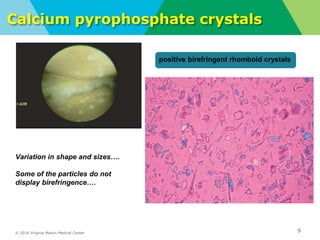
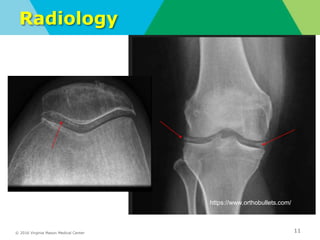
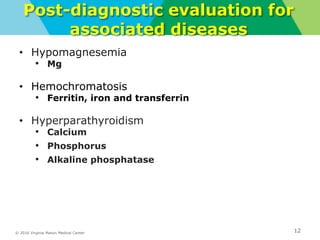
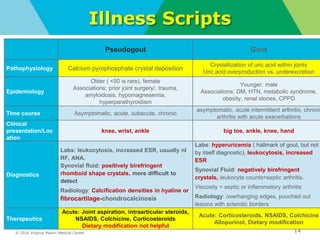
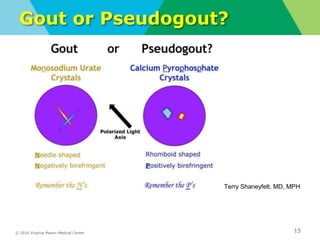
This document summarizes a noon conference presentation on pseudogout (calcium pyrophosphate crystal deposition disease). The presentation discusses the clinical presentation of pseudogout including acute attacks characterized by intense pain and swelling typically in the knees. Diagnosis involves identification of positively birefringent calcium pyrophosphate crystals in synovial fluid or tissue. Treatment depends on the number of affected joints, ranging from joint aspiration and steroid injection for one or two joints to NSAIDs and colchicine for more extensive involvement. The presentation also provides an illness script comparing pseudogout to gout and reviews associated conditions requiring further evaluation.












































![2019 04-30 noon conference [stephen slade]](https://cdn.slidesharecdn.com/ss_thumbnails/2019-04-30noonconferencestephenslade-190501212611-thumbnail.jpg?width=640&height=640&fit=bounds)


























