anatomy of wrist and carpal bones
•Download as PPTX, PDF•
52 likes•13,024 views

osseous and ligamentous anatomy

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to anatomy of wrist and carpal bones
Similar to anatomy of wrist and carpal bones (20)
Recently uploaded
Recently uploaded (20)
anatomy of wrist and carpal bones
- 1. Anatomy of wrist & carpal bones
- 2. Osseous anatomy • The distal ends of the radius and ulna articulate with the two carpal rows (proximal and distal), and these articulate with the bases of the five metacarpal bones .
- 4. • The proximal row of carpal bones termed as intercalated segment because forces acting on its proximal & distal articulations determine its position
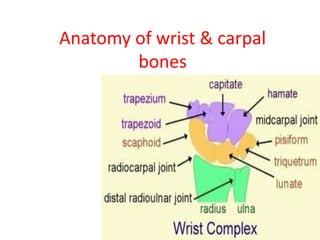
- 5. CARPAL BONES Carpal bones are arranged in two rows From lateral to medial and when viewed from anteriorly • PROXIMAL ROW 1. the boat-shaped scaphoid; 2. the lunate, which has a 'crescent shape'; 3. the three-sided triquetrum bone; 4. the pea-shaped pisiform • DISTAL ROW 1. the irregular four-sided trapezium bone; 2. the four-sided trapezoid; 3. the capitate, which has a head; 4. the hamate, which has a hook
- 6. General Features of Carpal Bones • 1. The proximal row is convex proximally, and concave distally. 2. The distal row is convex proximally and flat distally. 3. Each bone has 6 surfaces: (i) The palmar and dorsal surfaces are non-articular except for the triquetral and pisiform. (ii) The lateral surfaces of the two lateral bones (scaphoid and trapezium) are nonarticular. (iii) The medial surfaces of the three medial bones (triquetral, pisiform and hamate) are nonarticular. • 4. The dorsal nonarticular surface is always larger than the palmar nonarticular surface, except for the lunate, in which the palmar surface is larger than the dorsal
- 7. Articular Compartmental Anatomy • The wrist joint is separated into a number of compartments by the many ligaments that attach to the carpal bones • These compartments are of considerable significance for the interpretation of standard or MR arthrograms and for identifying various patterns of arthritic involvement
- 8. • The compartments are as follows: • 1. Radiocarpal compartment • 2. Midcarpal compartment • 3. Pisiform-triquetral compartment • 4. Common carpometacarpal compartment • 5. First carpometacarpal compartment • 6. Intermetacarpal compartments • 7. Inferior (distal) radioulnar compartment
- 10. Ligamentous anatomy • Two categories - Intrinsic - Extrinsic
- 12. • Intrinsic ligaments - Scapho-lunate interosseous ligament - Luno-triquetral interosseous ligament
- 13. • Scapholunate interosseous ligament ( SLIL ) : • C shaped structure • 3 parts - dorsal - proximal - volar
- 14. • Dorsal part – 3mm thick, transverse or short oblique fibers • located in the depth of the dorsal capsule and connects the dorsal-distal corners of the scaphoid and lunate bones. • Plays a key role in scapholunate stability.
- 15. • Volar part- has longer, more obliquely oriented fibers • allowing substantial sagittal rotation of the scaphoid relative to the lunate • playing a lesser role in carpal stability • Proximal part – thin, fibrocartilagenous • Follows the arc of the proximal edges of the two bones from dorsal to palmar • separating the radiocarpal and midcarpal jointspaces
- 17. • Lunate Triquetrum Interosseous Ligaments : • Three components- palmar, dorsal & proximal • In contrast to the scapholunate ligaments, the palmar lunate triquetrum ligament is thicker and stronger than the dorsal one
- 19. Extrinsic ligaments • Subdivided into three major subgroups - palmar radiocarpal - palmar ulnocarpal - dorsal radiocarpal
- 20. • Palmar radio-carpal ligaments : • Four palmar ligaments connect the radius to the carpus: -radio-scapholunate -radio-scaphoid-capitate - long radio-lunate -short radio-lunate ligaments
- 22. • The first three ligaments originate from the lateral third of the palmar margin of the distal radius and take an oblique course to insert into the scaphoid tuberosity & lunate(radioscapholunate), the palmar aspect of the capitate (radioscaphoid-capitate), and the lunate (long radiolunate). • The short radiolunate ligament originates from the medial anterior rim of the radius and has a vertical direction until it inserts into the palmar aspect of the lunate
- 23. • The radioscaphoid-capitate ligament courses around the palmar concavity ofthe scaphoid, forming a hinge over which the scaphoid rotates. • Between the two diverging radioscaphoid- capitate and long radiolunate ligaments, there is the so-called interligamentous sulcus (space of Poirier), which represents a weak zone through which perilunate dislocations frequently occur
- 24. Palmar Ulnocarpal Ligaments • Superficial extrinsic ulnar-capitate • Ulnar-triquetrum • Ulnar-lunate • Volar radioulnar
- 26. Dorsal Radiocarpal Ligaments • The only dorsal extrinsic radiocarpal ligament is the dorsal radial triquetrum ligament, also known as the dorsal radiocarpal ligament • this is a wide, fan-shaped ligament that connects the dorsal edge of the distal articular surface of the radius to the dorsal rim of the triquetrum, with some deep fibers inserting onto the lunate, and rarely onto the scaphoid.
- 28. Midcarpal Ligaments • Dorsal – dorsal intercarpal ligament • Palmar – • lateral group - scapho-trapezium-trapezoid - scapho-capitate - capitate-trapezium • Medial group - triquetro-capitate - triquetro-hamate - palmar scaphotriquetrum Lateral group are important in maintaining of normal scaphoid alignment
- 30. • Dorsal intercarpal ligament- • arises from the dorsal ridge of the triquetrum • courses transversely along the distal edge of the lunate • fans out to insert on the dorsal rim of the scaphoid the trapezium, and the trapezoid bones • contributes to increase the depth of the midcarpal socket • having a stabilizing role to the lunocapitate joint
- 31. Vascularity of the Wrist • The blood supply to the wrist is provided by an extrinsic and an intrinsic vascular system • The extrinsic blood supply is developed through branches of the radial, ulnar, and anterior interosseous arteries, which form an arcade of anastomosing branches that produce three dorsal and three palmar arches
- 32. • The dorsal and palmar radiocarpal arches • The dorsal and palmar intercarpal arches • The dorsal basal metacarpal and the deep palmar arches
- 34. • Panagis et al. and Gelberman and Gross classified the carpal bones into three groups on the basis of • the number and location of nutrient vessels, • the presence or absence of intraosseous anastomoses • and the dependence of large areas of bone on a single vessel. • The clinical significance of the various groups is based on the risk of posttraumatic avascular necrosis for the bones in each group
- 35. • Group I - Includes carpal bones which either have vessels entering from only one surface or • large areas of bone that are dependent on a single vessel. • This group is the most vulnerable to posttraumatic avascular necrosis. • Scaphoid, Capitate, and 8 % or 20 % of the lunates
- 36. • Group II - two or more areas of vessel entry but lack significant anastomoses within the entire or a major part of the bones. • Hamate, Trapezoid
- 37. • Group III - two or more areas of vessel entry and consistent intraosseous anastomoses. • Trapezium, triquetrum , pisiform, and 80 % or 92 % of the lunates
- 38. Innervation of wrist ligaments • The main innervation to the wrist capsule derives from • the anterior interosseous nerve, • lateral antebrachial cutaneous nerve, and • Posterior interosseous nerve. • Other minor sources of capsular innervation include: • The palmar cutaneous branch of the median nerve, • The deep branch of the ulnar nerve, • The superficial branch of the radial nerve, and • The dorsal branch of the ulnar nerve
- 39. BIOMECHANICS • The proximal carpal row has no direct tendon attachments. The moment generated by muscle contraction results in rotation that is initiated at the distal carpal row. • The bones of the proximal row follow passively, when tension within the midcarpal capsule reaches a certain level
- 40. • In kinematic terms, the distal carpal row can be thought of as one rigid functional unit. • The bones of the proximal carpal row seem to be less tightly bound to one another than the bones of the distal carpal row
- 41. • When the wrist is constrained along the sagittal plane, the scaphoid has a larger amount of rotation (average 90% of the total arc of motion) than the lunate (50%) and the triquetrum (65%). • The average scapholunate angle is 76 degrees in full wrist flexion and 35 degrees in full extension. • During radioulnar deviation of the wrist, the three proximal carpal bones move synergistically from a flexed position in radial deviation to an extended position in ulnar deviation
- 42. • During unconstrained flexion of the wrist, the distal row synchronously rotates into flexion, but also into some degree of ulnar deviation. • In contrast, during wrist extension, the tendency of all distal carpal bones is to rotate into extension and a slight radial deviation.
- 45. • It is widely accepted that the ligamentous restraints stabilizing the scaphoid are classified into primary and secondary
- 46. • Primary stabilizers – scapho-lunate interosseous ligament • Secondary stabilizers- STT, RSC, SC, and the unique V-arrangement of the DIC and DRC ligaments
- 47. • Primary rupture secondary intact -Such cases manifest with SL dissociation without rotary subluxation of the scaphoid (RSS) (widening of the SL space, rupture of the dorsal SL ligament, and normal SL angle) • Primary intact secondary rupture - Such cases manifest with RSS without SL dissociation (foreshortened scaphoid on posteroanterior radiographs with a positive ring sign, increased SL angle, and the dorsal SL ligament macroscopically intact)
- 48. • Biomechanic concepts that have been proposed for better understanding of functioning,movements and various types of forces acting.some of them are: 1. LINK CONCEPT 2. NAVARRO THREE COLUMN CONCEPT 3. ROWS CONCEPT 4. TALEISNIK’S CONCEPT 5. LICHTMAN’S RING CONCEPT 6. WEBER’S TWO COLUMN CONCEPT
- 49. LINK CONCEPT • three links in a chain composed of radius, lunate and capitate – head of capitate acts as center of rotation – proximal row (lunate) acts as a unit and is an intercalated segment with no direct tendon attachments – distal row functions as unit
- 50. 3 COLUMN CONCEPT (Navarro 1935) • lateral (mobile) column – comprises scaphoid, trapezoid and trapezium – scaphoid is center of motion and function is mobile • central (flexion-extension) column – comprises lunate, capitate and hamate – luno-capitate articulation is center of motion – motion is flexion/extension • medial (rotation) column – comprises triquetrum and pisiform – motion is rotation
- 51. ROWS CONCEPT (Johnston 1907) • comprises proximal and distal rows – scaphoid is a bridge between rows • motion occurs within and between rows
- 52. TALEISNIK’S CONCEPT • Modification of the columnar theory • The pisiform does not function as a carpal bone, so it is excluded from the model. • Trapezium and trapezoid are part of the central column
- 53. WEBER’S TWO COLUMN CONCEPT • Weber (1980): Two columns are the load- bearing column (capitate, trapezoid, scaphoid, and lunate) and • the control column (triquetrum and hamate).
- 54. LICHTMAN’S RING CONCEPT • proximal and distal rows are semirigid posts stabilized by interosseous ligaments; • Normal controlled mobility occurs at scaphotrapezial and triquetrohamate joints. • Any break in ring, either bony or ligamentous (arrows), can produce dorsal intercalated segmental instability or volar intercalated segmental instability deformity.
- 56. Craigen and Stanley (1995) • There are two patterns of motion during radioulnar deviation: • the proximal row rotates mostly along the frontal plane (row pattern) or mostly along the sagittal plane (column pattern).
- 57. Stabilizing Mechanism of the Distal Row • Tendons included in the carpal tunnel have divergent directions when they emerge in the palm. • If their corresponding muscles contract, the flexor tendons of the little finger generate a compressive force to the hook of the hamate toward the ulnar side. • This force would be opposite in direction to the force that is generated when the flexor pollicis longus contracts against the inner surface of the trapezium. • Such opposite forces would tend to open the palmar carpal concavity (the trapezium toward the radial side, the hamate toward the ulnar side).
- 58. Stabilizing Mechanism of the Midcarpal Joint • Under axial load, the distal carpal row exerts an axial compressive force onto the proximal row. • Because of its oblique orientation relative to the long axis of the forearm, the loaded scaphoid tends to rotate into flexion and pronation. • If the scapholunate and lunate triquetrum interosseous • ligaments are intact, the flexion moment generated by the scaphoid is transmitted to the lunate and the triquetrum. • Consequently, the unconstrained proximal row would rotate into flexion
- 59. • Especially important midcarpal stabilizers are the STT and scaphoid capitate ligaments laterally andtriquetrum-hamate-capitate ligament (the so- called ulnar leg of the arcuate ligament) medially. • Failure of these ligaments results in a typical carpal collapse characterized by abnormal flexion of the unconstrained proximal row, a fairly typical pattern of carpal malalignment, known as volar intercalated segment instability (VISI)
- 60. Stabilizing Mechanism of the Proximal Row • When axially loaded, the three proximal bones are not equally constrained by the palmar-crossing midcarpal ligaments. • Because of the peculiar arrangement of the STT and scaphoid capitate ligaments, the scaphoid is allowed larger rotation into flexion and pronation than the lunate, whereas the triquetrum is tightly constrained by its attachments to the distal row. • If palmar and dorsal scapholunate and lunate • triquetrum ligaments are intact, such differences in angular rotation are likely to generate increasing torque and intercarpal coaptation of the scapholunate and lunate triquetrum joints, contributing further to their stability
- 61. • . If the scapholunate ligaments are completely torn, the scaphoid no longer is constrained by the rest of the proximal row and tends to collapse into an abnormally flexed and pronated posture (the so-called rotatory subluxation of the scaphoid) • whereas the lunate and triquetrum are pushed by the distal row into an abnormal extension, known as a dorsal intercalated segment instability (DISI
- 62. • If, instead of the scapholunate, the lunate triquetrum ligaments fail, the scaphoid • and lunate tend to adopt an abnormal flexed posture (VISI), whereas the triquetrum remains solidly linked to the distal row