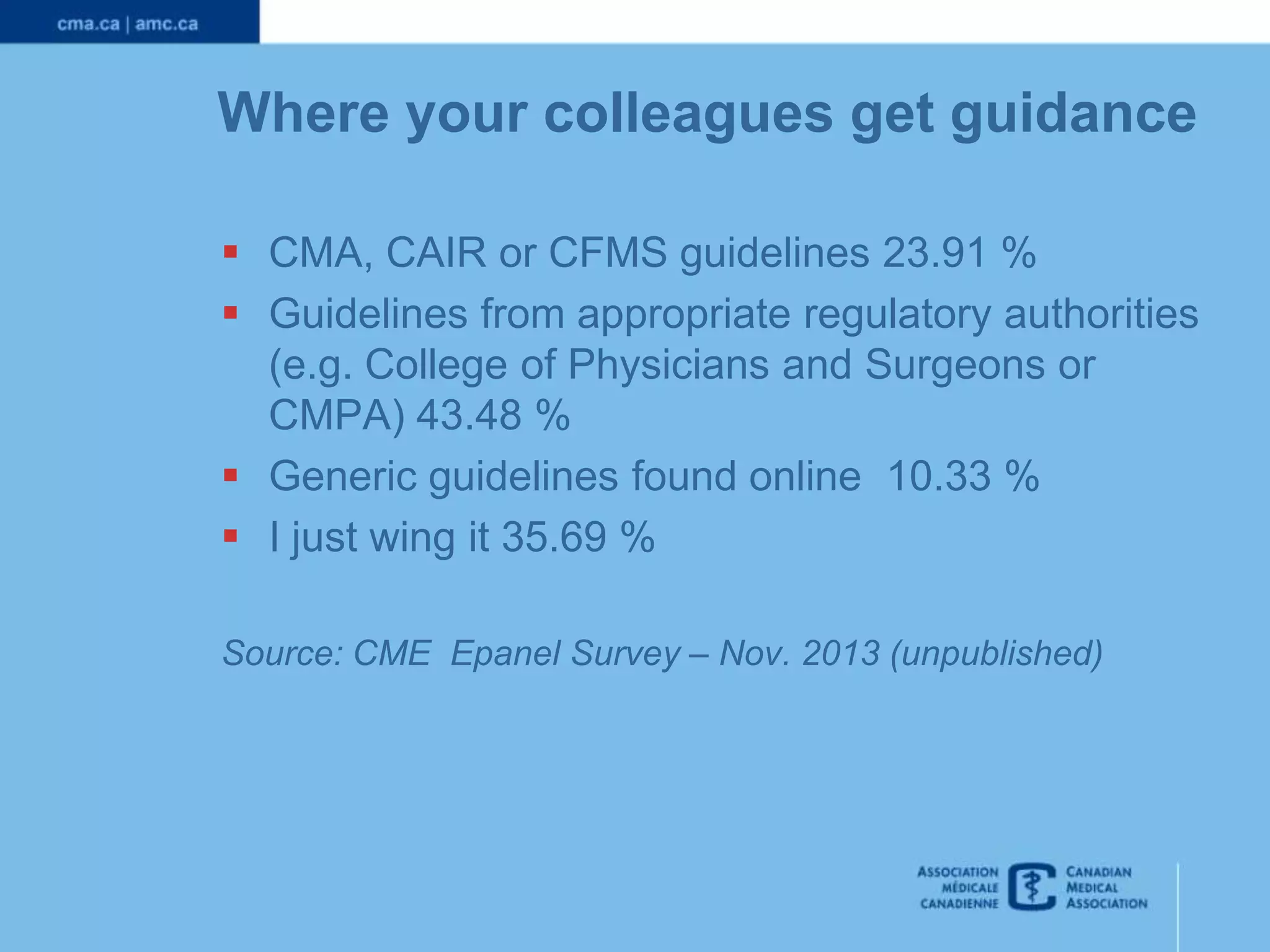
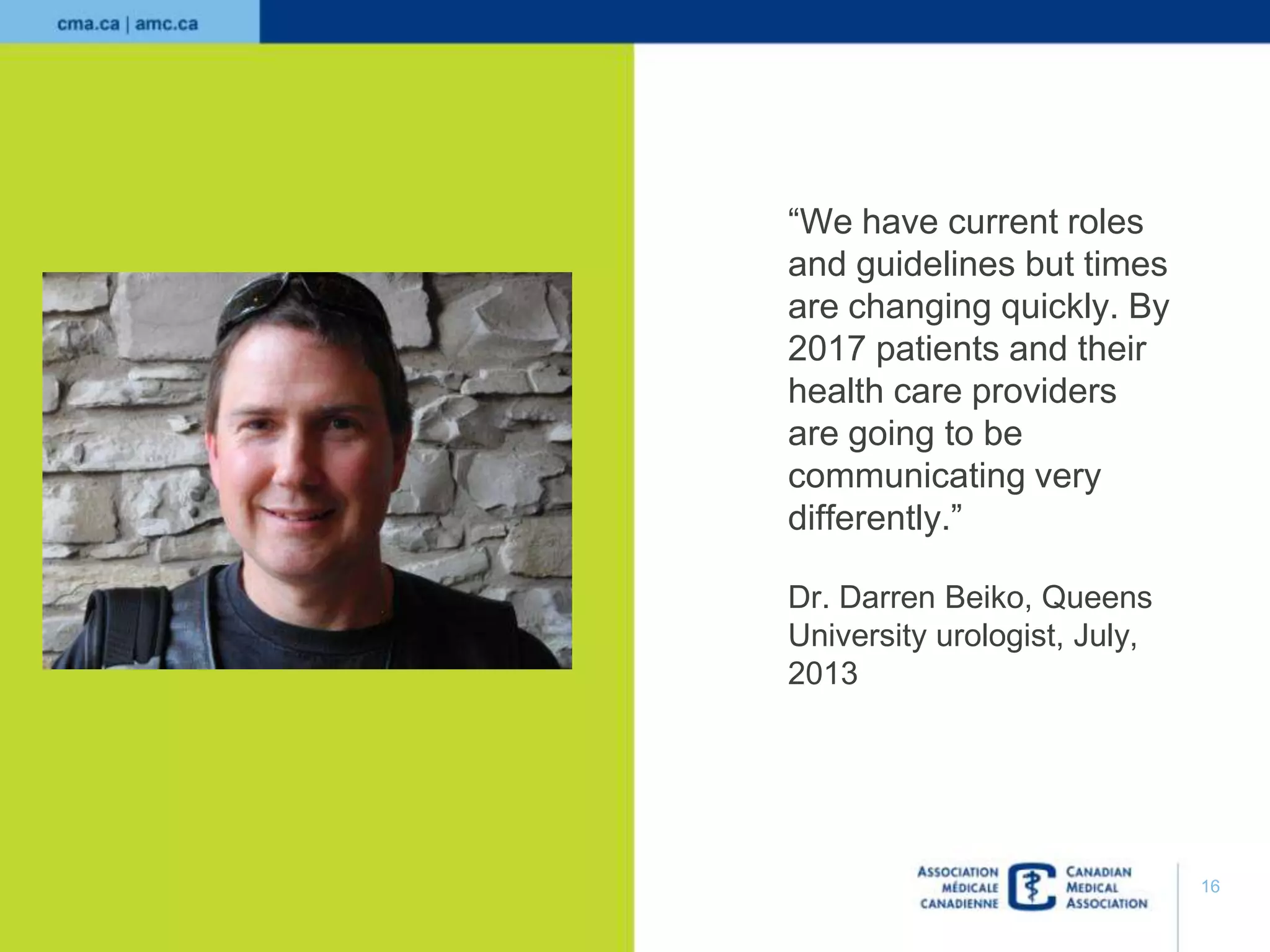




This document provides guidance for medical residents on the professional use of social media. It discusses challenges around privacy, boundaries and ethics that physicians face with social media use. It emphasizes applying the same principles of professionalism online as in person, and respecting patient confidentiality. The document also offers suggestions for appropriate social media use during residency, such as using platforms like Facebook to connect with colleagues and LinkedIn to build professional networks. Overall, it encourages residents to consider social media as a learning tool and for disseminating information, if used responsibly and respectfully.



































































