Peptic ulcer
•Download as PPTX, PDF•
2 likes•294 views

disease of the gastrointestinal tract

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (18)
Similar to Peptic ulcer
Similar to Peptic ulcer (20)
More from Ruben Gombalandi
More from Ruben Gombalandi (13)
Recently uploaded
Recently uploaded (20)
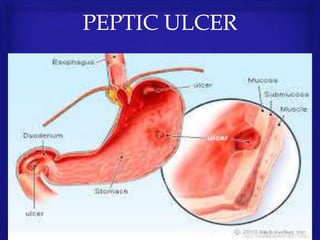
Peptic ulcer
- 3. A problem with the gastrointestinal tract characterized by mucosal damage secondary to pepsin and gastric acid secretion. Contrary to general belief, more peptic ulcers arises in the duodenum than in the stomach.
- 4. CLASSIFICATION According to Localisation. Stomach –gastric ulcers. Duodenum-duodenal ulcers. Oesophagus- oasophageal ulcers. According to Phase of Disease. Acute Uncomplete remission. Remission. Association with H.Pylori o H.Pylori Associated. o H.Pylori Not Associated.
- 5. Etiology. Helicobacter Bacteria. Drugs – NSAIDS,Corticosteroids. Hyperacidity eg,Zollingers Ellison . Lifestyle risks include smoking,Alcohol and dietary factors . Heredity . Association with other diseases or known factors.
- 6. The main symptoms of PUD: Recurrent Abdominal pain: localization (epigastrium) and radiation, character (episodic occurrence), permanent or seasonal relationship to food (early, late, nocturnal, hunger). Dyspepsia: (vomiting, nausea, heartburn) Relieving factors (taking food or soda, spasmolytics, warmly) Possible clinical features (weight loss, fever, anorexia, dysphagia). Clinical symptoms of PUD: - Tender palpation of the abdomen: local pain (tenderness) - Local muscular resistance - Mendel’s symptom in epigastrium or duodenum bulb projection point in percussion Auscultation of the abdomen: gastric’s down border, If the initial clinical presentation suggests the diagnosis of PUD, the patient should be evaluated for alarm symptoms. Anemia, hematemesis, melena, or heme-positive stool suggests bleeding; vomiting suggests obstruction; anorexia or weight loss suggests cancer; persisting upper abdominal pain radiating to the back suggests penetration; and severe, spreading upper abdominal pain suggests perforation. Patients older than 55 years and those with alarm symptoms should be referred for prompt upper endoscopy.
- 7. INVESTIGATION. Lab Studies Obtain a CBC. Check the hemoglobin and hematocrit - anemia. Obtain an electrolyte panel - identifying and correcting electrolyte abnormalities Liver function tests may be helpful, when a malignant etiology is suspected. A test for H pylori is helpful when the diagnosis of PUD is suspected Imaging Studies Plain abdominal radiographs, contrast upper GI studies (Gastrografin or barium), and CT scans with oral contrast are helpful. Plain radiographs, including the obstruction series (ie, supine abdomen, upright abdomen, chest posteroanterior), can demonstrate the presence of gastric dilatation and may be helpful in distinguishing the differential diagnosis. Diagnostic Procedures Upper endoscopy can help visualize the gastric outlet and may provide a tissue diagnosis when the obstruction is intraluminal. The sodium chloride load test is a traditional clinical nonimaging study that may be helpful. The traditional sodium chloride load test is performed by infusing 750 cc of sodium chloride solution into the stomach via a nasogastric tube (NGT). A diagnosis of GOO is made if more than 400 cc remain in the stomach after 30 minutes.
- 8. Tests Used in the Diagnosis of Peptic Ulcer Test Comments EGD ______________________ Indicated in patients with evidence of bleeding, weight loss, chronicity, or persistent vomiting; those whose symptoms do not respond to medications; and those older than 55 years More than 90 % sensitivity and specificity in diagnosing gastric and duodenal ulcers and cancers Barium or Gastrografin contrast radiography (double-contrast hypotonic duodenography) Indicated when endoscopy is unsuitable or not feasible, or if complications such as gastric outlet obstruction suspected Diagnostic accuracy increases with extent of disease; 80 to 90 % sensitivity in detecting duodenal ulcers Helicobacter pylori testing Serologic ELISA _____________________ Useful only for initial testing (sensitivity, 85 %; specificity, 79 %); cannot be used to confirm eradication Urea breath test ______________________ More expensive, Sensitivity, 95 to 100 %; specificity, 91 to 98 %; can be used to confirm eradication PPI therapy should be stopped for 2 weeks before test Stool antigen test ______________________ Inconvenient but accurate (sensitivity 91 to 98 %; specificity 94 to 99%), Can be used to confirm eradication Urine-based ELISA and rapid urine test Sensitivity, 70 to 96 %; specificity, 77 to 85 % Cannot be used to confirm eradication Endoscopic biopsy Culture (sensitivity, 70 to 80 %; specificity, 100 %), histology (sensitivity, > 95 %; specificity, 100 %), rapid urease (CLO) test (sensitivity, 93 to 97 %; specificity, 100 %) EGD = esophagogastroduodenoscopy; ELISA= enzyme-linked immunosorbent assay; PPI= proton pump inhibitor; CLO= Campylobacter-like organism.
- 9. Treatment. 1. Antisecretory drugs • Proton pump inhibitors :Omeprazole(20mg) Lansoprazole(30 mg) Pantoprazole( 40mg) Rabeprazole (20mg) ..all once a day. H2 receptor antagonists : Cimetidine, Famotidine, Nizatidine ,Rantidine • Antacids :Amagel,Maalox. 2. Antibiotics :Clarithromycin,Amoxycillini. 3. Cytoprotective agents : Misoprostol, Sucralfate . 4. Diet- it is common sense approach to avoid any foods and beverages that aggravate the symptoms alcohol included.
- 10. Complications. Perforation - Involuntary guarding is indicative of peritonitis secondary to gastric perforation. Penetration – is type of the closed Perforation Hemorrhage – Upper gastrointestinal bleeding (UGIB) is a common medical condition that results in high patient mortality and medical care costs. Obstruction - Gastric outlet obstruction (GOO) is not a single entity; it is the clinical and pathophysiological consequence of any disease process that produces a mechanical impediment to gastric emptying.