
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Antacid 1
Similar to Antacid 1 (20)
More from Dipali Kulkarni
More from Dipali Kulkarni (20)
Recently uploaded
Recently uploaded (20)
Antacid 1
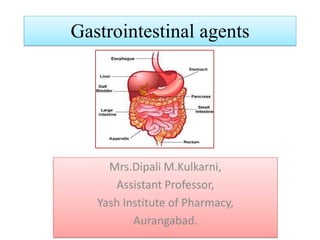
- 1. Gastrointestinal agents Mrs.Dipali M.Kulkarni, Assistant Professor, Yash Institute of Pharmacy, Aurangabad.
- 2. Gastrointestinal agents Acidifiers: Ammonium chloride* Dil. HCl Antacid: Ideal properties of antacids, combinations of antacids, Sodium 40 Bicarbonate*, Aluminum hydroxide gel, Magnesium hydroxide mixture Cathartics: Magnesium sulphate, Sodium orthophosphate, Kaolin Bentonite
- 3. Gastro intestinal agents Product altering gastric pH Acidifiers Antacid 2. Protectives for intestinal inflammation 3. Adsorbent for intestinal toxins 4. Cathartics and Laxatives Inorganic agents used to treat gastrointestinal disorder
- 4. ACIDIFERS Patients suffering from ,hypochlorhydria or achlorhydria, there is less or absence of hydrochloric acid in Gastric secretions. In such cases, acidifiers are useful in providing the necessary acidity for the proper digestion of food. Systemic acidifiers are those which, when gives usually by injection, act by reducing the alkali reserve in the body and so are useful in reducing metabolic alkalosis. Ammonium chloride, Calcium chloride, Dilute HCl
- 5. AMMONIUM CHLORIDE Category: Systemic acidifier, expectorant and diuretic Description: Hygroscopic white crystalline powder. Solubility: Soluble in water, alcohol & glycerine •NH4Cl act by stimulating the gastric reflexes (causing irritation by ammonia/amine gas) HCl → H+ + Cl- NH4Cl → NH3 + HCl
- 6. Method of preparation of Ammonium Chloride • Preparation: • Ammonium chloride is made by reacting hydrochloric acid with ammonia the solution is evaporated to dryness and the product is purified by recrystallization. NH3 + HCl → NH4Cl • Doses: it is given 3- 6 g per day in divided doses.
- 7. Indicator- ferric ammonium sulphate A solution acidifies with nitric acid shake with a measured volume of N/10 silver nitrate, Nitrobenzene added It coagulate silver chloride PPT, avoid its interference Titrate with excess of silver nitrate N/10 ammonium thiocynate,. Assay of ammonium chloride A modified Volhard method I.P
- 8. AgNO3 + NH4Cl → AgCl + NH4NO3 AgNO3 + NH4SCN → AgSCN + NH4NO3 Ammonium thiocynate Silver thiocynate • The following is the reaction taking place at the end point when red ferric thiocynate is formed (by reaction of ammonium thiocynate with the indicator ammonium sulphate). FeNH4(SO4)2 +3NH4SCN → Fe(SCN)3 + 2(NH4)2SO4
- 9. It is colour less aqueous solution acidic to litmus. Prepared by mixing 274gm of HCl and 726 gmof purified water (Ref. I.P.). I.P. Limit: It contains not less than 9.5% and not more than 10.5% w/w of HCl. When 5.0ml of dilute HCl is added to 200ml ofwater, it provides about 15 mEq of dil. HCl acid Dilute HCl I.P. Recommended to relieve the patients suffering from achlorhydria
- 10. Method of Analysis: Dil HCl • It is analyzed on the principle of ‘acid-base titration’. • An accurately weighed quantity (4.0g to 6.0g), add 30 ml of distilled water mix , titrate against 1.0 N NaOH Indicator - methyl orange HCl + NaOH → NaCl + H2O Each ml of 1.0 N NaOH solution is equivalent 0.03646g of HCl
- 11. Test for Identification: 1) When added to KMnO4 with dilute nitric acid,chlorine is evolved. 2) Limit test for chloride: To acidified solution add silver nitrate solution, shake and allow to stand, curdy white precipitate is formed, which is insoluble in HNO3, but this ppt soluble after being washed with water in ammonium hydroxide from which it is re-precipitated by the additionof HNO3.
- 12. Dose & Uses • Dose: About 0.6 to 8.0 ml • The acid should be diluted with 25-50 volumes with water or juice and sipped through a glass tube to prevent reaction upon dental enamel. It is taken during or after meals given inconjunction with iron therapy in hyperchromic anemia. • Uses: Acidifier
- 13. Antacids are weak bases • Raise pH to about 4- 7 (NaHCO3) without systemic alkalosis Decrease gastric acidity by neutralizing HCL. Used in hyperchlorhydria to relieve pain (HCH) • Effectiveness of antacids is measured in neutralizing capacity. • HCl secreted by epithelial cell of gastric mucosa, PH of stomach - 1-6. • Gastritis inflammation of gastric mucosa hypersecretion of HCL. • Prolong excessive secretion of HCl- peptic ulcer. • Mucosal layer Erosion- Esophageal ulcer, gastric ulcer, duodenal ulcer Antacids
- 14. Ideal Characteristic of Antacid should not be absorba ble, causes systemic alkalosis should not be laxative or cause constipat ion should exert effect rapidly, over a long period of time should buffer in pH 4-6. should not produce large volume of gas should be palatable , inexpens ive should probably inhibit pepsin
- 15. Antacids are divided into two categories 1.Systemic/Absorbable Antacids, alkalotic agents, systemic alkalisers absorbs from gut into blood circulation, changes pH of the blood and cause systemic alkalosis. in diabetic coma-used by injection to relieve acidosis in the blood. Sodium bicarbonate, Potassium citrate, Sodium citrate Side-effects: Nausea, Vomiting, Diarrhea, Abdominal pain, Headache, Irritability, Insomnia etc Uses: use to combat/maintain acidosis systemic acidbase balance (acid- base equilibrium) of the blood CLASSFICATION OF ANTACIDS
- 16. 2.Non-systemic Antacids: local antacids Neutralize acid in stomach, relives gastric and duodenal ulcers. a) Aluminium hydroxide gel B) Dried aluminium hydroxide gel c) Aluminium phosphate d) Magnesium hydroxide e) Magnesium trisilicate f) Light and heavy magnesium carbonate g) Magaldrate h) Calcium carbonate. i)Bismulth suberarbonate.
- 17. • Insoluble in water • Absorption rate is less due to their cationic nature • No direct effect upon the systemic acid base Balance (acid-base equilibrium) of the blood • E.g. Aluminum hydroxide and Magnesium hydroxide & Mg trisilicate • Uses: in the treatment of peptic ulcer & hyperacidity Properties of non systemic antacids
- 18. Thank you