De quervain's
•Download as PPTX, PDF•
55 likes•23,318 views

This is a student project, presented by Ms Yeo during her clinical attached at my Centre!

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (18)
Similar to De quervain's
Similar to De quervain's (20)
Recently uploaded
Recently uploaded (20)
De quervain's
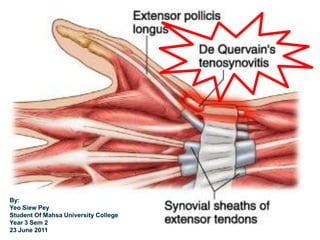
- 2. de Quervain's Disease Named after a Swiss surgeon, Fritz de Quervain, whom first described the problem in 1895. It is a progressive stenosing tenosynovitis which affects the tendon sheaths of the 1st dorsal compartment of the wrist. Characterised by degeneration and thickening of the tendon sheath.
- 3. 1st dorsal compartment contains the tendons and synovial sheaths of APL and EPB tendons.
- 4. Etiology Inflammation of synovial sheaths results from continuous repetitive use of EPB and APL muscle. ↓ Scarring and thickening of tendon sheaths. Stenosing, increase friction ↓ Inflammation ↓ Degeneration RA – affect synovial proliferation and swelling in tendon sheaths
- 5. Predisposing Factors Overuse injury Repetitive tasks that involve overexertion of thumb, radial and ulnar deviation of the wrist Arthritis Activities such as: Wringing out wet clothes. Hammering. Painting. Skiing. Knitting. Lifting heavy objects such as a jug of milk, taking a frying pan off of the stove, or mother lifting a baby out of a crib (baby wrist).
- 6. Incidence and Prevalence: Usually a gradual and insidious onset of dull ache over radial aspect of the wrist. Occurs most often in individuals age between 30 and 50 y.o 10 times more common in women. Higher risk for workers / sports that perform repetitive activities requiring sideways movement of the wrist while gripping the thumb (eg. hammering, some assembly line jobs, skiing, golf)
- 7. Sign & Symptoms Localised swelling and tenderness in the region of radial styloid process. Pain while performing ulnar deviation, thumb flexion and adduction. Diagnosis Positive Finkelstein test Increase pain on active contraction against resistance on thumb extension Xray to r/o bony pathology (eg. scaphoid #, arthritic changes)
- 8. Management Conservative Mx Rest from activity that increases pain / Thumb Spica Splint for 3~4wk Modification of activity Anti-inflammatory medication Corticosteroid injection Physiotherapy Surgical (tenosynovectomy) Only indicated for surgical if symptoms persists > 3mth / conservative failed. A 1-2cm incision is made over the first dorsal compartment and the extensor retinaculum is divided to free the tendons.
- 9. Rehabilitation - ConservativeGoal : Decrease pain and swelling, Activity modification, Restore mobility and strength Treatment: Pain Relieve - Physical modalities Soft Tissue Massage (STM) Tendon gliding ex MWM for wrist & manipulation of thumb. As pain decrease, gradual progress to strengthening ex for wrist and hands
- 10. Rehabilitation – Post Op Day 0-2 - Rest, surgical wound on dressing Day 2-14 - Removal of dressing, Thumb splica splint - Gentle active ROM ex - STO on 10 -14th days - Desensitization – Digital massage on the area of incision 1-6weeks - Gradual progressing strengthening ex - Scars tissue mobilization - Resisted activity to be avoided till 6wks post-op
- 13. 1st Ax on 16 March 2011 SUBJECTIVE ASSESSMENT Name : Mr. AXX Age : 29 y.o Gender: Male Occupation: Lorry Driver Pt’s Problem: - Sudden onset of pain at Left lateral wrist for 2/52 Pain: - Area: Left lateral wrist proximal to radial styloid process - Nature: Sharp pain - Agg: Ulnar deviation, resisted thumb movement - Ease: Rest - 24 hrs: Not specific - Irritability: Low
- 14. Hx of Current Condition: Pt. noticed pain at left lateral wrist in the morning, suspect compressing the thumb during sleep. Did not seek treatment. Pain get worst gradually with activity. Past Medical Hx.: Had wrist fracture 3 years ago. General health: Good Medication: Nil Investigation: Nil Dominant Hand: Right Functional Status / ADL: Patient experience pain in activity that involve grasping and driving. Vital Sign: B/P: 120/80 mmHg
- 15. OBJECTIVE ASSESSMENT Local Observation - Mild swelling at left lateral wrist as compare to right side. - No open wound / haematoma Palpation - Tenderness at base of left thumb and radial styloid process.
- 16. Movement Active ROM of left wrist, with end-range-pain on ulnar and radial deviation Active ROM of thumb, with end-range-pain on thumb extension and abduction. Active ROM of elbow and neck motions were full and pain free. Muscle Power (Oxford grading) Muscle grading were deferred d/t resisted movement involving thumb and wrist were painful. All other fingers tested normal. Special Test Finkelstein’s test – Positive
- 17. Analysis - Impaired motor function and ROM associated with inflammation of EPB and APL tendons and tendon sheaths suggesting de Quervain’s disease. Short Term Goal -To control pain to tolerable level with activity in 1/52 - To reduce swelling in 1/52 - To preserve ROM, muscle length and strength Long Term Goal - Pain free thumb and wrist motions in 2/12 - Strengthen muscle power of left wrist and thumb to 5/5 - Prevent complication and recurrent pain
- 18. Plan WAX Soft Tissue Massage (STM) Tendon gliding ex MWM for wrist & manipulation of thumb. Strengthening ex for wrist and hands Patient education on activity modification Intervention 1) Hot cold test √ 2) WAX bath 3) Transverse friction massage on EPB & APL tendon 4) Tendon gliding ex for EPB & APL 5) MWM for wrist flexion & extension 6) Thumb manips 7) Ultrasound at lateral wrist (1MHz, 1.0W/cm2, 3mins) 8) Home exercise programme – STM, tendon gliding ex, pain free ROM ex 9) Patient was told to rest left thumb and avoid aggravating motions and activities.
- 19. EVALUATION - Pt. able to perform wrist and thumb motions with lesser pain. Motions felt less restricted. REVIEW - To review patient’s pain scale and joint motions. KIV muscle power test when pain reduce. Gradually increase ex intensity and progress to strengthening ex.
- 20. Conclusion Most individuals does not require surgery and will recover with rest or injections within 6wk times. Surgical cases may require up to 3-6 months to regain pre-operative strength. Recurrence of the symptoms is very rare. Complications Possible problems after the surgery can include irritation of the small nerves which give feeling of numbness or tingling sensation to the area of skin on the wrist and back of the hand. Previous injury that altered the anatomy of the wrist would make treatment more difficult.
- 22. References Brotzman, S. and Wilk, K. (2003) Clinical Orthopaedic Rehabilitation, 2nd ed. Philadelphia: Mobsy, p.72-75. Dutton, M. (2008) Orthopaedic Examination, Evaluation, and Intervention, 2nd ed. USA: The Mc-Graw Hill, p.810-828. Website: http://www.ajronline.org/cgi/content/full/182 /3/719