Anca vasculitis & anti gbm
•Download as PPTX, PDF•
18 likes•3,736 views

Dr Shrier presents a complete review on ANCA vasculitis and Anti GBM disease

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Anca vasculitis & anti gbm
Similar to Anca vasculitis & anti gbm (20)
More from Hofstra Northwell School of Medicine
More from Hofstra Northwell School of Medicine (20)
Recently uploaded
Recently uploaded (20)
Anca vasculitis & anti gbm
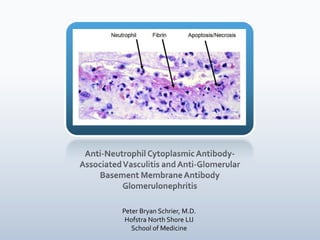
- 1. Anti-Neutrophil Cytoplasmic Antibody-Associated Vasculitis and Anti-Glomerular Basement Membrane Antibody Glomerulonephritis Peter Bryan Schrier, M.D. Hofstra North Shore LIJ School of Medicine
- 2. Today’s Discussion Introduction to Vasculitis Classification Specifically small vessel vasculitis and ANCA vasculitis What are ANCA’s, anyway? Introduction to ANCAs and ANCA-associated vasculitis Wegener’s Granulomatosis With brief MPA discussion Churg-Strauss Syndrome Anti-GBM antibody syndrome/Goodpasture’s Disease
- 3. Introduction to Vasculitis Classification
- 4. Clinical Classification of Systemic Vasculitis
- 7. What are ANCA’s, anyway? Introduction to ANCAs and ANCA-associated vasulitis
- 8. What are ANCAs? Anti-neutrophil cytoplasmic antibodies Antibodies against myeloperoxidase (MPO-ANCA) and Proteinase 3 (PR3-ANCA) MPO & PR3 are found in the azurophilic granules of neutrophils and the lysosomes of monocytes. ANCAs are autoantibodies Therefore ANCA-associated vasculitis is an autoimmune disease John H. Stone, MD, MPH
- 9. ANCA testing 2 methods Immunofluorescence Uses alcohol-fixed buffy coat leukocytes More sensitive ELISA Uses purified specific antigens (MPO and PR3) If Pt’s blood has antibodies to the antigens, result + More specific John H. Stone, MD, MPH
- 10. Immunofluorescence Cytoplasmic or Perinuclear patterns Cytoplasmic immunofluorescence pattern (C-ANCA) Most often associated with anti-proteinase 3 Can occur with MPO Perinuclear immunofluorescence pattern (P-ANCA) Almost always associated with myeloperxidase Perinuclear pattern is due to an artifact of ethanol fixation of anti-MPO leading to positively charged granules that are attracted to the negatively charged nucleus
- 11. ANCA testing Although particular ANCAs are linked with particular diseases, it is possible to be ANCA + without manifesting a disease syndrome, and it is possible to manifest a traditional ANCA-associated vasculitis without + ANCAs Any of the ANCA-associated vasculitides can be associated with either type of ANCA or no ANCAs at all. Other autoimmune disease can be ANCA positive, at least on immunofluorescence
- 12. ANCA in Vasculitis and other Autoimmune Diseases
- 14. ANCA in Vasculitis and other Autoimmune Diseases
- 15. What to do?
- 16. Pathophysiology of ANCA-Associated Vasculitis
- 17. Pathophysiology of ANCA-Associated Vasculitis Journal of Leukocyte Biology. 2003;74:3-15.
- 18. Pathophysiology of ANCA-Associated Vasculitis
- 19. Clinical Classification of Systemic Vasculitis
- 20. Wegener’s Granulomatosis Vasculitis of small and medium sized arteries Systemic necrotizing angiitis Necrotizing granulomatous inflamation of the respiratory tract Necrotizing glomerulonephritis Peak age 35-50 yrs. Male: Female 1.5:1 90% European descent
- 21. Clinical Presentation (Including RPGN)
- 23. Diagnostic Criteria for Wegener’s Granulomatosis (ACR) British Journal of Rheumatology 1997;36:453–458
- 24. Diagnostic Criteria for Wegener’s Granulomatosis (CHCC) British Journal of Rheumatology 1997;36:453–458
- 25. Proposed Pathogenesis PR3-ANCA (anti-proteinase-3) activation of primed neutrophils Production of reactive oxygen species Realease of lytic enzymes from lysosomes Elastases Proteinase-3 (PR3) after all degrades proteins! Leads to tissue injury Kallenberg CGM. Pathogenesis of PR3-ANCA associated vasculitis. J Autoimmun. February-March 2008;30:29-36
- 26. Proposed Pathogenesis Genetic Associations Specific alleles of Cytotoxic T-lymphocyte antigen 4 (CTLA-4) Specific alleles of Fcγ IIIb receptor on neutrophils, monocytes, and macrophages A defective alpha-1 antitrypsin allele Environmental Associations Northern latitudes Farming Environmental allergies and drug allergies Silica or solvent exposure Nasal staphlococcus aureus > associated with relapses Bactrim has been shown to decrease relapse
- 27. Diagnosis for the Nephrologist Routine Labs Elevated BUN & creatinine Anemia- normocytic Leukocytosis Neutrophil predominant NO eosinophilia Rheumatologic non-specific Erythrocyte Sedimentation Rate C-reactive Protein Rheumatoid Factor Anti-nuclear Antibodies
- 28. Diagnosis for the Nephrologist Urinalysis with microscopic examination Hematuria/ Red cell casts Proteinuria “active urinary sediment” Serologic Studies ANCA Most often C-ANCA but can be P-ANCA or ANCA negative Confirm with ELIZA for anti-PR3 Imaging Chest Xray or CT BIOPSY!!!
- 29. Imaging
- 30. Biopsy
- 31. Biopsy Z. Xu, MD.
- 32. Treatment- Induction Cytotoxics Cyclophosphamide- Oral vs. Intravenous X 3-6 months Same rate of inducing remission Oral has fewer relapses, but more side effects (leukopenia, infection) Rituximab For patients who refuse cyclophosphamide because of risks (e.g. fertility) or have other contraindications For cyclophsophamide-resistant patients Methotrexate for non-organ-threatening disease Nephrol Dial Transplant. 2001;16(10):2018-27 Ann Intern Med. 2009;150(10):670-80
- 33. Treatment- Induction Glucocorticoid Pulse vs. standard dose Daily oral glucocorticoid taper over 4-6 months Alternate day glucocorticoids is no longer done Plasma exchange (controversial) Severe renal dysfunction (creat >5.7/ pt requiring HD) Diffuse alveolar hemorrhage PCP prophylaxis with trimethoprim/ sulfamethoxazole during induction with cytotoxics Use atovaquone for methotrexate
- 34. Treatment- Maintenance Birmingham Vasculitis Activity Score adjusted for Wegener’s should be used to assess remission and replapse Azathioprine vs. Methotrexate X 12-18 months Azathioprine for GFR<50 ml/min Azathioprine after induction with Methotrexate Methotrexate only if induction was with Cyclophosphamide Mycofenolate Mofetil or Rituximab may be used if azathioprine and methotrexate are not tolerated/contraindicated or if there are relapses while on MTX or AZA
- 35. Microscopic Polyangiitis Most common ANCA vasculitis Median age ~ 50s Vasculitis of small and medium sized arteries Renal lesions same as with Wegener’s, but most often renal-limited No granulomas More often MPO-ANCA, but can be PR3-ANCA and, rarely, ANCA negative.
- 37. Microscopic Polyangiitis May be on the same disease spectrum as Wegener’s Granulomatosis Treatment is the same as for Wegener’s, based on the Birmingham Vasculitis Activity Score
- 38. Churg-Strauss Syndrome Allergic Granulomatosis and angiitis Vasculitis of small and medium sized arteries Necrotizing vasculitis Builds over years until full presentation as it progresses through the following phases: Prodromal Phase- teens-20s Allergic rhinitis Asthma Eosinophilic phase Vasculitic phase as early as 20s-30s, but mean age is 50s Curr Opin Rheumatol. 2010;22(1):21-8
- 39. Clinical Presentation Causes 50% deaths from CSS
- 41. Diagnostic Criteria for Churg-Strauss (ACR) British Journal of Rheumatology 1997;36:453–458
- 42. Diagnostic Criteria for Churg-Struass (CHCC) British Journal of Rheumatology 1997;36:453–458
- 44. Diagnosis for the Nephrologist Routine Labs Elevated BUN & creatinine Eosinophilia (>10%) Anemia Rheumatologic Erythrocyte Sedimentation Rate C-reactive Protein Rheumatoid Factor Urinalysis with microscopic examination Hematuria/ Red cell casts Proteinuria active urinary sediment
- 45. Diagnosis for the Nephrologist Serologic Studies ANCA Often P-ANCA but can be C-ANCA or ANCA negative Confirm with ELIZA for anti-MPO Elevated IgE levels Hypergammaglobulinemia Elevated eosinophilic cationic protein (ECP) Bronchioalveolar Lavage (BAL) with eosinophilia Imaging Chest Xray or CT BIOPSY!!!
- 46. Imaging
- 47. Biopsy Eosinophilic infiltrates Prominent necrosis Giant cell vasculitis of small arteries and veins Interstitial and perivascular necrotizing granulomas Eosinophilic leukocytoclastic angiits
- 48. Biopsy
- 49. Treatment- Assess Disease Severity Five Factors Score Cardiac involvement Gastrointestinal involvement Renal involvement (creatinine > 1.58mg/dl) Proteinuria (>1g/24h) Central nervous system involvement Birmingham Vasculitis Activity Score also used on occasion These help assess disease severity and determine aggressiveness of initial treatment
- 50. Treatment- Induction Glucocorticoids Pulse vs. standard dose depending on severity Daily oral glucocorticoids tapered symptoms and eosinophilia improve over 12-18 months Are often continued for other reasons (e.g. severe asthma) Cyclophosphamide Only in severe cases (although renal involvement is usually enough to qualify as as severe case) Daily oral vs. monthly IV Daily oral with slightly more side effects Monthly IV with slightly more relapse Usually achieve remission within 6 months
- 51. Treatment Maintenance Azathioprine vs. Methotrexate X 12-18 months Azathioprine preferred over methotrexate Methotrexate pneumonitis complicates matters Second line- for relapses or refractory cases Mycofenolate Mofetil Intravenous Immunoglobulin (IVIG) Hydroxyurea Interferon-alpha Rituximab (though may cause bronchospasm)
- 52. Drug-Induced ANCA Vasculitis Propylthiouracil (PTU) Accumulates in neutrophils and binds to MPO Alters the MPO antigen ? autoantibodies Usually resolves with d/c PTU Hydralazine Drug-induced SLE and Drug-induced ANCA vasculitis Requires d/c hydralazine and corticosteroids + cyclophosphamide Minocycline P-ANCA, but against antigens other than MPO Others: Sulfonamides, Penicilliamine, allopurinol John H. Stone, MD, MPH
- 53. Anti-Glomerular Basement Membrane Antibody Syndrome
- 54. Anti- GBM Acute or Rapidly Progressive Glomerulonephritis Circulating autoimmune antibodies against the glomerular basement membrane Nomenclature When renal-limited, the disease is called Anti-GBM Antibody Syndrome When pulmonary hemorrhage is also present, the disease is called Goodpasture’s disease (after the doctor who first described it) Sometimes any pulmonary renal syndrome with pulmonary hemorrhage is called Goodpasture’s Syndrome
- 55. Anti-GBM Anti-GBM disease is rare; approximately 1 per million Found in all age groups Tends to present as Goodpasture’s disease in younger patients (age<30) and as anti-GBM antibody syndrome in older patients (age>50) Prognosis is overall poor It is especially poor if renal function is poor Once recovery is successful, it rarely relapses
- 56. Pathogenesis
- 57. Pathogenesis
- 58. Pathogenesis Pharmaceutical Research, Vol. 25, No. 12, December 2008 (# 2008)
- 59. Possible Associations HLA-DR15 haplotype (especially DRB 1*1501 allele) Found in 80% of patients with anti-GBM disease This may have something to do with T-cell recognition of an epitope that is usually degraded by endosomal proteases before T-cell maturation It is possible that T-cells then sensitize B-cells to produce anti-GBM antibodies Regulatory CD25+ T-cells attenuate the glomerular injury Pulmonary hemorrhage usually requires initial insult to the lung to expose the NC1 domain of the type 3 collagen e.g. cigarette smoke, respiratory infection, etc.
- 60. Clinical Presenation Rapidly Progressive Glomerulonephritis +- Pulmonary hemorrhage Increased DLCO No systemic complaints (malaise, fever/chills, weight loss,etc.)
- 61. Diagnosis Routine Labs Eleavated BUN & creatinine Rapidly Progressive rise in creatinine over time Urinalysis with microscopic examination Hematuria/ Red cell casts Proteinuria active urinary sediment Serologies Anti-GBM antibody (though this is not always reliable) ANCAs are positive in up to 1/3 of patients Usually P-ANCA
- 62. Biopsy
- 64. Treatment Outcome best correlated with % crescents >75% crescents almost always indicates nearly 0% chance of renal recovery Initial management Plasmapharesis/exchange X 2-3 weeks Pulse glucocorticoids followed by standard dose PO Cyclophosphamide (PO vs IV) Duration of treatment 3-4 months if serological conversion to anti-GBM negative Longer if anti-GBM remains positive (~ 6-9 months) If still anti-GBM positive after 3 months, Azathioprine may be substituted for cyclophosphamide
- 65. Treatment Patient’s requiring aggressive treatment: Concurrent ANCA vasculitis (or just positive ANCAs!) Systemic vasculitic symptoms (rash, arthralgia, etc) Pulmonary hemorrhage Maintenance Prednisone X 6-9 mo vs. 1 mo. taper to off +-Azathioprine X 6-9 months If true remission (serological and symptomatic), pt’s usually do not relapse, and treatment can usually be discontinued
- 66. Today’s Discussion Introduction to Vasculitis Classification Specfically small vessel vasculitis and ANCA vasculitis What are ANCA’s, anyway? Introduction to ANCAs and ANCA-associated vasulitis Wegener’s Granulomatosis With brief MPA discussion Churg-Strauss Syndrome Anti-GBM antibody syndrome/Goodpasture’s Disease
Editor's Notes
- ANCA produce tissue damage by activating cytokine-primed neutrophils and monocytesThese activated neutrophils adhere to endothelial cells, releasing proteolytic granule contents and proinflammatory cytokines
- The release of inflammatory cytokines causes the downstream release of reactive oxygen species and oxidative damage, which further activates the endothelium causing more inflammation…In short, ANCAs activate neutrophil
- Focal glomerulonephritis with crescent formation on renal biopsy specimen, characteristic of Wegener granulomatosis.
- Lung biopsy specimen from a patient with Wegener granulomatosis showing evidence of vasculitis and inflammation
- CYCLOPS trial - Pulse IV vs. daily PO
- MEPEX trial –Plasmapharesis vs IV methylprednisolone BOTH WITH PO prednisone and cyclophosphamide (not the best trial)
- CYCAZAREM- Azathioprine vs. Cycophosphamide in maintenance. Same efficacy, MANY fewer complications. So we use Azathioprine. Another study compared MTX & AZA. Same relapse rate. Same side effect rate, just different side effects.
- Pathogenetic model proposed for Churg–Strauss syndrome, based on available experimental evidence. Hypothetical allergens or antigens may be uptaken by antigen-presenting cells and presented to CD4+ T cells, leading to T-cell activation and expansion. Antigen-presenting cells (which can be of different cell types, for example, dendritic cells, monocyte macrophages, and eosinophils) have a restricted HLA repertoire and often express HLA-DRB4. Once activated, CD4+ T cells secrete IFN-γ, which promotes granulomatous inflammation, and also drive eosinophil activation and expansion through the secretion of IL-4, IL-5, and IL-13, or by means of the CD95–CD95L pathway. Eosinophils mediate tissue damage mainly by secreting granule proteins such as ECP and MBP. Endothelial cells may also contribute to tissue infiltration by eosinophils by releasing eotaxin-3, a chemokine with strong chemotactic activity on eosinophils. B cells are also likely to play a pathogenetic role: activated on antigen encountering and 'helped' by T-helper 2 cytokines such as IL-4 and IL-13, they may become mature plasma cells and then produce different autoantibodies, including ANCA, which may in turn mediate vasculitis. ANCA, anti-neutrophil cytoplasmic antibodies; CD95L, CD95 ligand; ECP, eosinophilic cationic protein; IFN-γ, interferon-γ; IL(-4, -5, -13), interleukin(-4, -5, -13); MBP, major basic protein; TCR, T-cell receptor.
- The most common radiological manifestations consist of transient, patchy, nonsegmental areas of consolidation without predilection for any lung zone.[24-26] The areas of consolidation can be symmetric or asymmetric and may have a peripheral distribution similar to that seen in chronic eosinophilic pneumonia[25,26] (Fig. 5). Less common manifestations include small or large nodules, unilateral or bilateral pleural effusions, and hilar lymphadenopathy.
- Skin & Kidney
- Type IV collagen
- Alpha 3, alpha 4, alpha 5 form a triple helical molecule (the promotor) which then dimerize to form a Hexamer of type IV collagen.
- Fig 1 A hypothetical structure of α3 chain type IV collagen. Linear structure of human α3 chain type IV collagen composed of three distinct domains: a cysteine rich N-terminal 7S domain, a central triple helical domain with multiple small interruptions and a globular C-terminal non-collagenous (NC1) domain.
- Crescentic glomerulonephritis (RPGN)