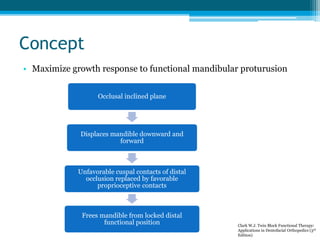
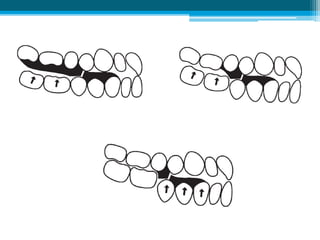
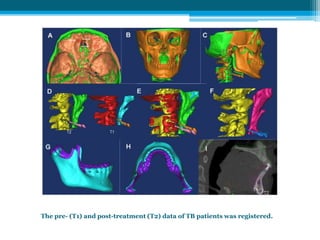
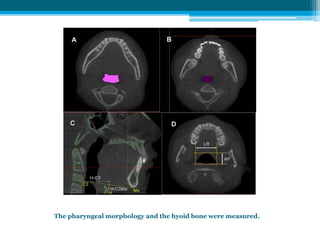
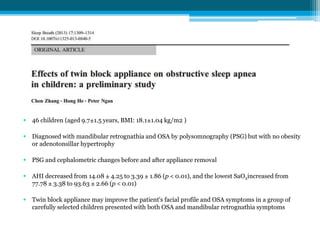
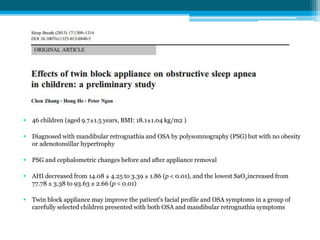


The document discusses the Twin Block appliance, developed by William Clark in 1977, for treating Class II Division 1 malocclusion by positioning the mandible forward to promote growth. It outlines the design features, applications, bite registration methods, and patient instructions for use, emphasizing the importance of full-time wear for effectiveness. Additionally, it presents findings from studies indicating improvements in airway and facial profile for children treated with the appliance.































![Bionator[1]](https://cdn.slidesharecdn.com/ss_thumbnails/bionator1-110611105906-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)
![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)








