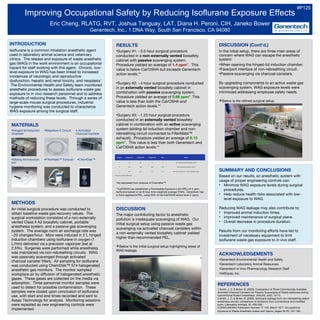
1. RESULTS
•Surgery #1: ~3.5 hour surgical procedure
conducted in a non-externally vented biosafety
cabinet with passive scavenging system.
Procedure yielded an average of 1.4 ppm*. This
value is below Cal/OSHA but exceeds Genentech
action levels.**
•Surgery #2: ~4 hour surgical procedure conducted
in an externally vented biosafety cabinet in
combination with passive scavenging system.
Procedure yielded an average of 0.66 ppm*. This
value is less than both the Cal/OSHA and
Genentech action levels.**
•Surgery #3: ~1.25 hour surgical procedure
conducted in an externally vented biosafety
cabinet in combination with an active scavenging
system (sliding-lid induction chamber and non-
rebreathing circuit connected to FilterMate™
exhaust). Procedure yielded an average of 0.12
ppm*. This value is less than both Genentech and
Cal/OSHA action levels.**
*As calculated from analysis of Chemdisk™.
**Cal/OSHA has established a Permissible Exposure Limit (PEL) of 2 ppm
isoflurane based on an 8-hour time-weighted average (TWA). Genentech has
a more aggressive PEL, using 50% of the Cal/OSHA action level (1 ppm).
Improving Occupational Safety by Reducing Isoflurane Exposure Effects
Eric Cheng, RLATG, RVT, Joshua Tanguay, LAT, Diana H. Peroni, CIH, Janeko Bower
Genentech, Inc., 1 DNA Way, South San Francisco, CA 94080
METHODS
An initial surgical procedure was conducted to
obtain baseline waste gas recovery values. The
surgical workstation consisted of a non-externally
vented Class II A2 biosafety cabinet, portable
anesthesia system, and a passive gas scavenging
system. The average room air exchange rate was
~20 changes/hour. Mice were induced in 2 L hinged
induction chambers using isoflurane in oxygen (1
L/min) delivered via a precision vaporizer (set at
2.5%). Surgeries were performed while anesthesia
was maintained via non-rebreathing circuits. WAG
was passively scavenged through activated
charcoal canister filters. Air sampling for isoflurane
was conducted using ChemDisk™ 574 halogenated
anesthetic gas monitors. The monitor sampled
workplace air by diffusion of halogenated anesthetic
gases. These gases are collected on the media via
adsorption. Three personnel monitor samples were
used to detect for possible contamination. These
samples were closed upon conclusion of isoflurane
use, with start and end times recorded and sent to
Assay Technology for analysis. Monitoring sessions
were repeated as new engineering controls were
implemented.
ACKNOWLEDGEMENTS
•Genentech Environmental Health and Safety
•Genentech Laboratory Animal Resources
•Genentech In Vivo Pharmacology Research Staff
•VetEquip, Inc.
DISCUSSION (Cont’d.)
In the initial setup, there are three main areas of
concern where WAG can escape the anesthetic
system:
•When opening the hinged-lid induction chamber.
•Face/port interface of non-rebreathing circuit.
•Passive scavenging via charcoal canisters.
By upgrading components to an active waste gas
scavenging system, WAG exposure levels were
minimized addressing employee safety needs.
Below is the refined surgical setup.
SUMMARY AND CONCLUSIONS
Based on our results, an anesthetic system with
usage of proper engineering controls can:
• Minimize WAG exposure levels during surgical
procedures.
• Help reduce health risks associated with low-
level exposure to WAG.
Reducing WAG leakage may also contribute to:
• Improved animal induction times.
• Improved maintenance of surgical plane.
• Overall decrease in procedure duration.
Results from our monitoring efforts have led to
investment of necessary equipment to limit
isoflurane waste gas exposure to in vivo staff.
INTRODUCTION
Isoflurane is a common inhalation anesthetic agent
used in laboratory animal science and veterinary
clinics. The release and exposure of waste anesthetic
gas (WAG) in the work environment is an occupational
hazard for staff working with this agent. Chronic, low-
level exposure to WAG has been linked to increased
incidences of neurologic and reproductive
dysfunction, hepatic and renal toxicity, and neoplasia1
.
The Environmental Health and Safety team monitored
anesthetic procedures to assess isoflurane waste gas
exposure to in vivo research personnel and to address
methods of reducing these levels. Through a series of
large-scale mouse surgical procedures, industrial
hygiene monitoring was conducted to characterize
WAG exposure among the surgical staff.
MATERIALS
•Hinged-lid Induction •Mapelson E Circuit • Activated
Chamber Charcoal Canister
•Sliding-lid Induction •FilterMate™ Exhaust •ChemDisk™
547
Chamber
DISCUSSION
The major contributing factor to anesthetic
pollution is inadequate scavenging of WAG. Our
initial surgical setup using passive waste gas
scavenging via activated charcoal canisters within
a non-externally vented biosafety cabinet yielded
higher than recommended PEL.
Below is the initial surgical setup highlighting areas of
WAG leakage.
REFERENCES
1.Smith, J. C. & Bolon, B. (2003). Comparison of Three Commercially Available
Activated Charcoal Canisters for Passive Scavenging of Waste Isoflurane during
Conventional Rodent Anesthesia. JAALAS, 42(2), 10-15.
2.Smith, J. C. & Bolon, B. (2006). Isoflurane leakage from non-rebreathing rodent
anesthesia circuits: comparison of emissions from conventional and modified
ports. Laboratory Animals, 40, 200-209.
3.DHHS (NIOSH) Publication Number 77-140, March 1977. Occupational
Exposure to Waste Anesthetic Gases and Vapors, pages 29-35, 107-108.
#P125
Non-rebreathing Circuits
Hinged-lid Induction Chambers
Activated Charcoal Canisters
FilterMate™ Exhaust
Non-rebreathing circuits
with finger cots
Sliding-lid induction chambers
connected to FilterMate™
Circuit tubing connected
to exhaust via collector
Surgery Surgeon #1 Surgeon #2 Surgeon #3 Avg. Notes
1 1.5 NA 1.3 1.4 Non-externally vented biosafety cabinet
2 0.73 0.63 0.63 0.66 Externally vented biosafety cabinet
3 0.11 0.16 <0.1 0.12 Externally vented Hood + Active scavenging system
Results are an 8-hour TWA, ppm