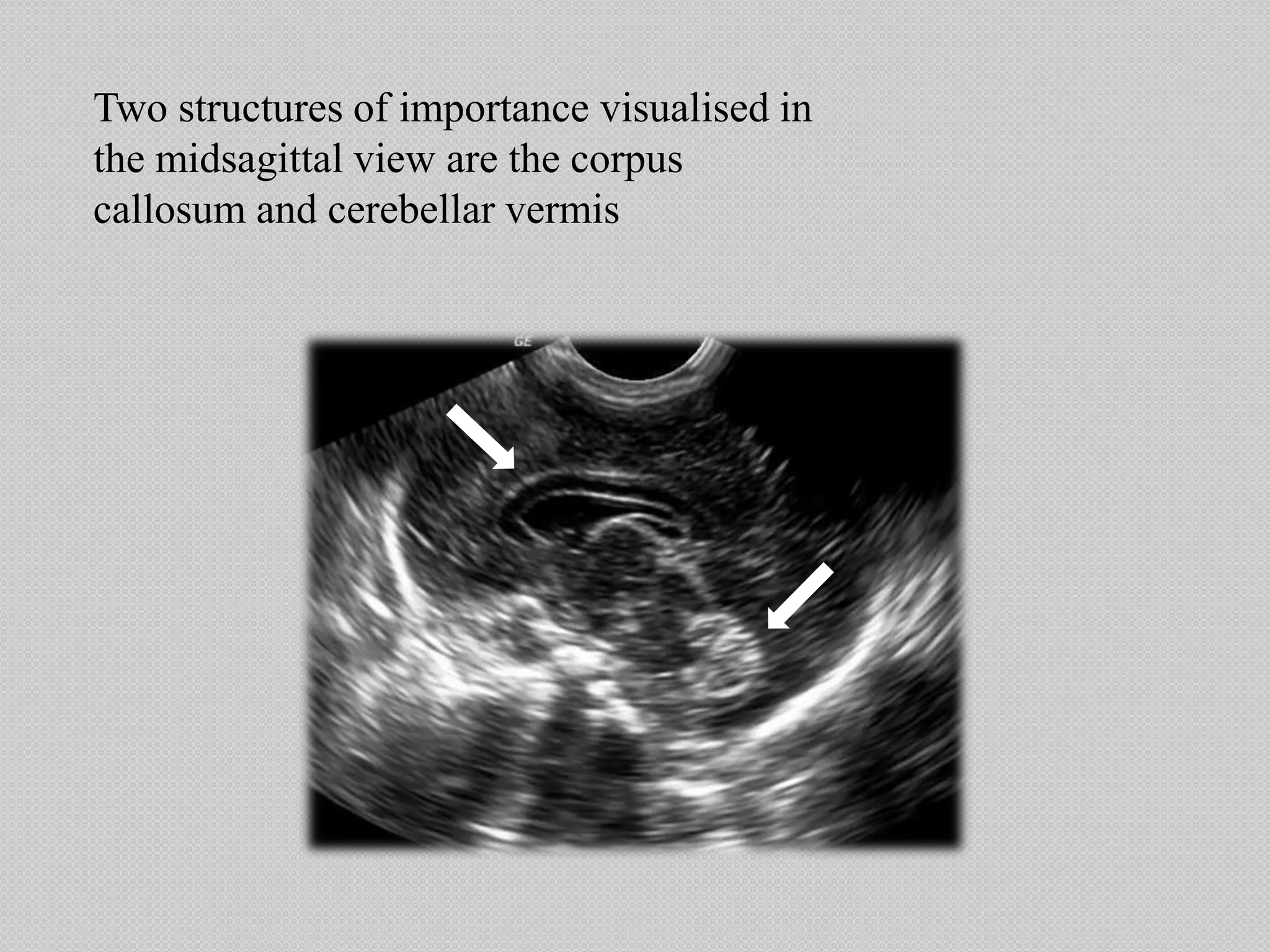
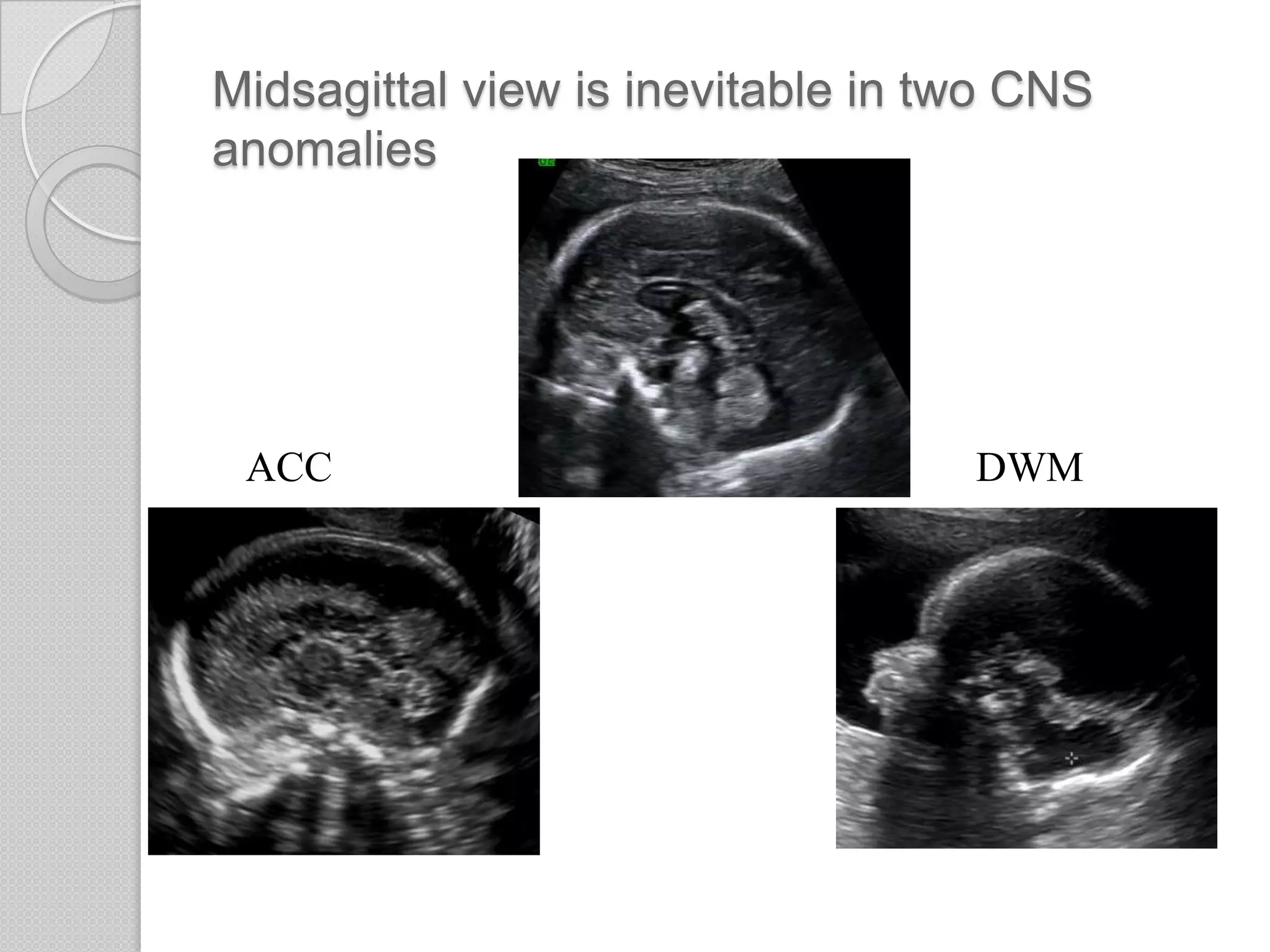
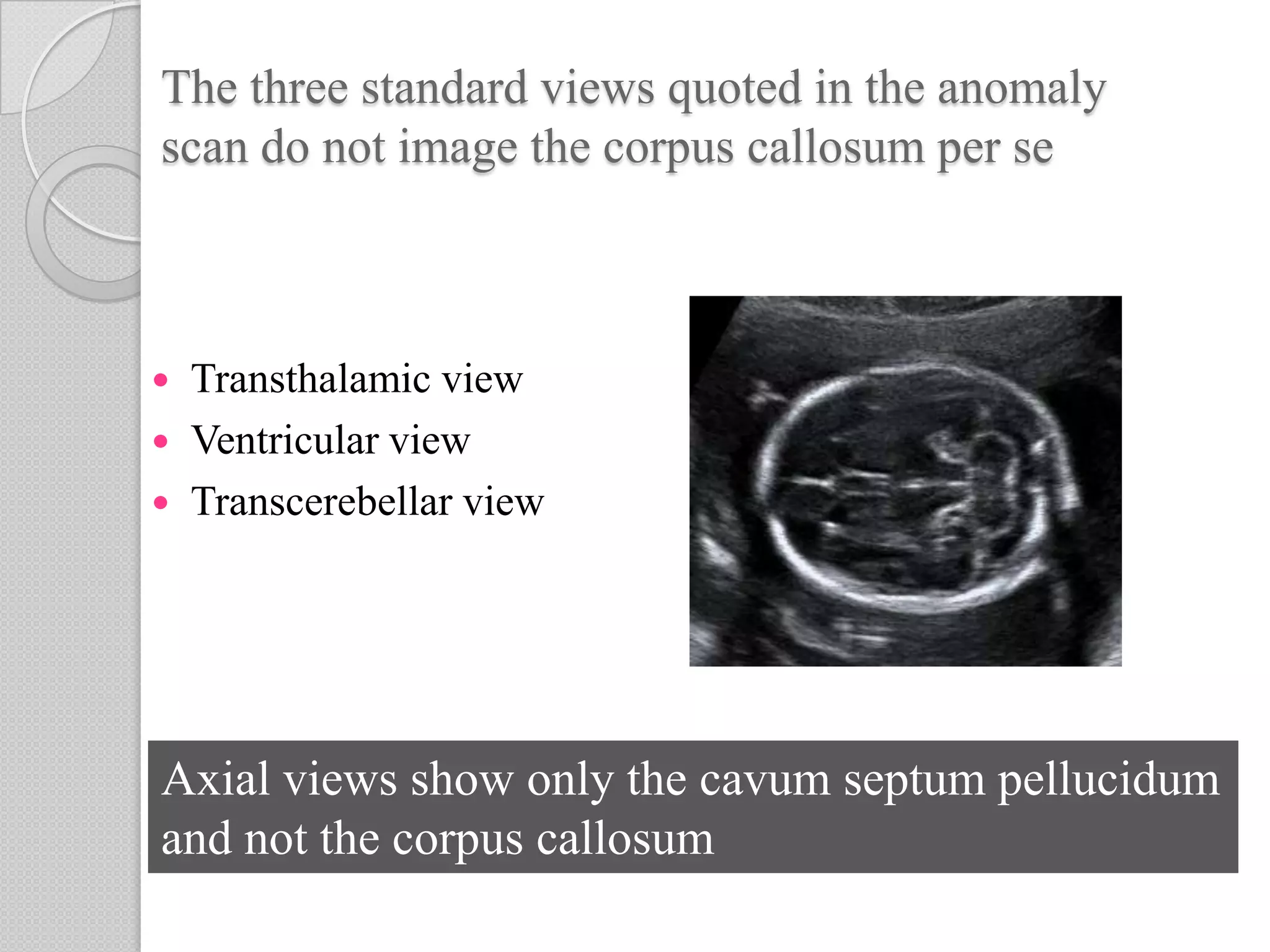
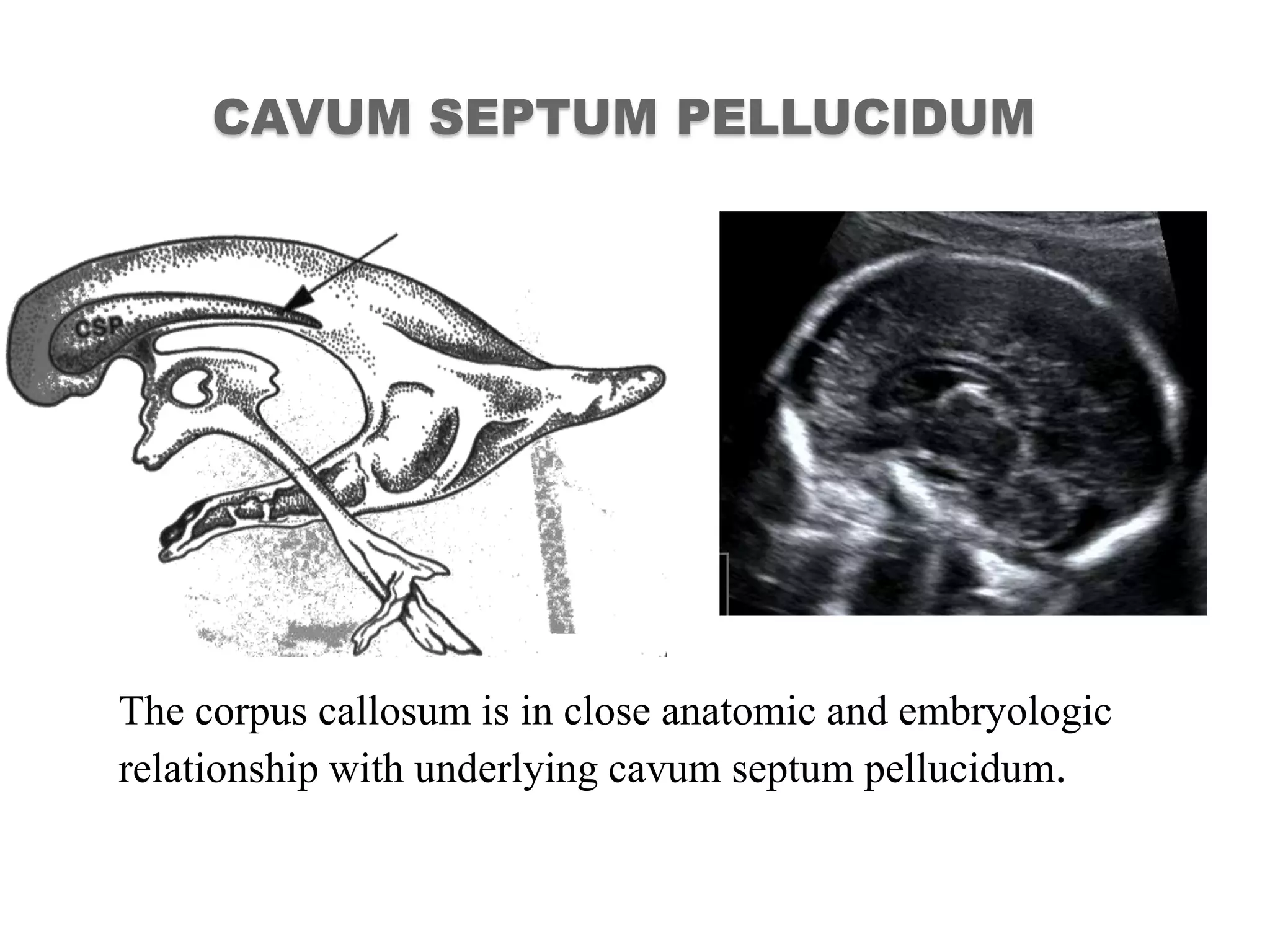
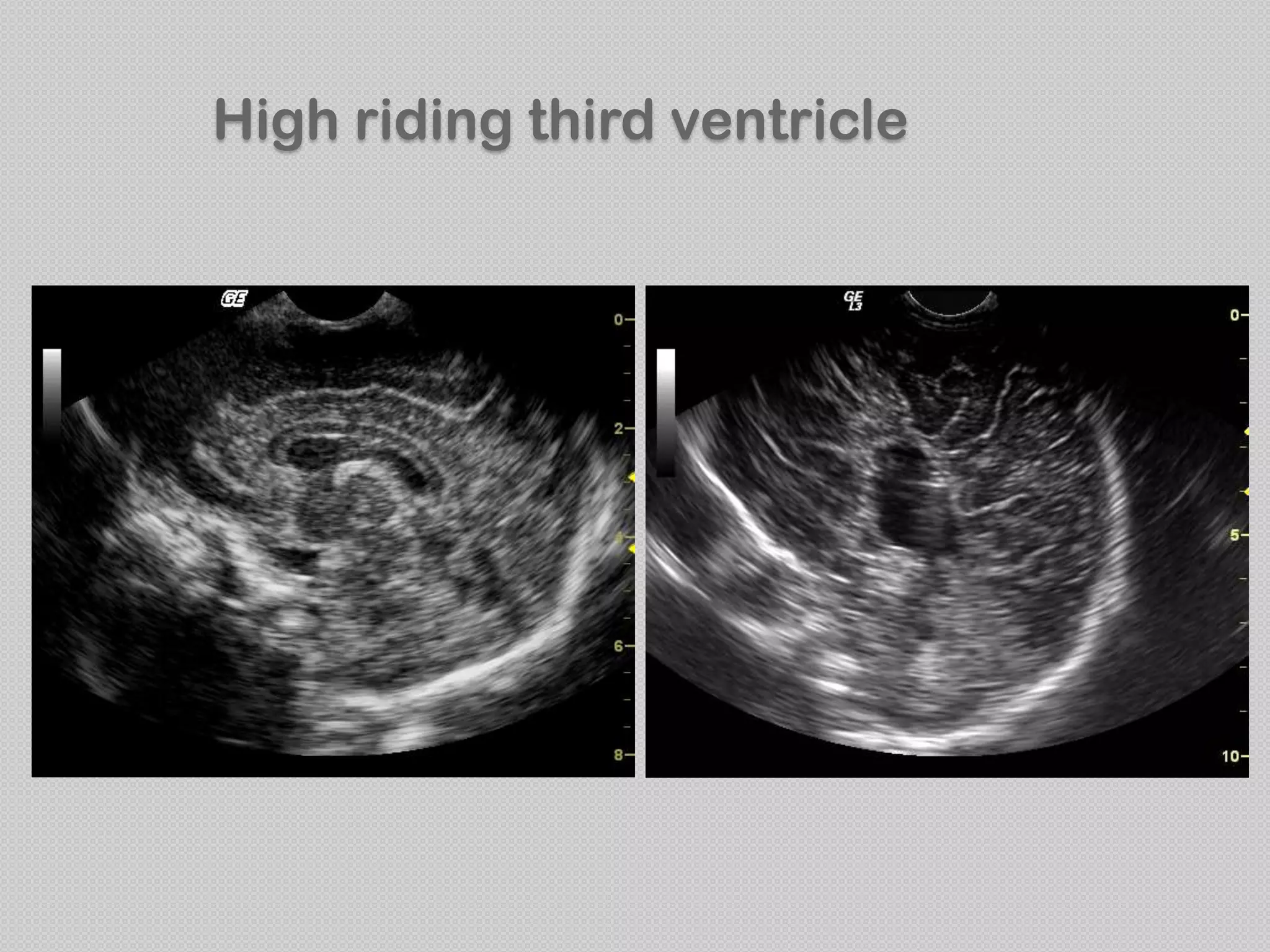
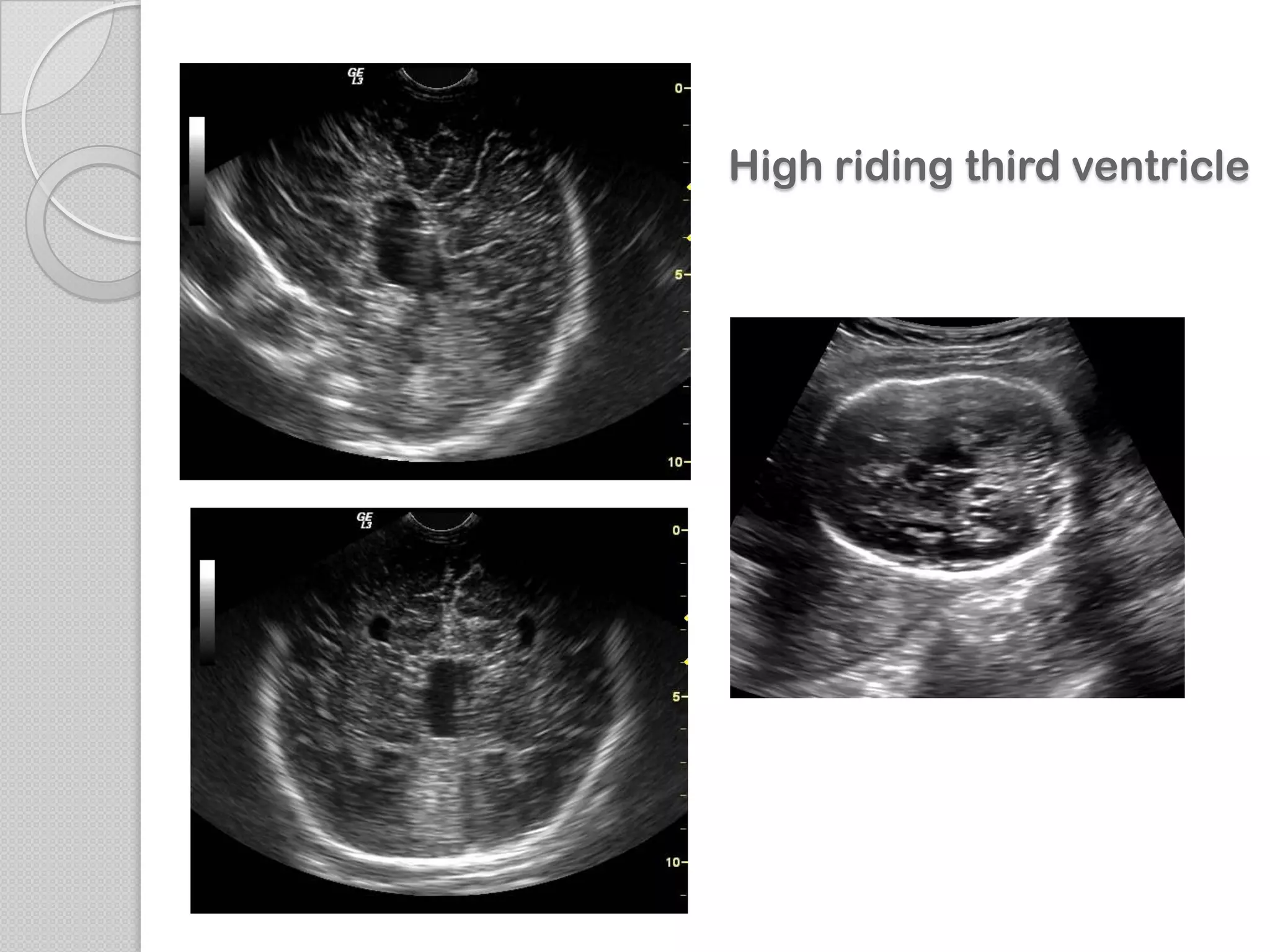
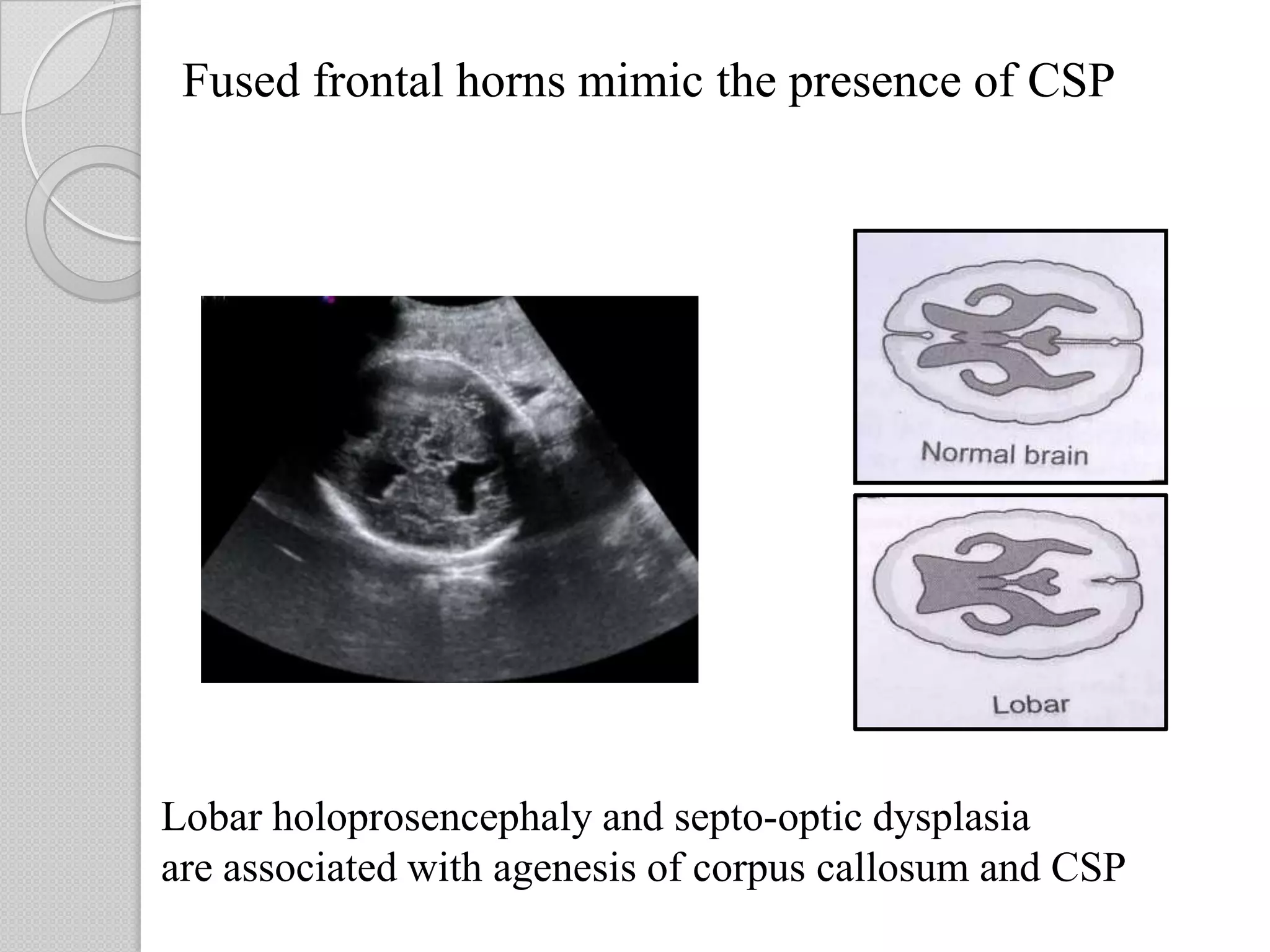
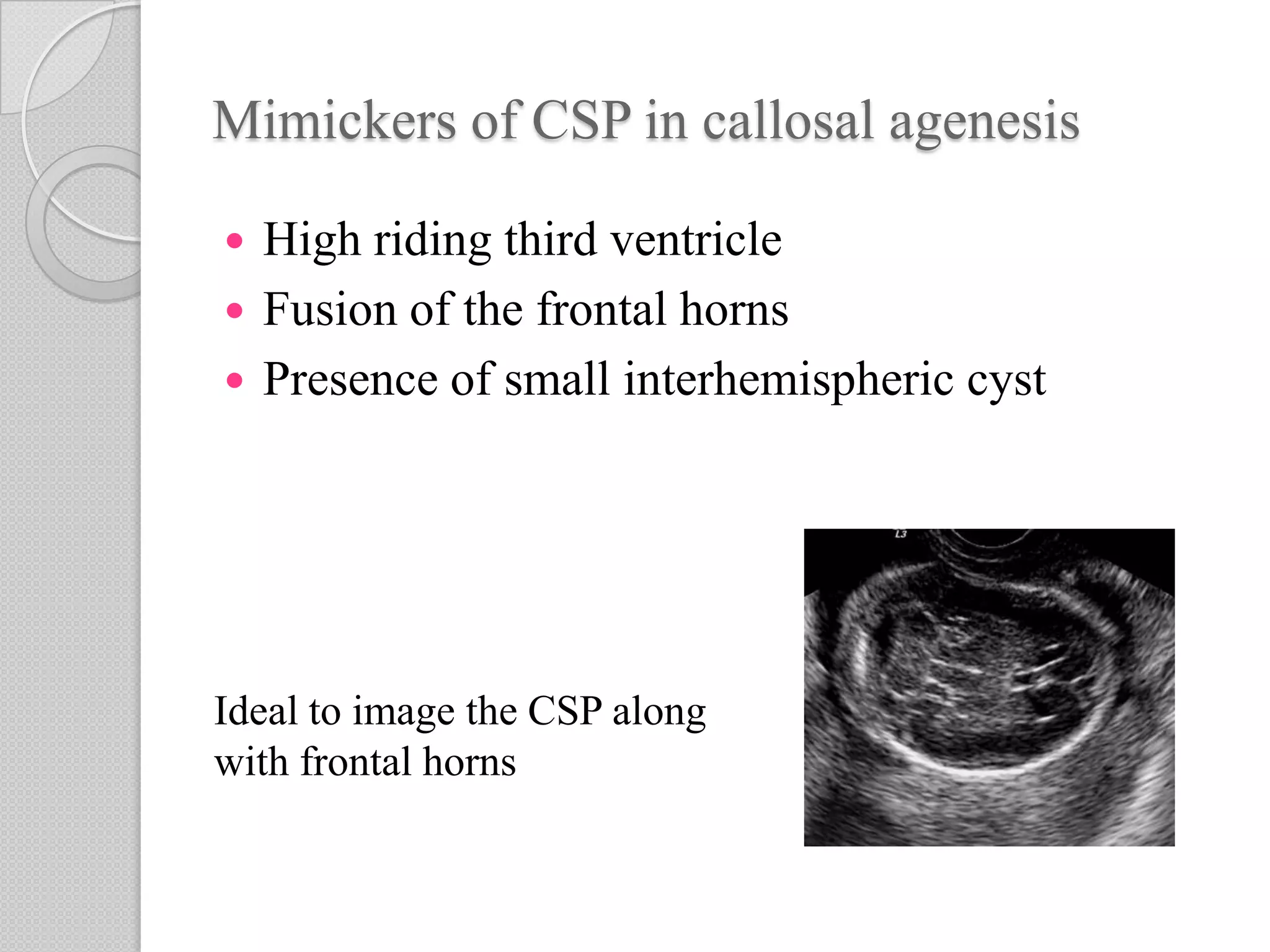
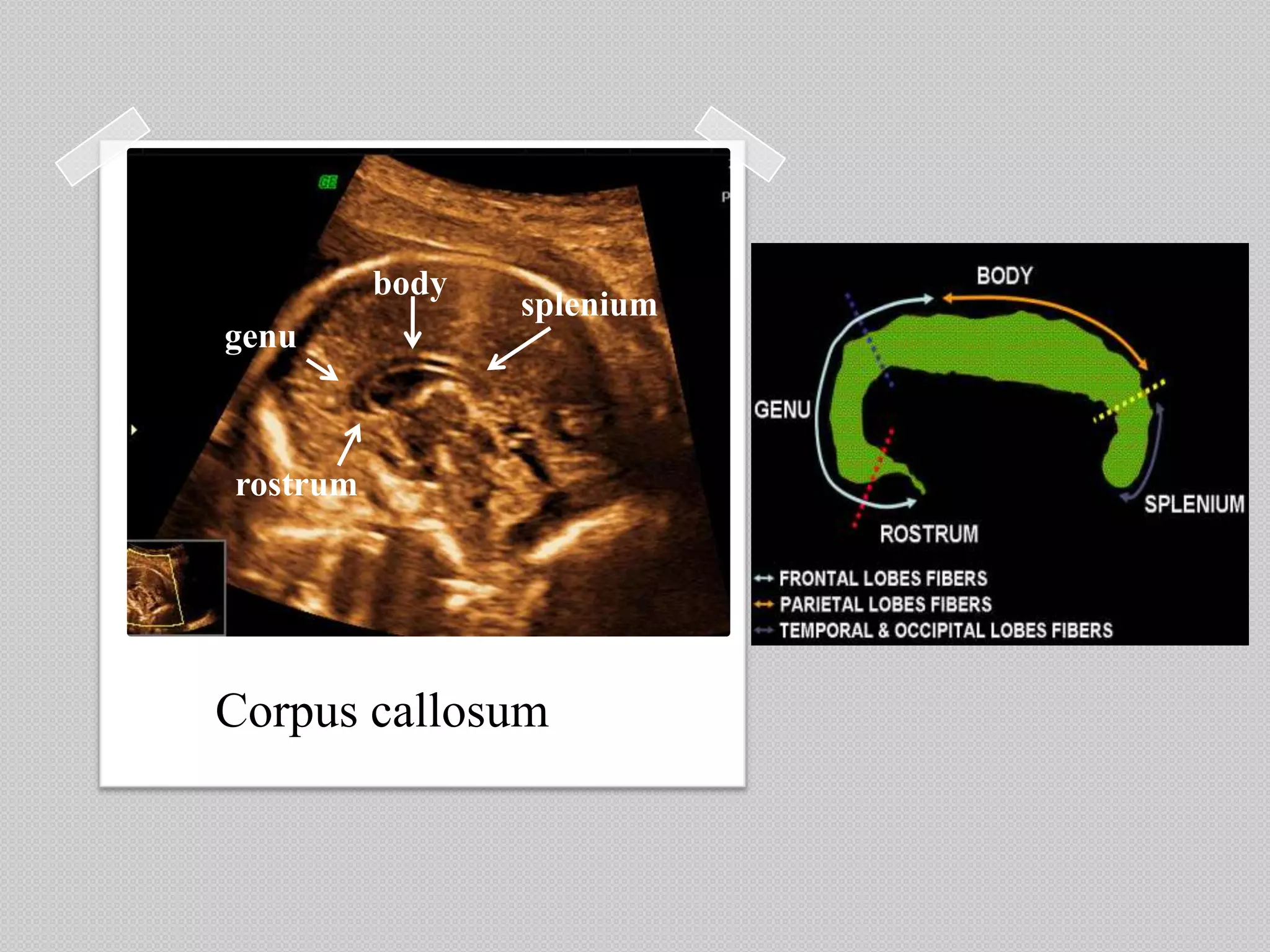
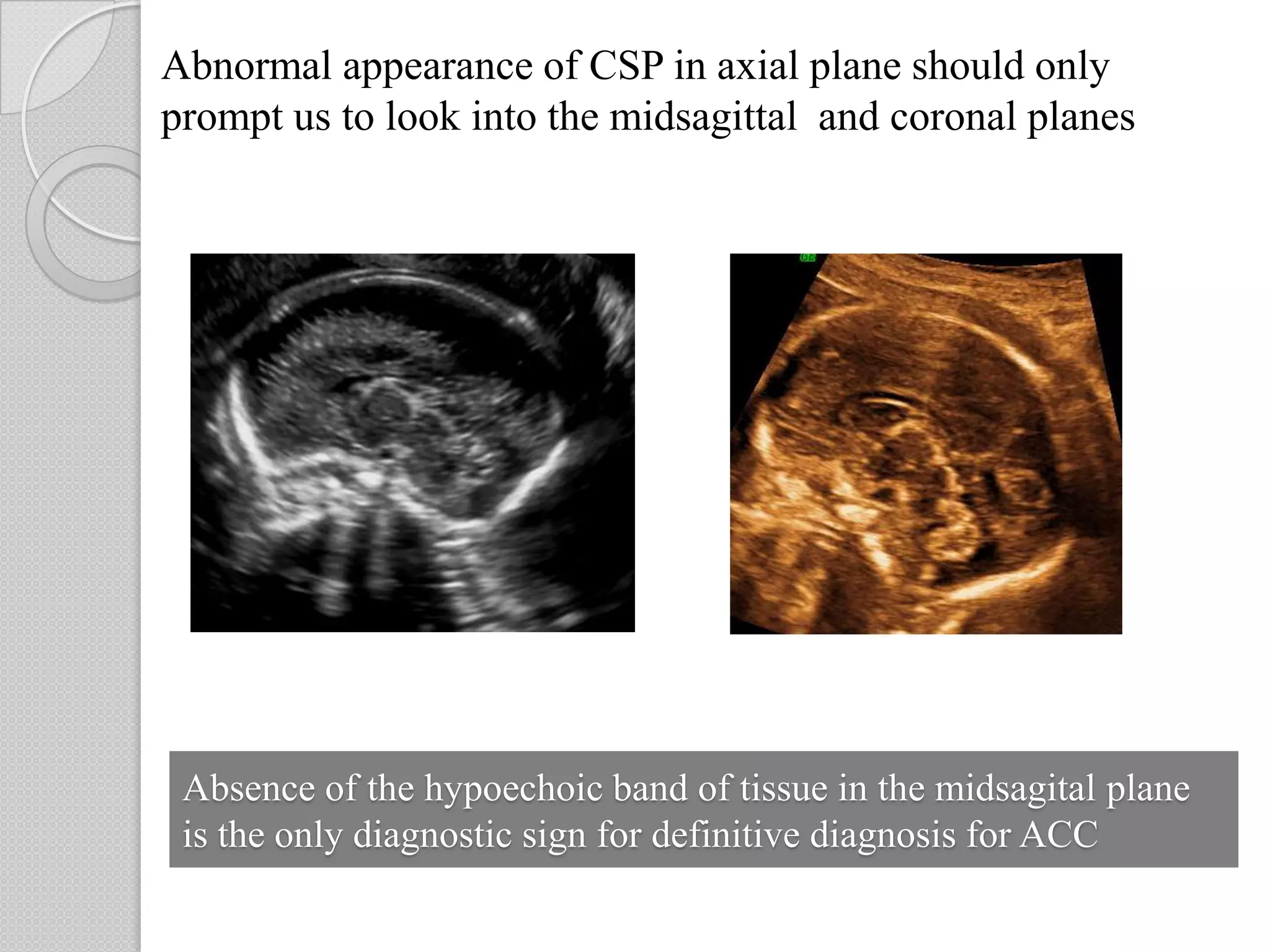
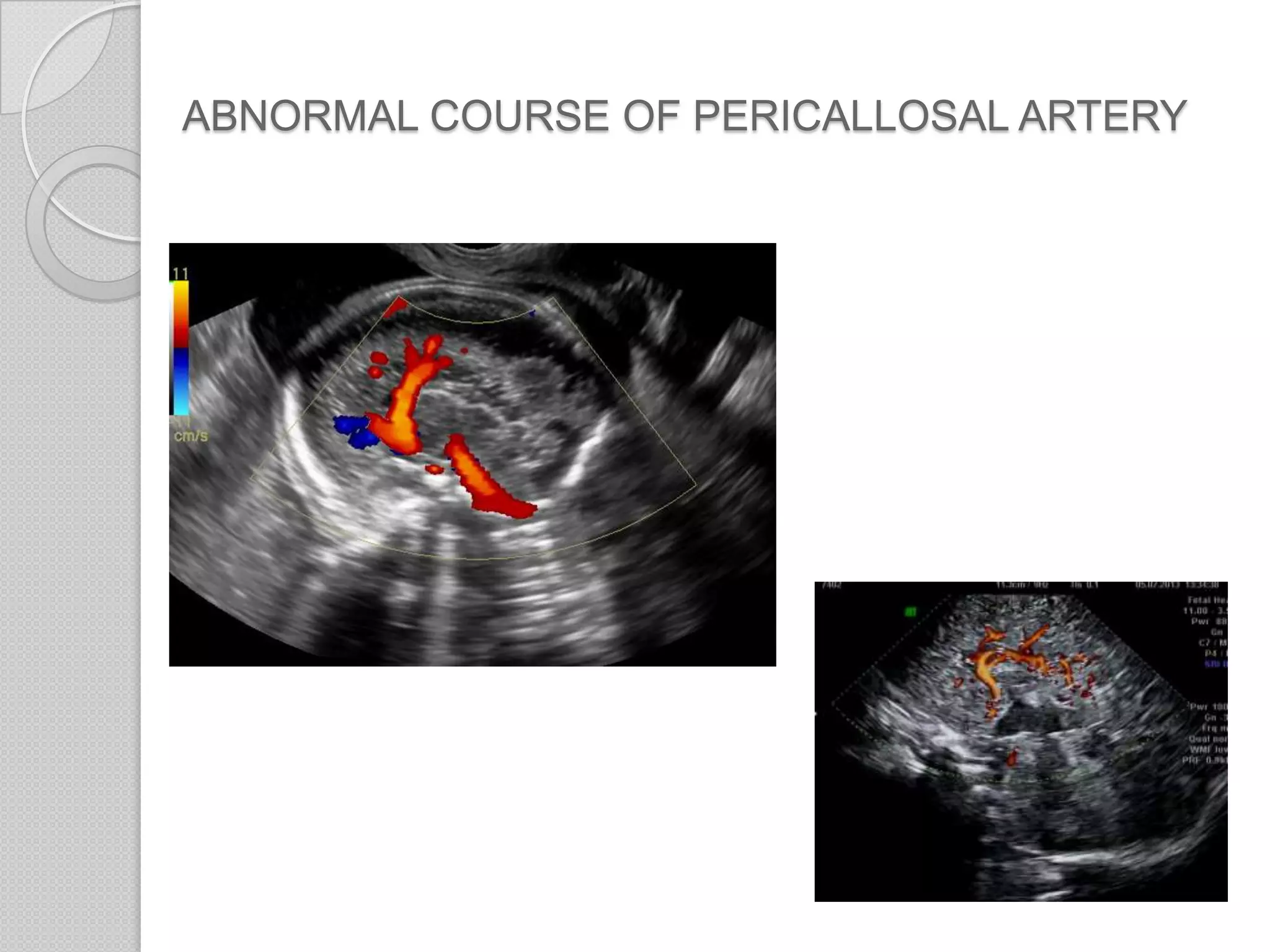
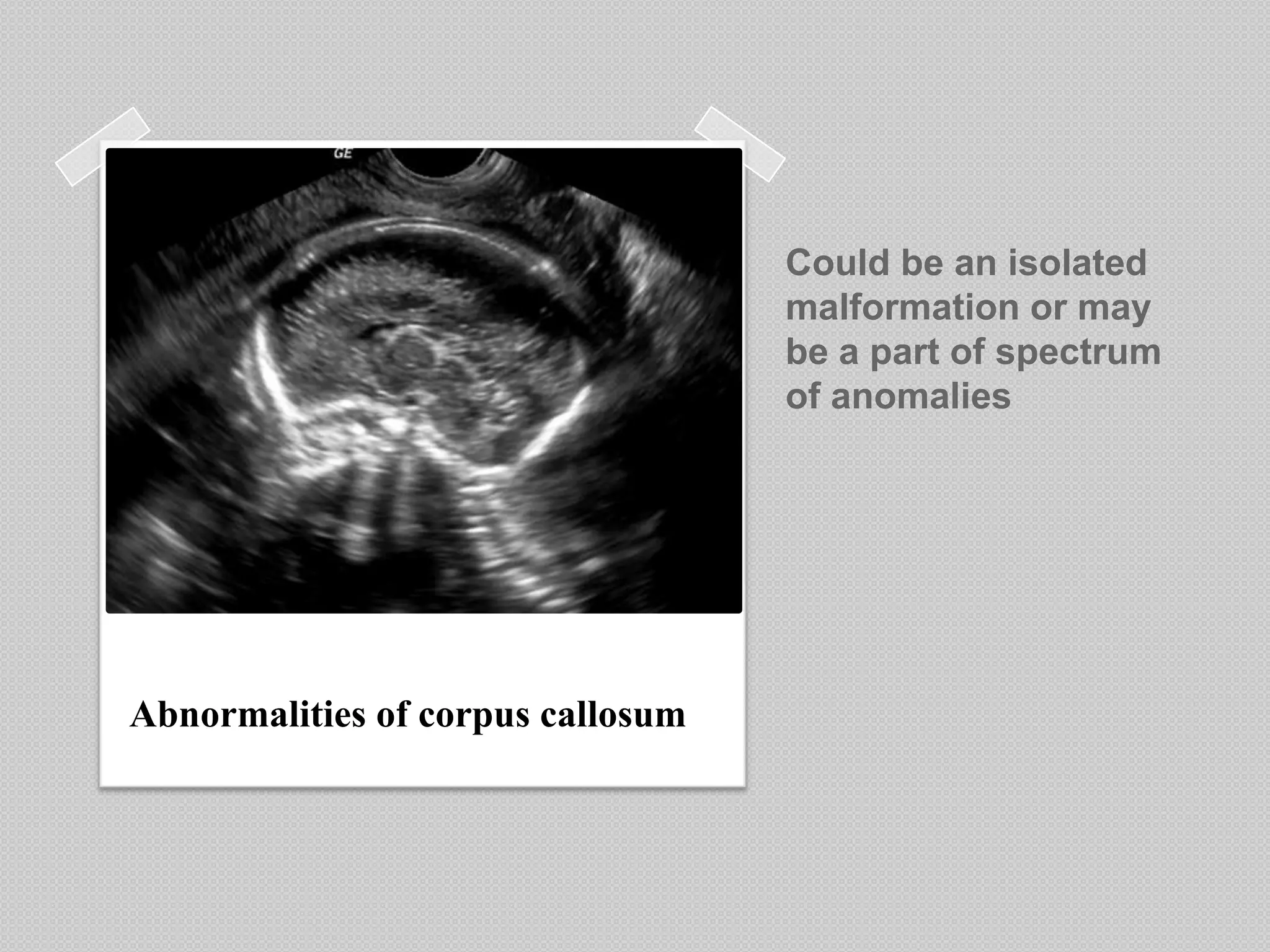
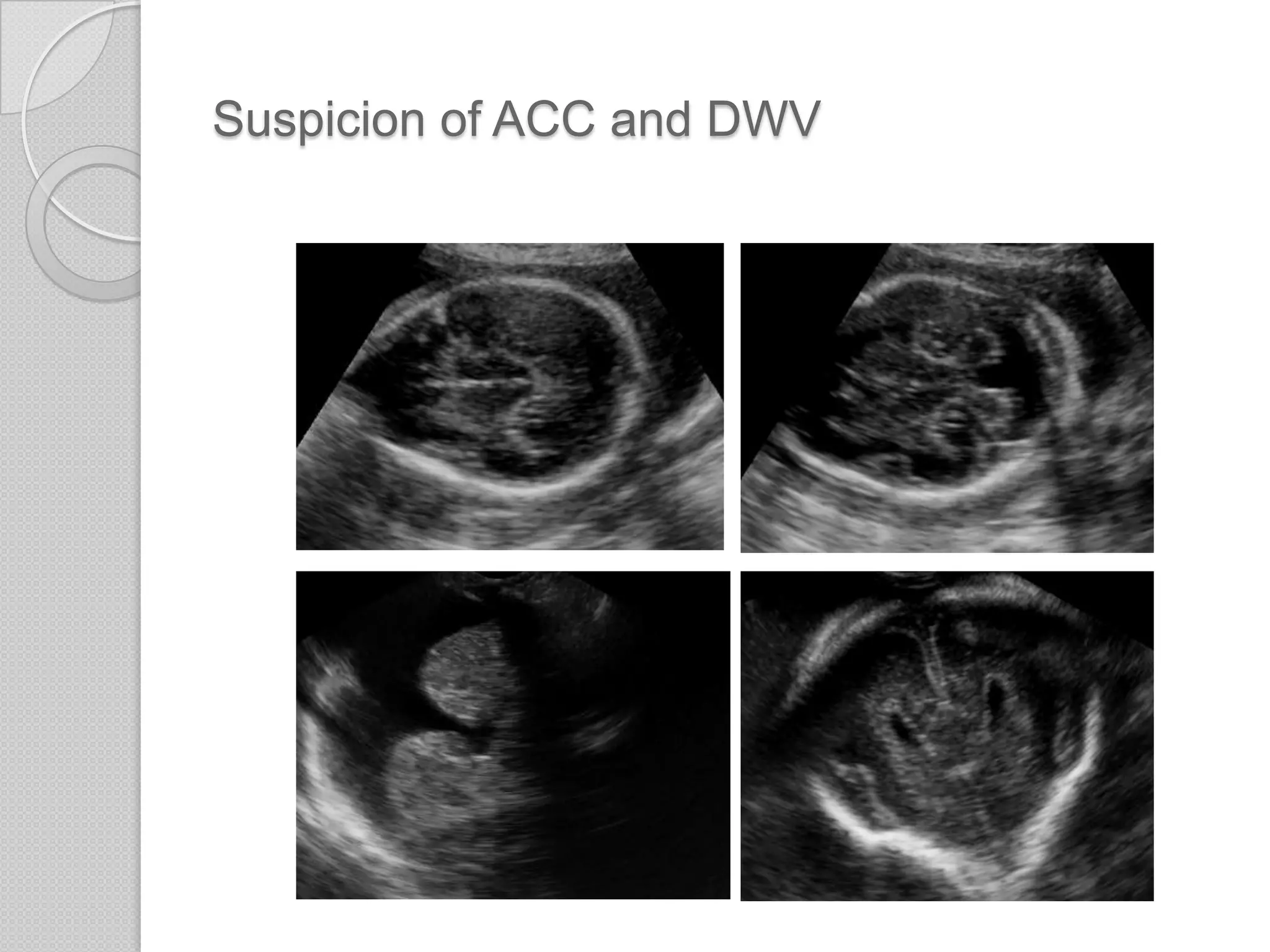
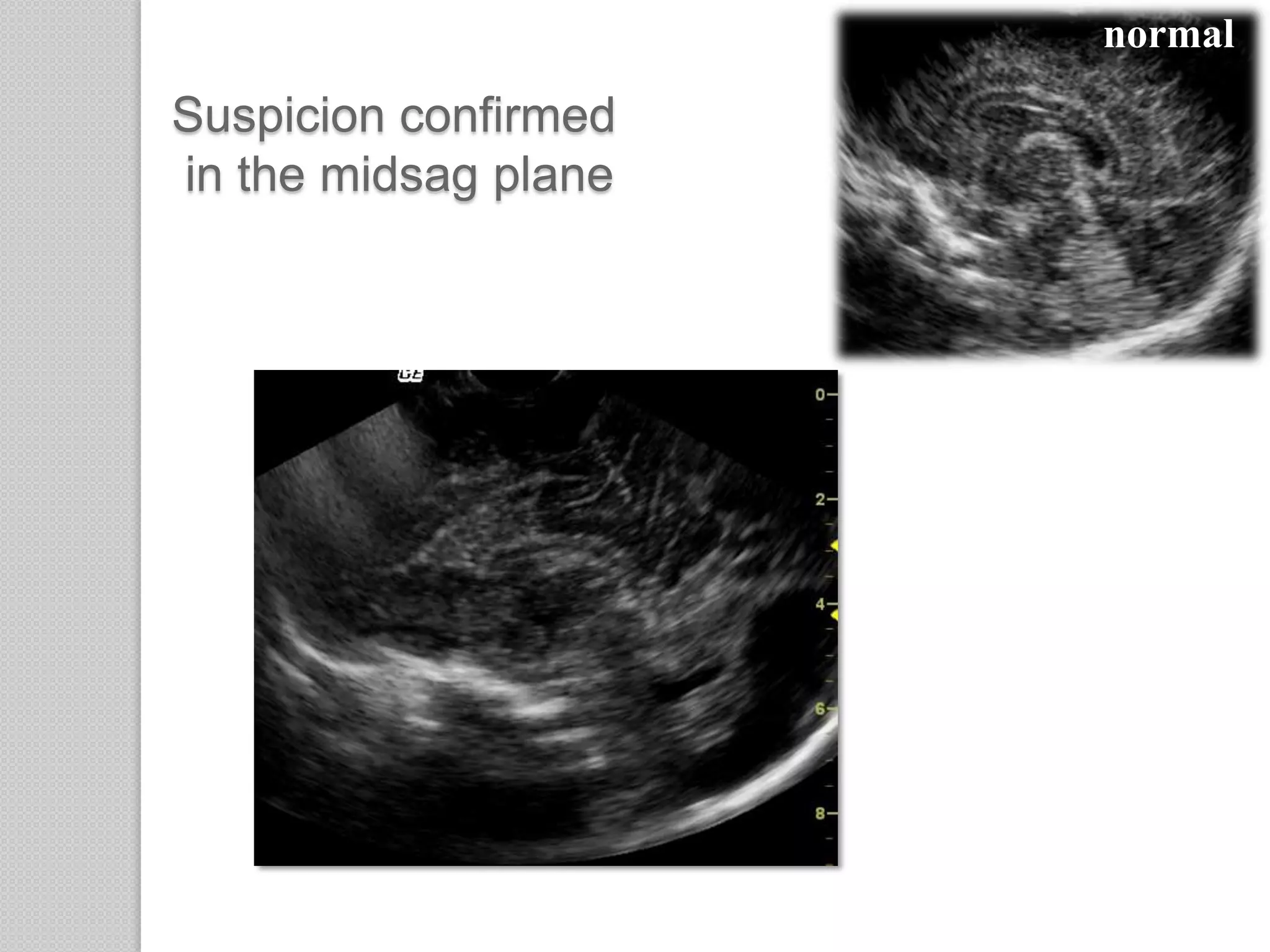
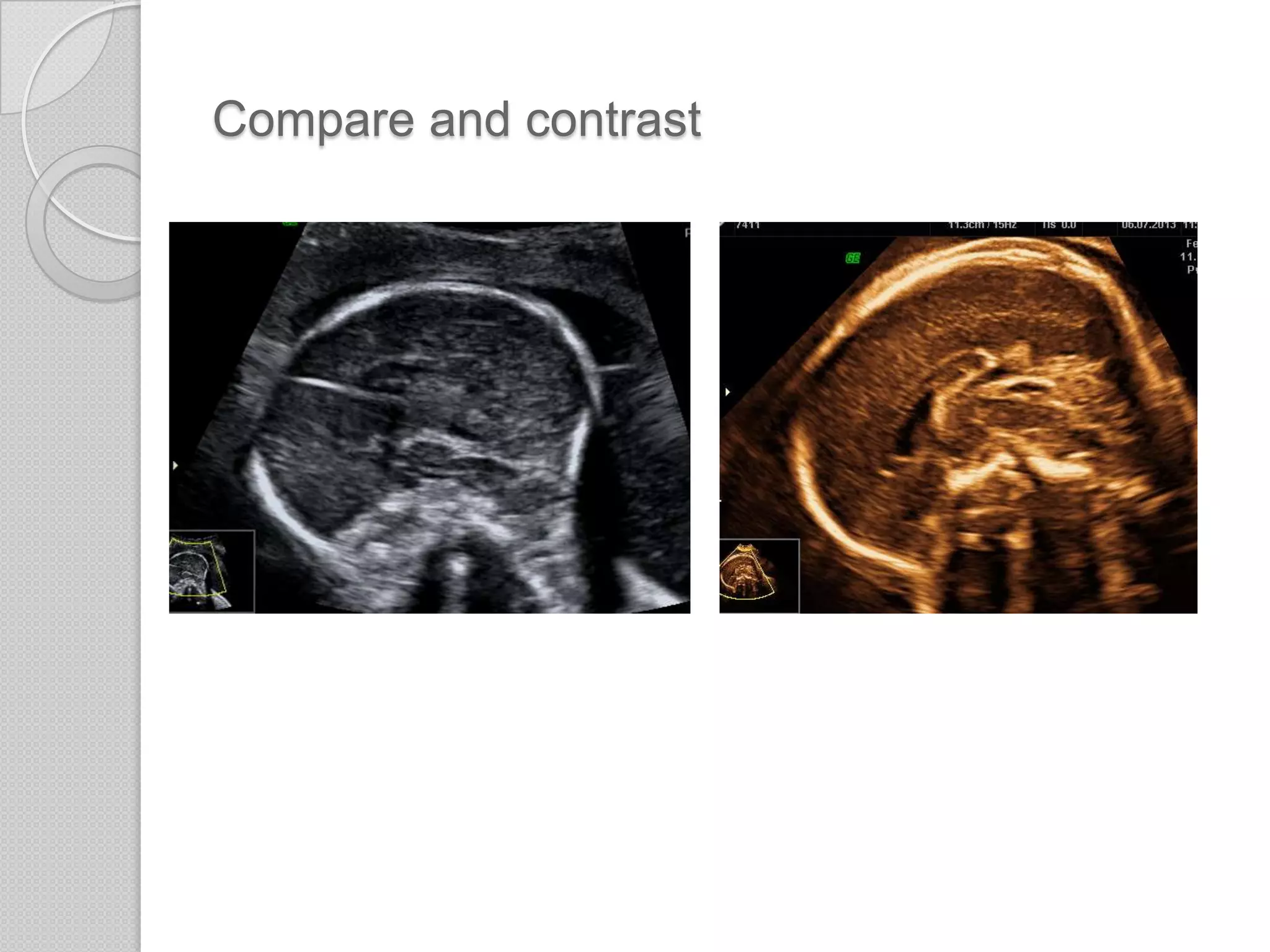
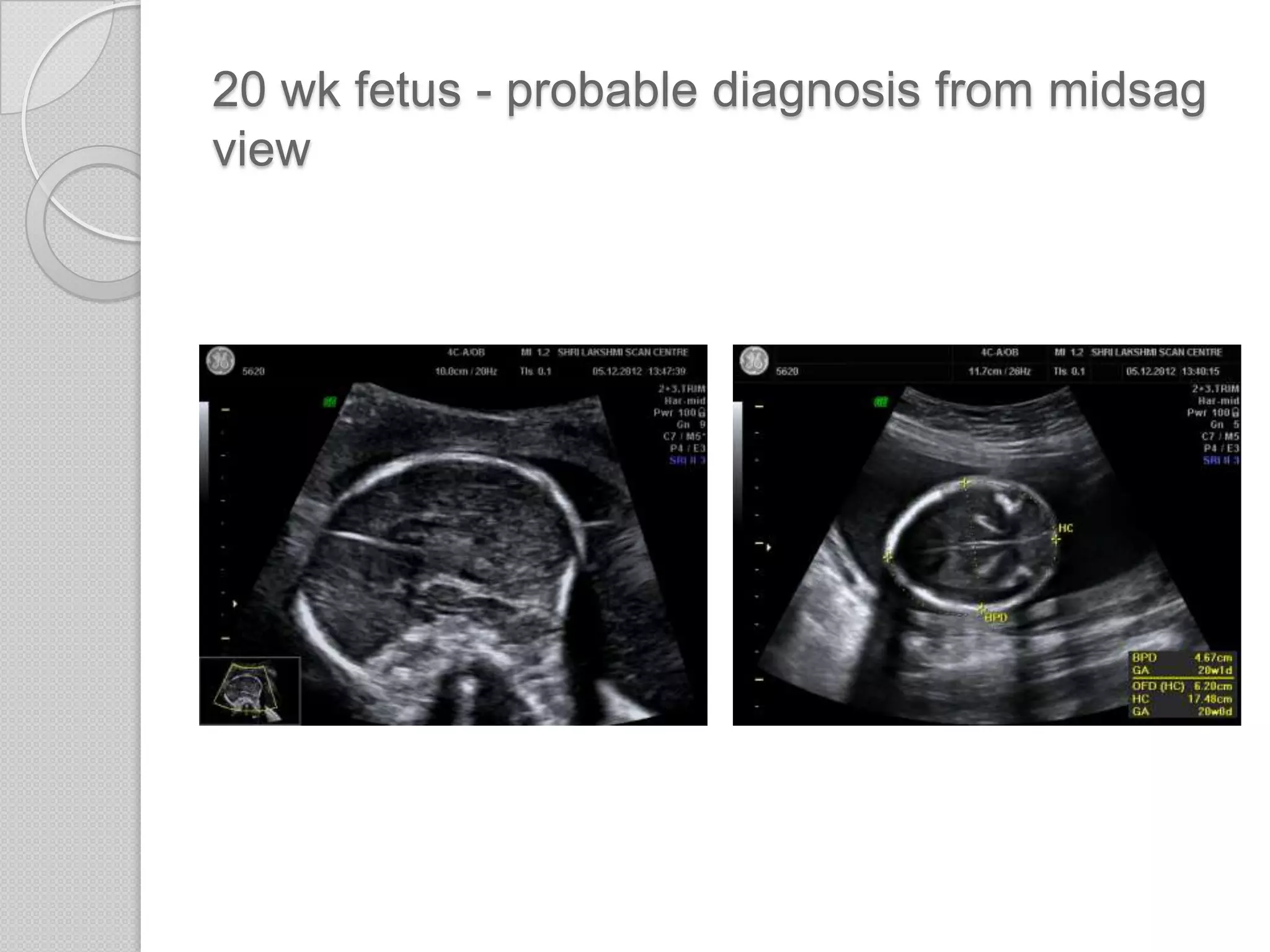
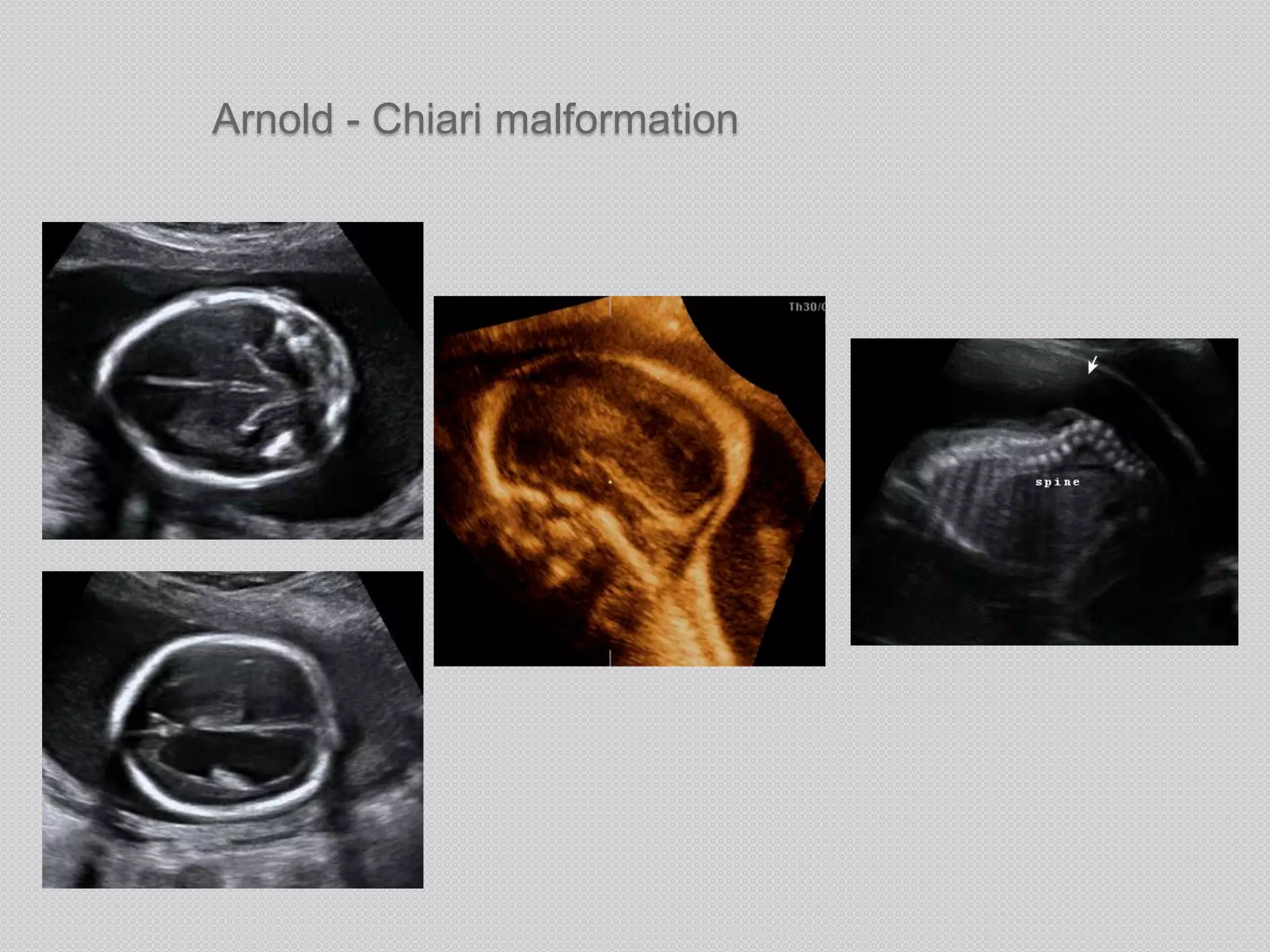
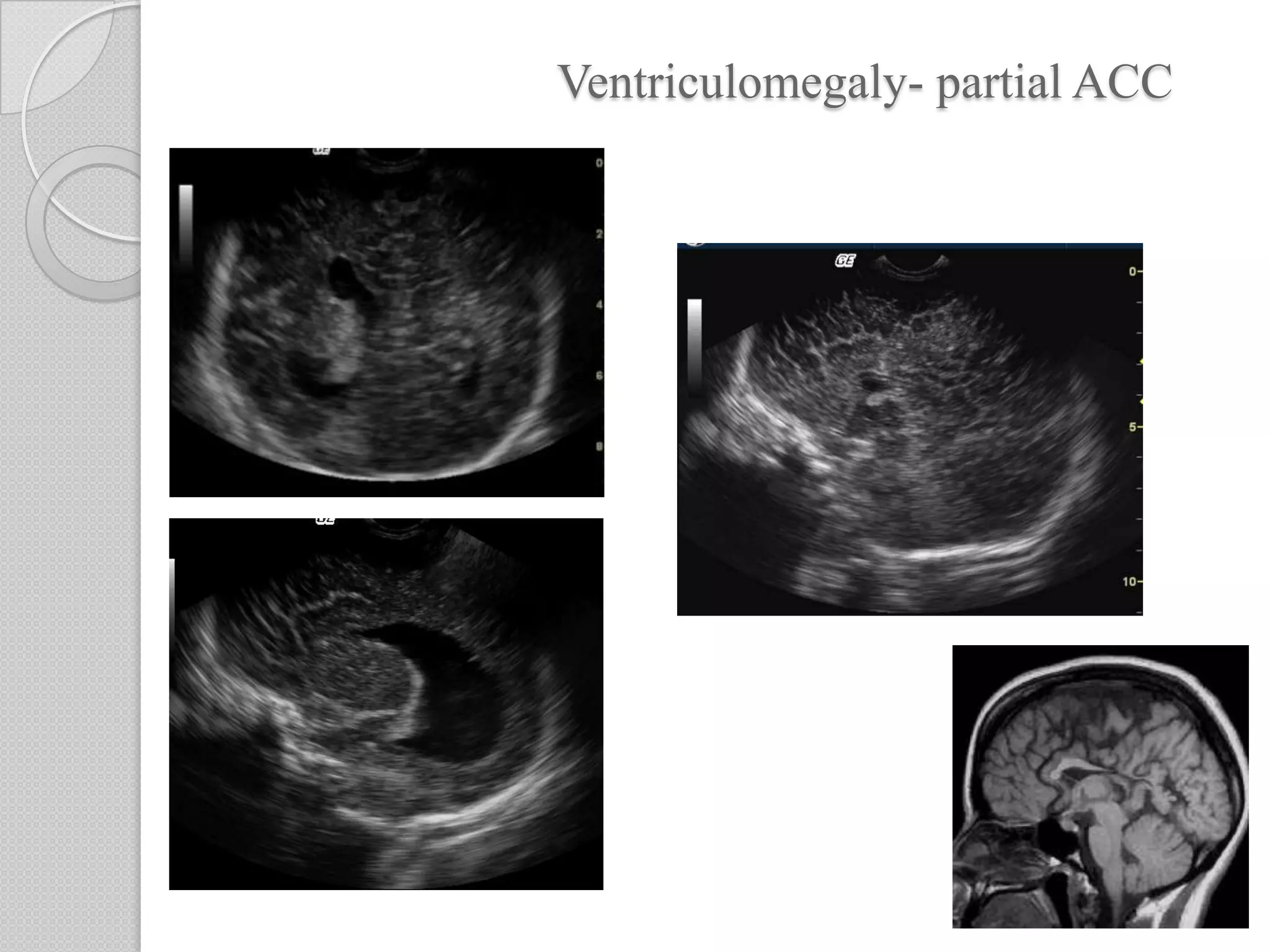
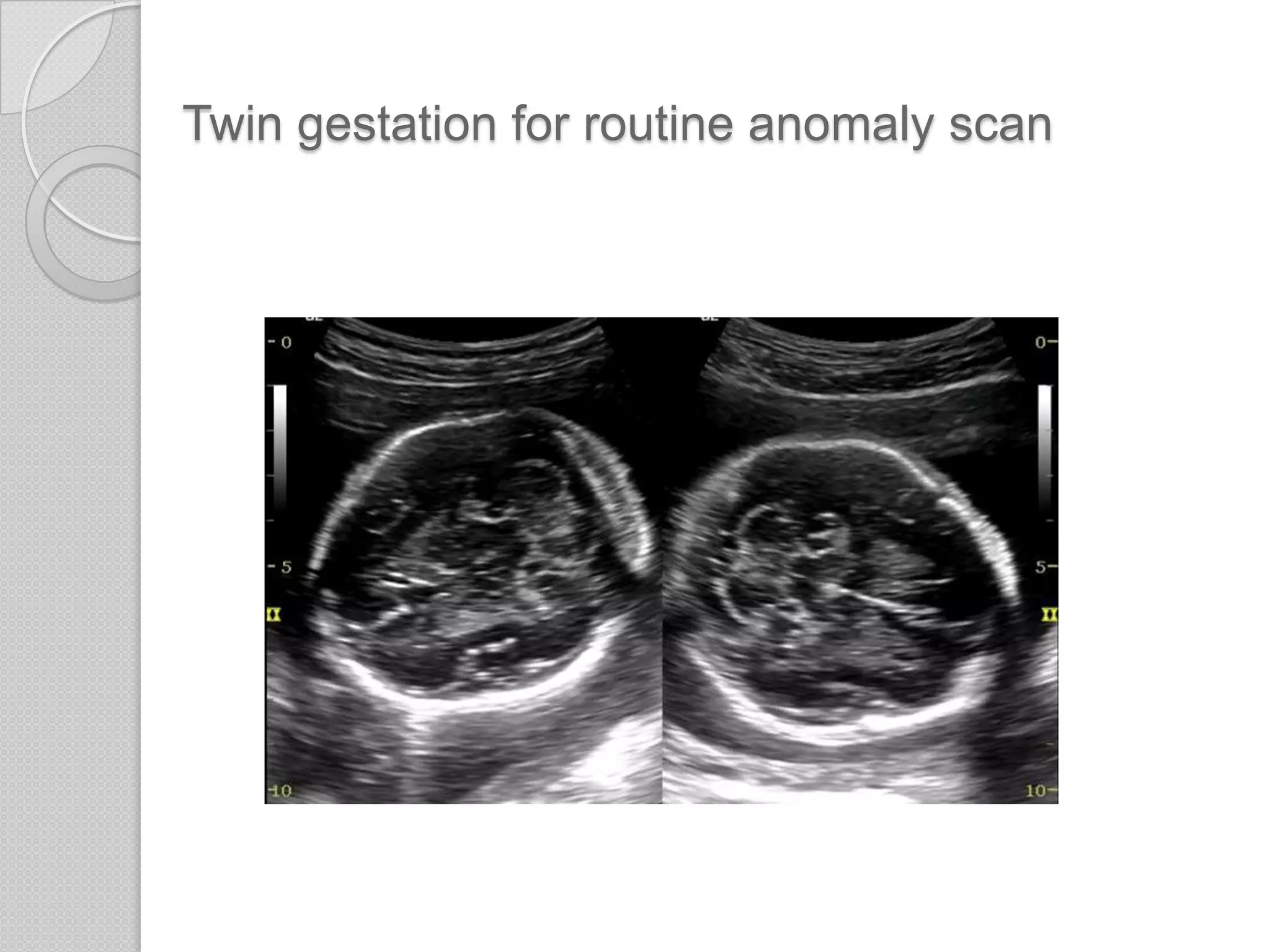
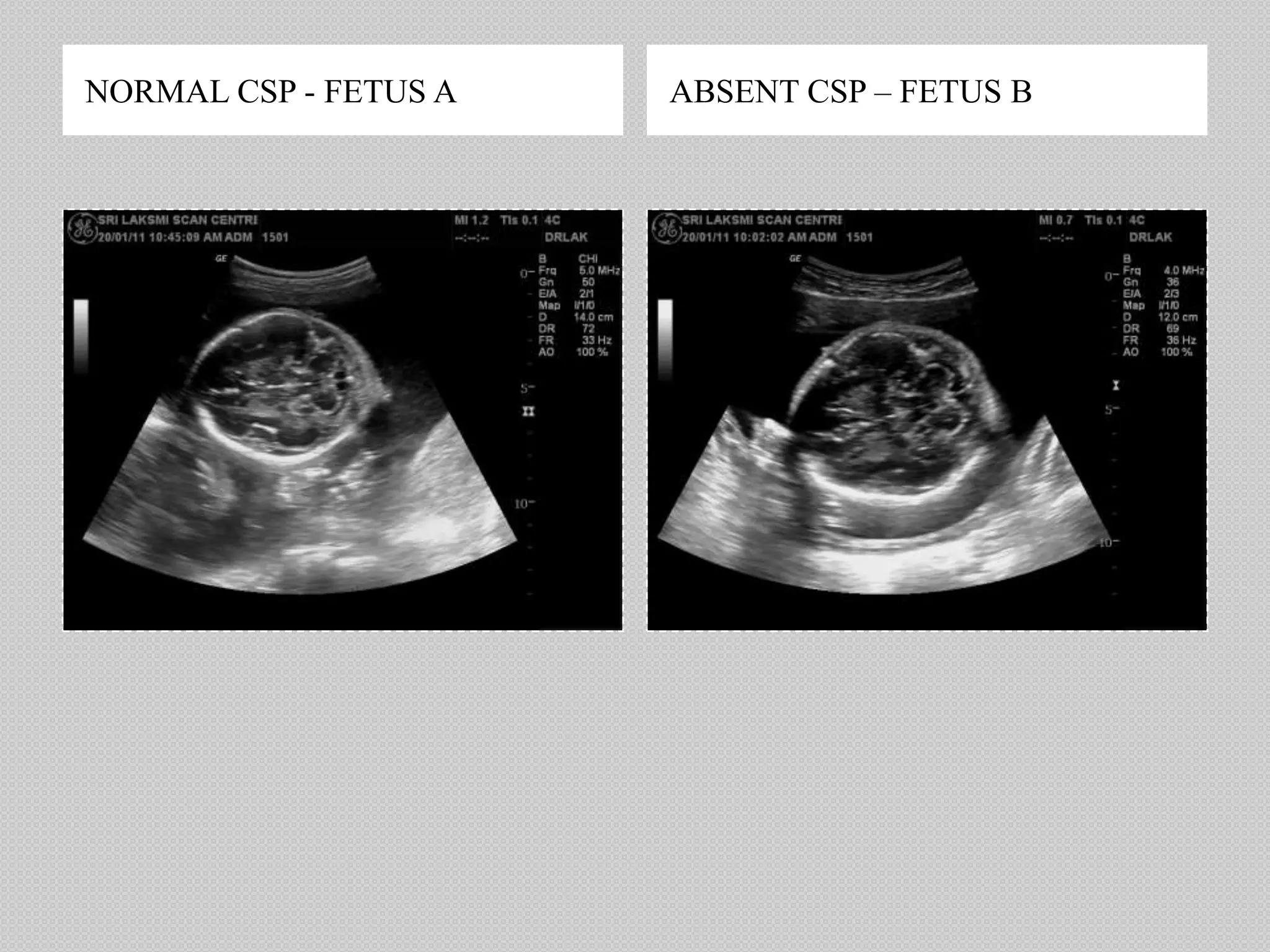
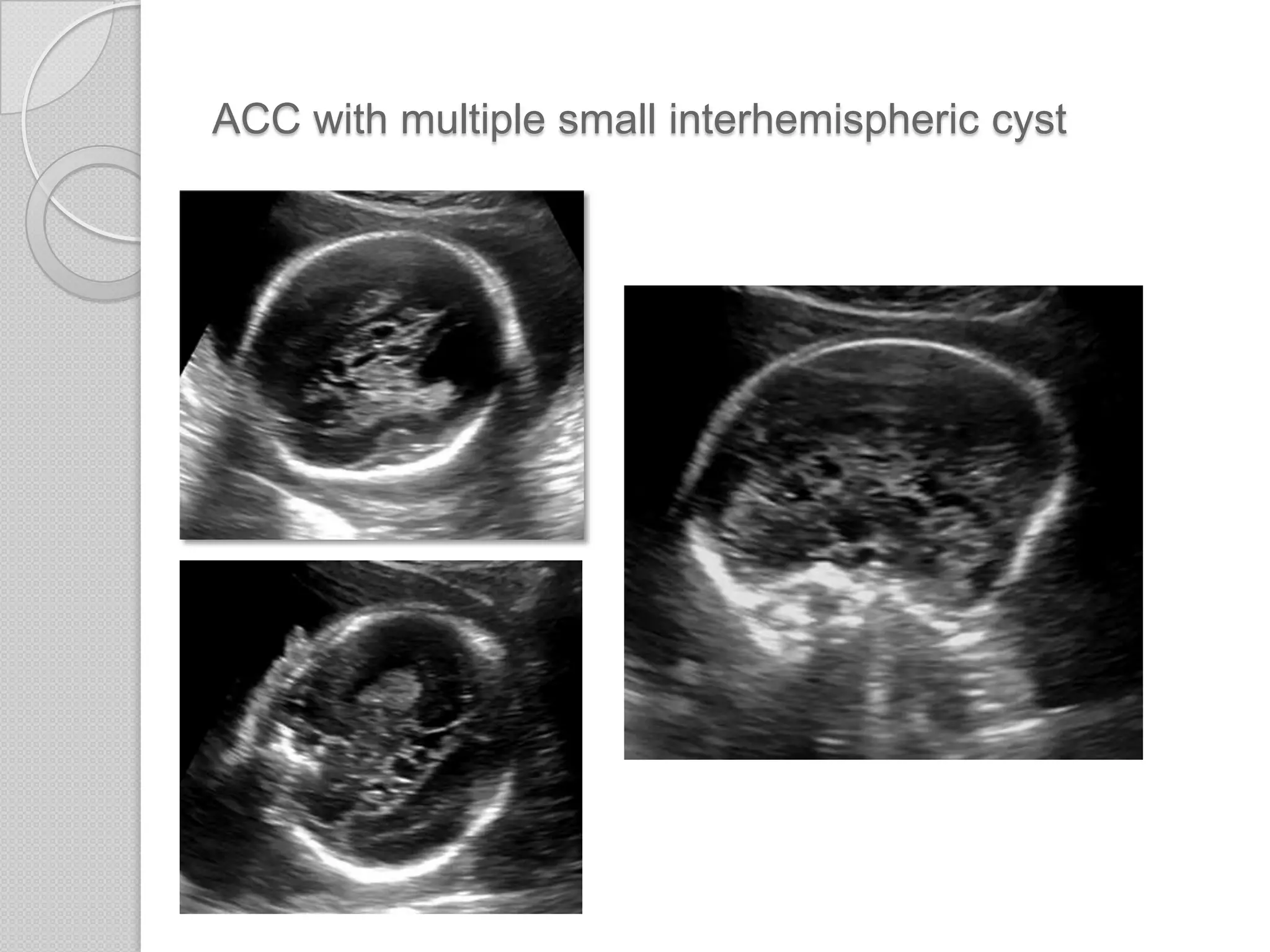
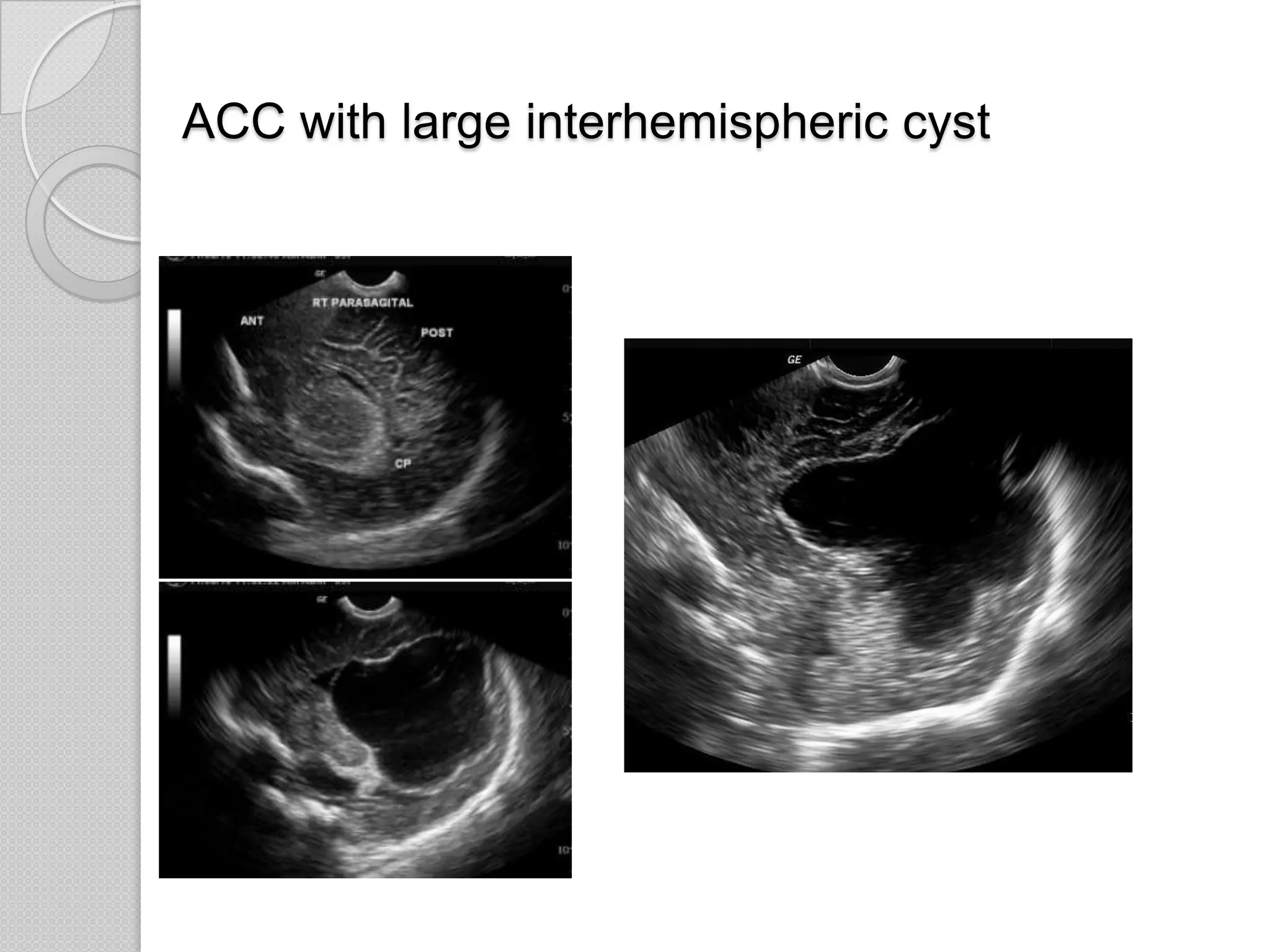
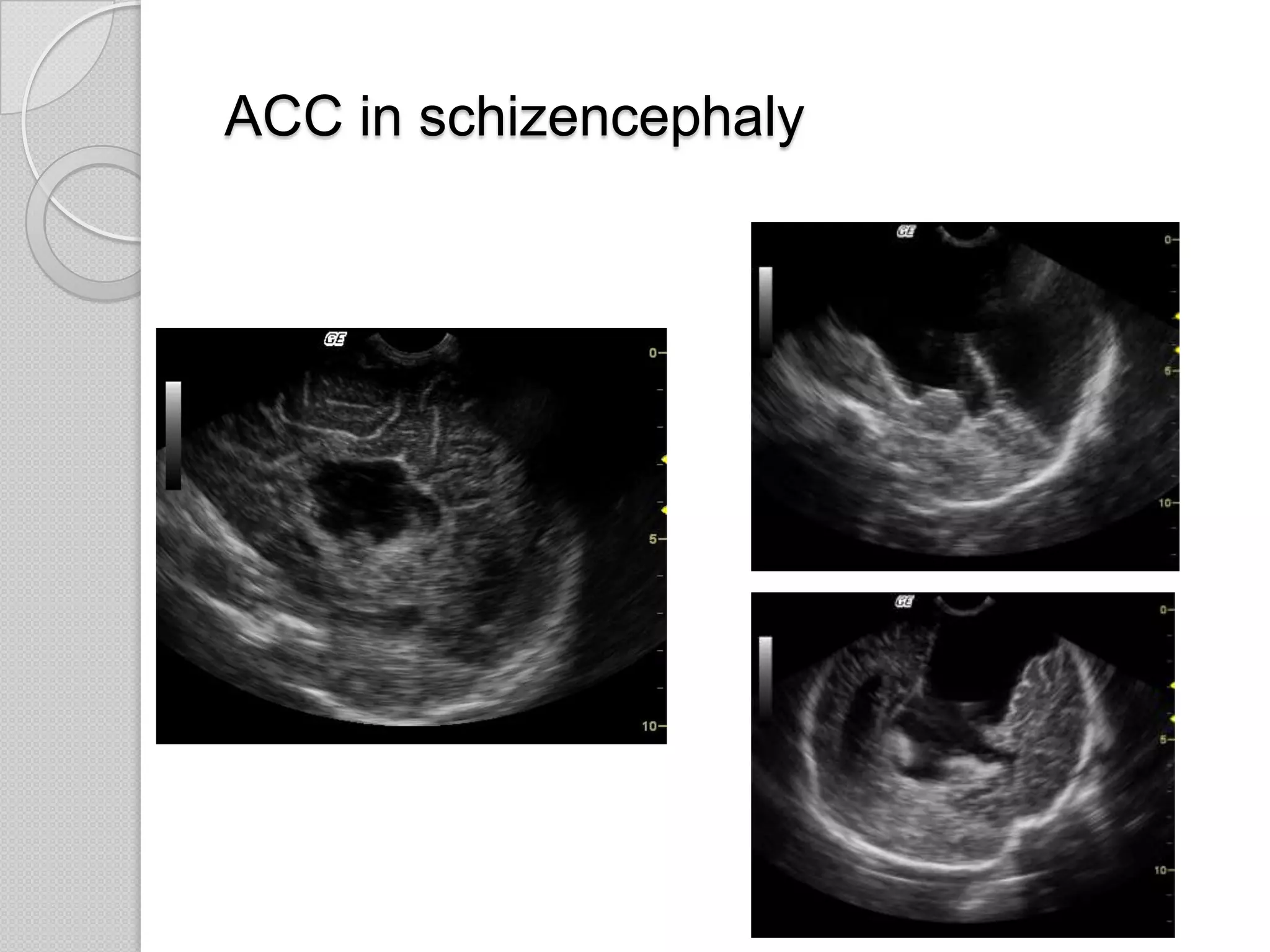
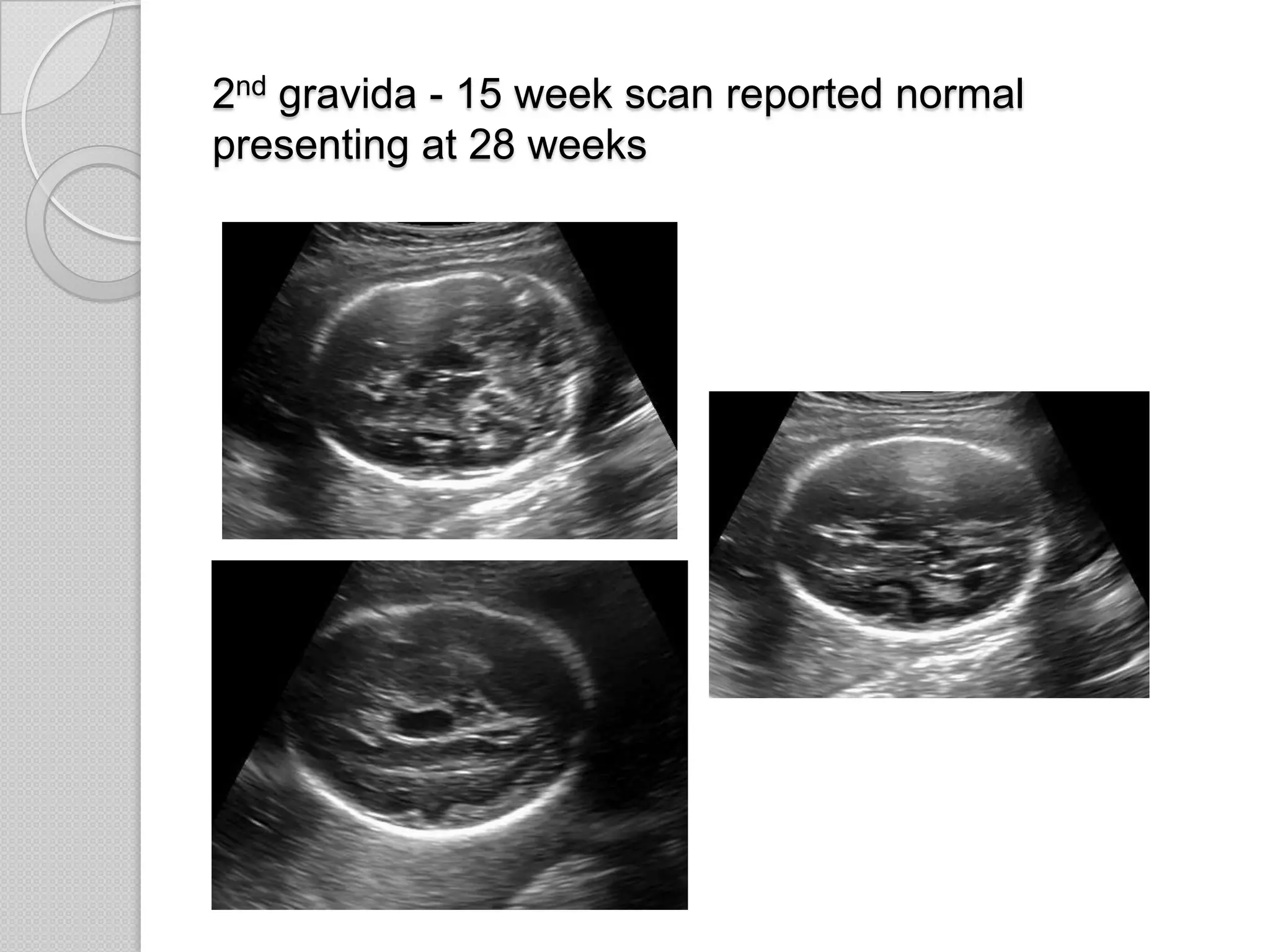
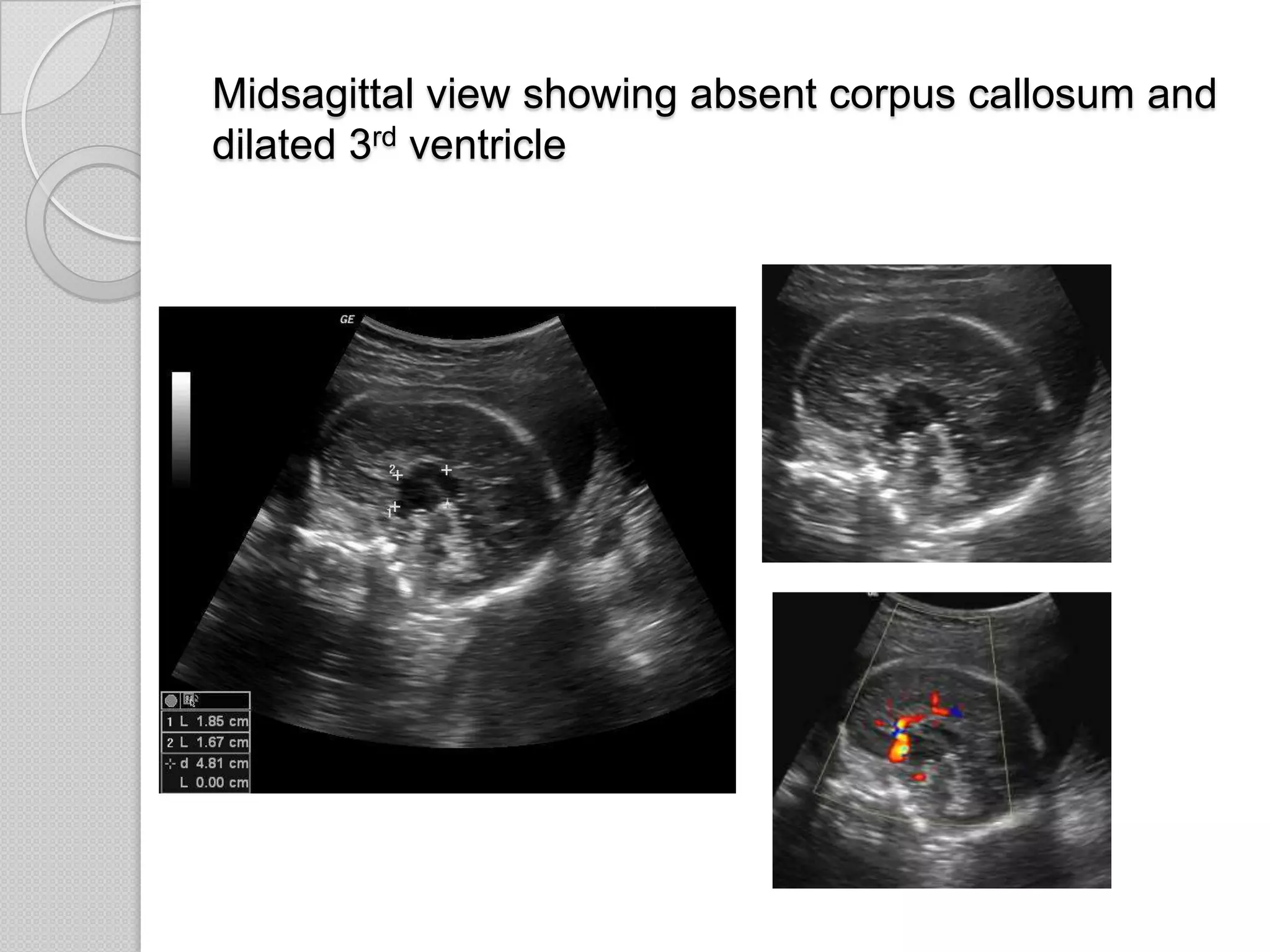
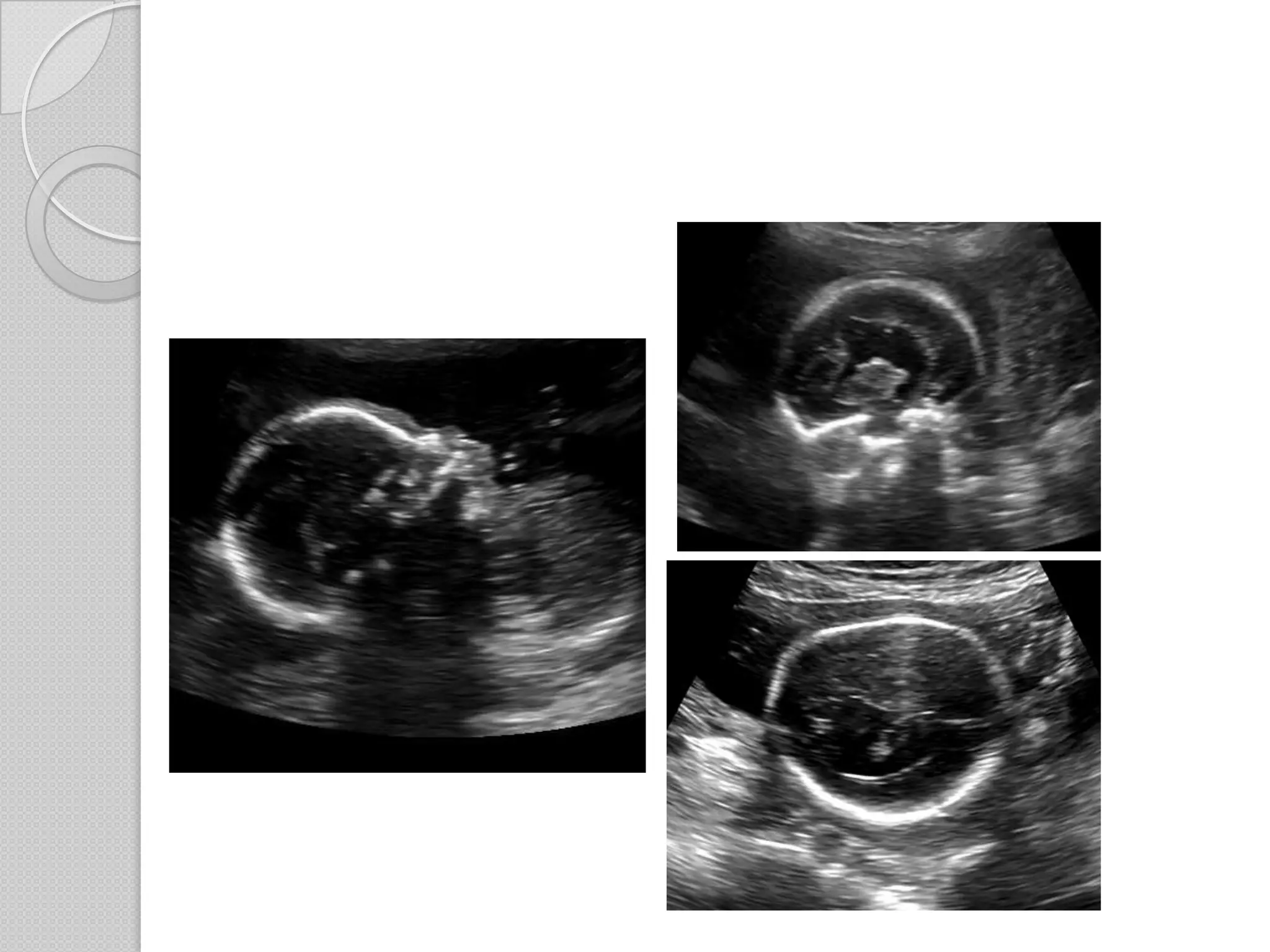
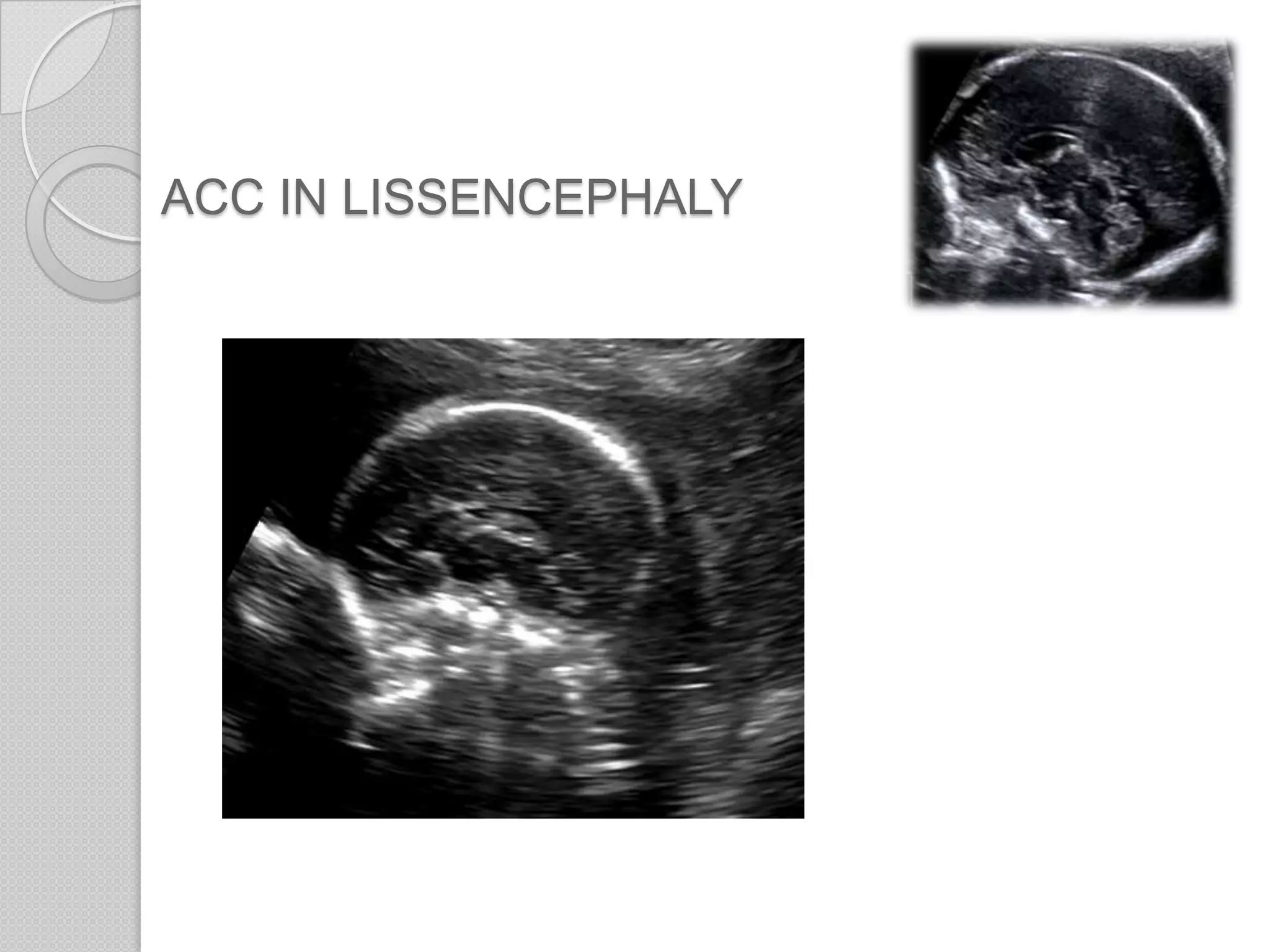
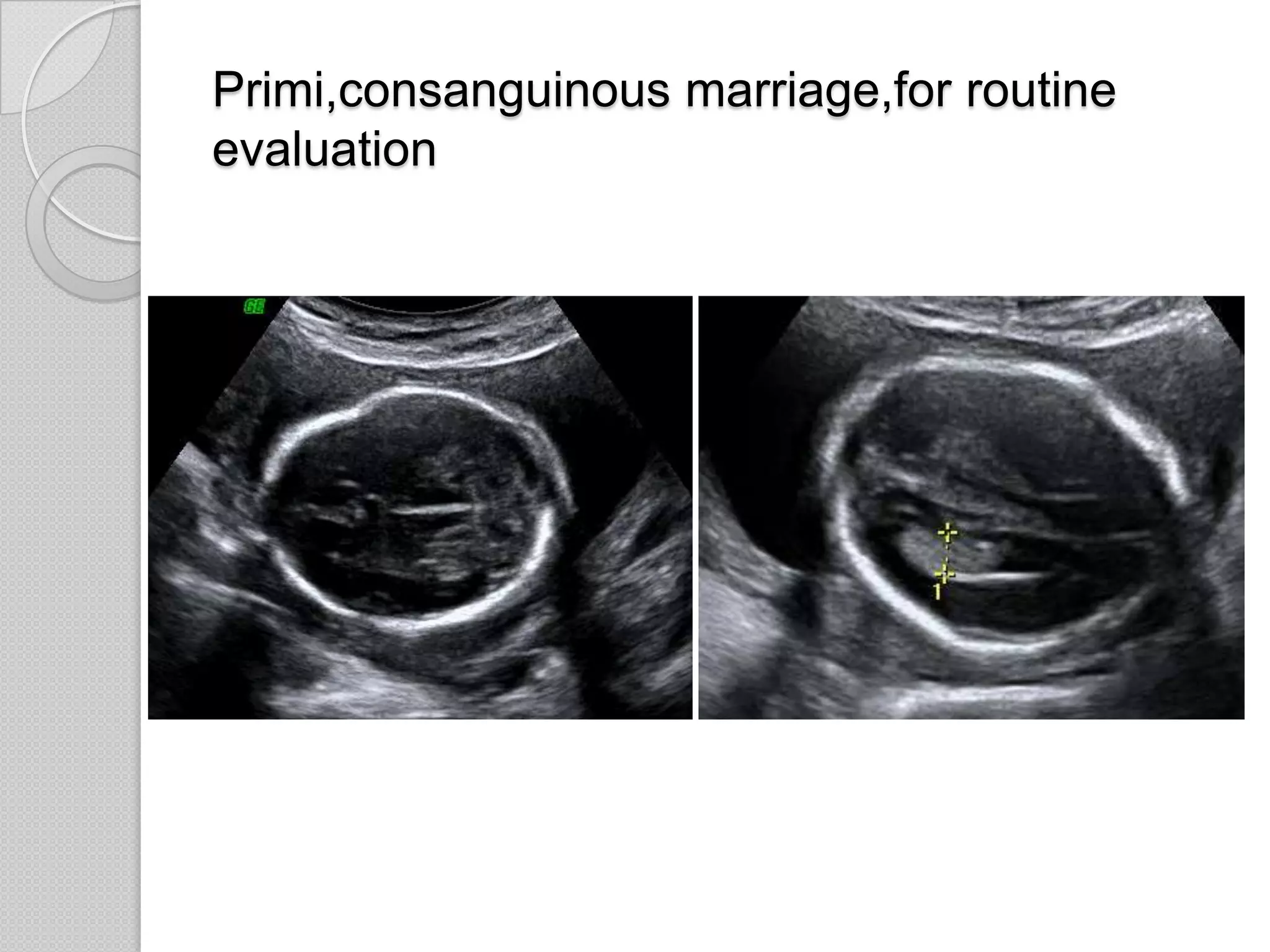
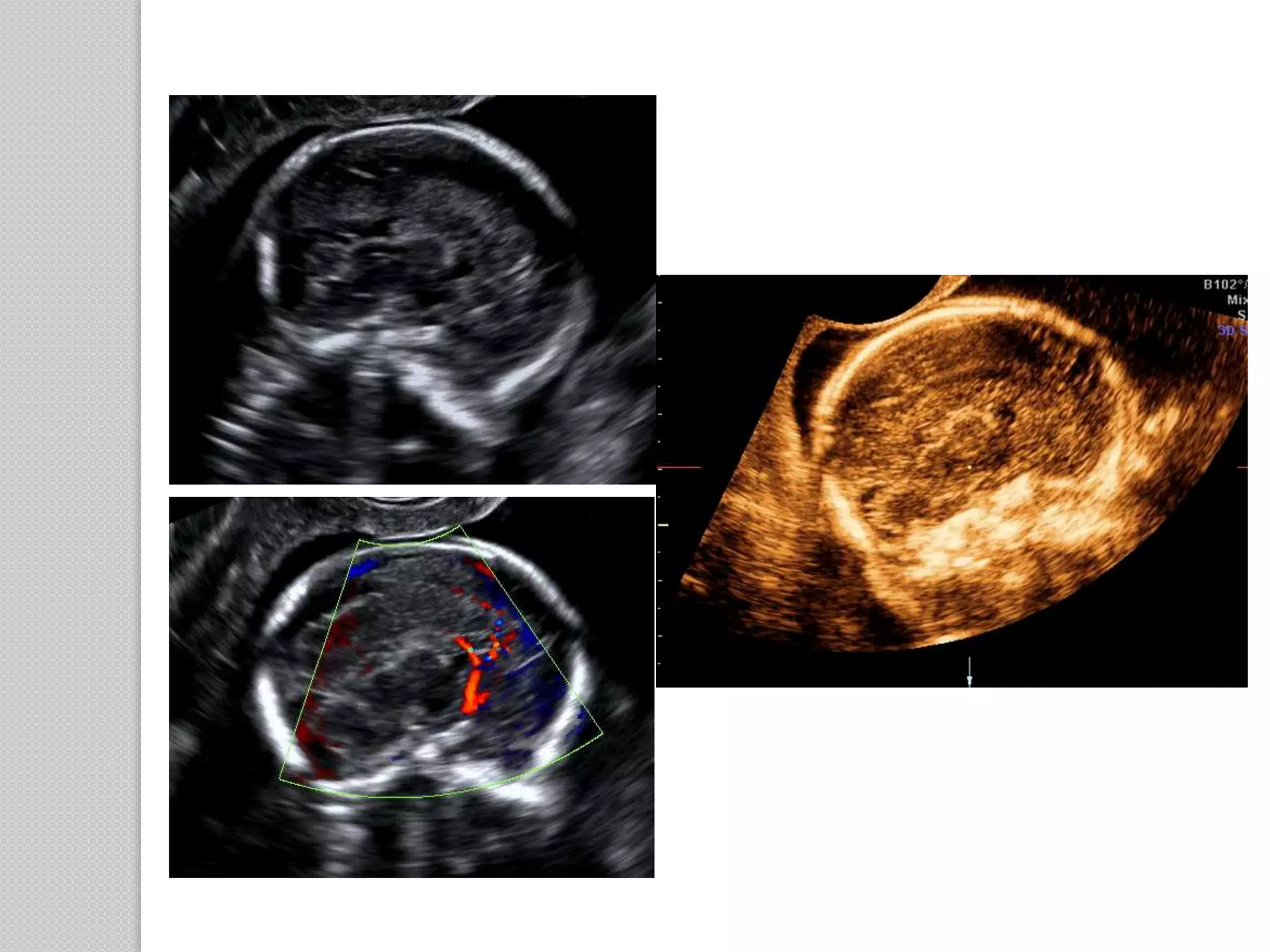
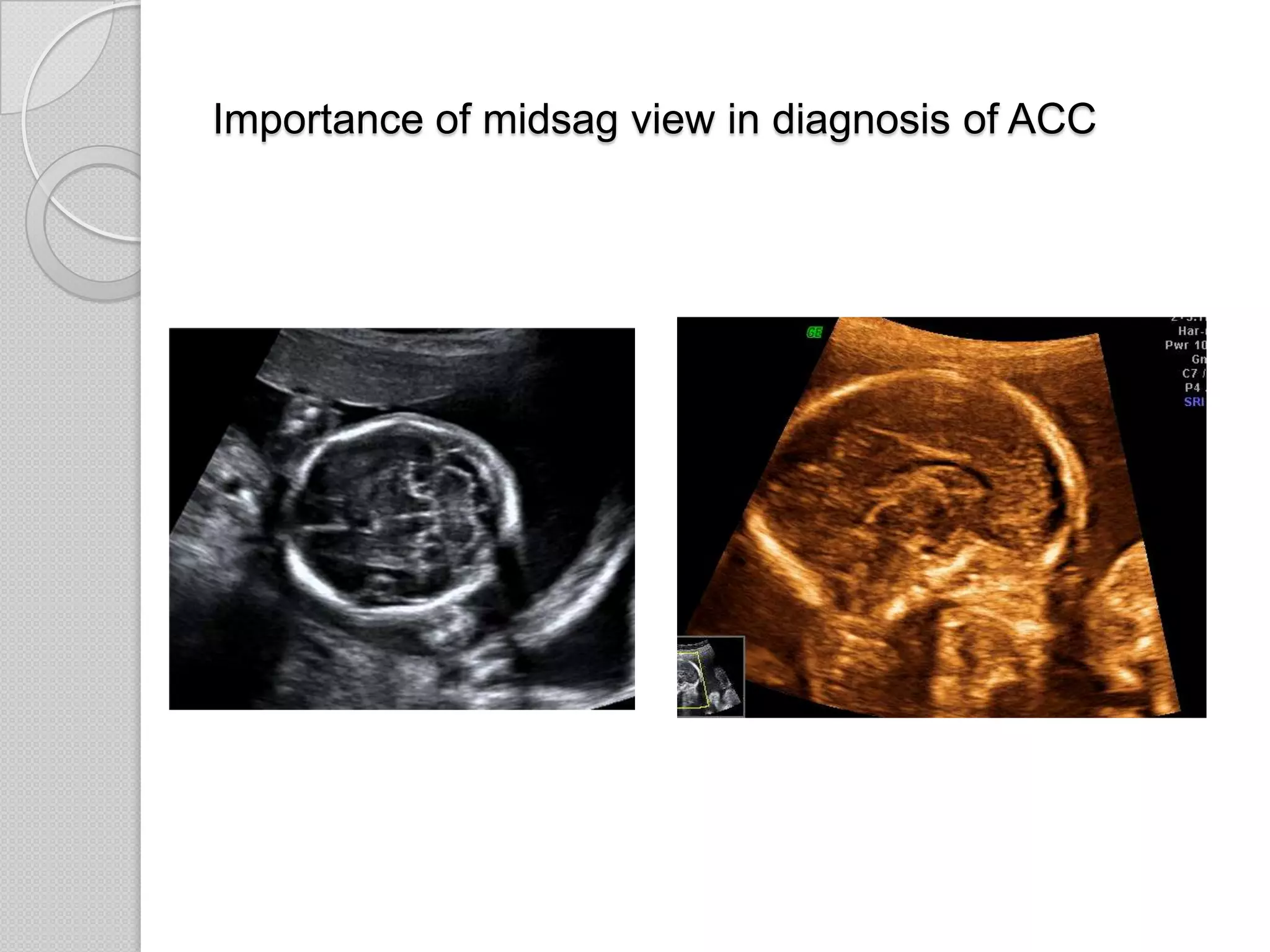
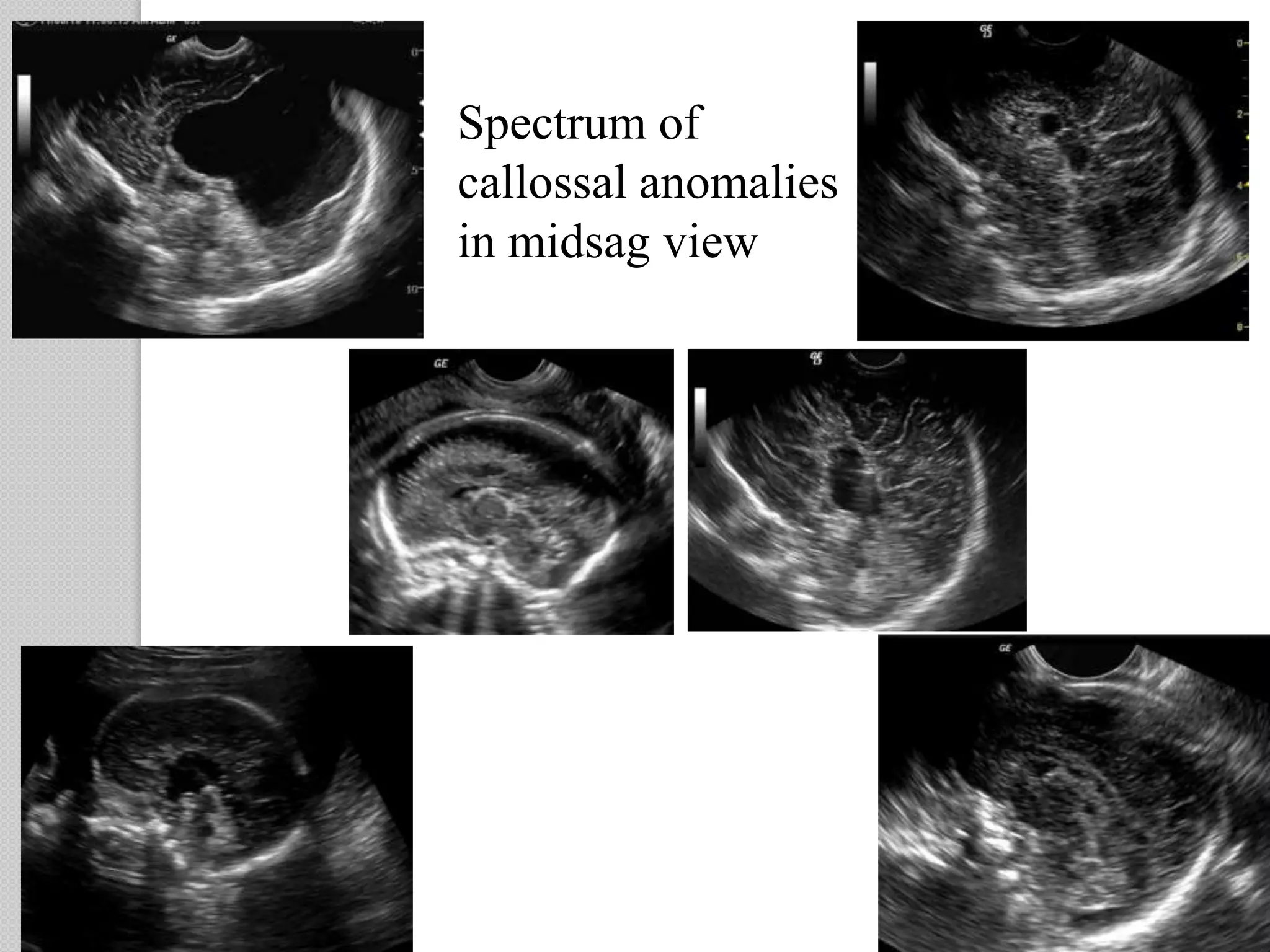
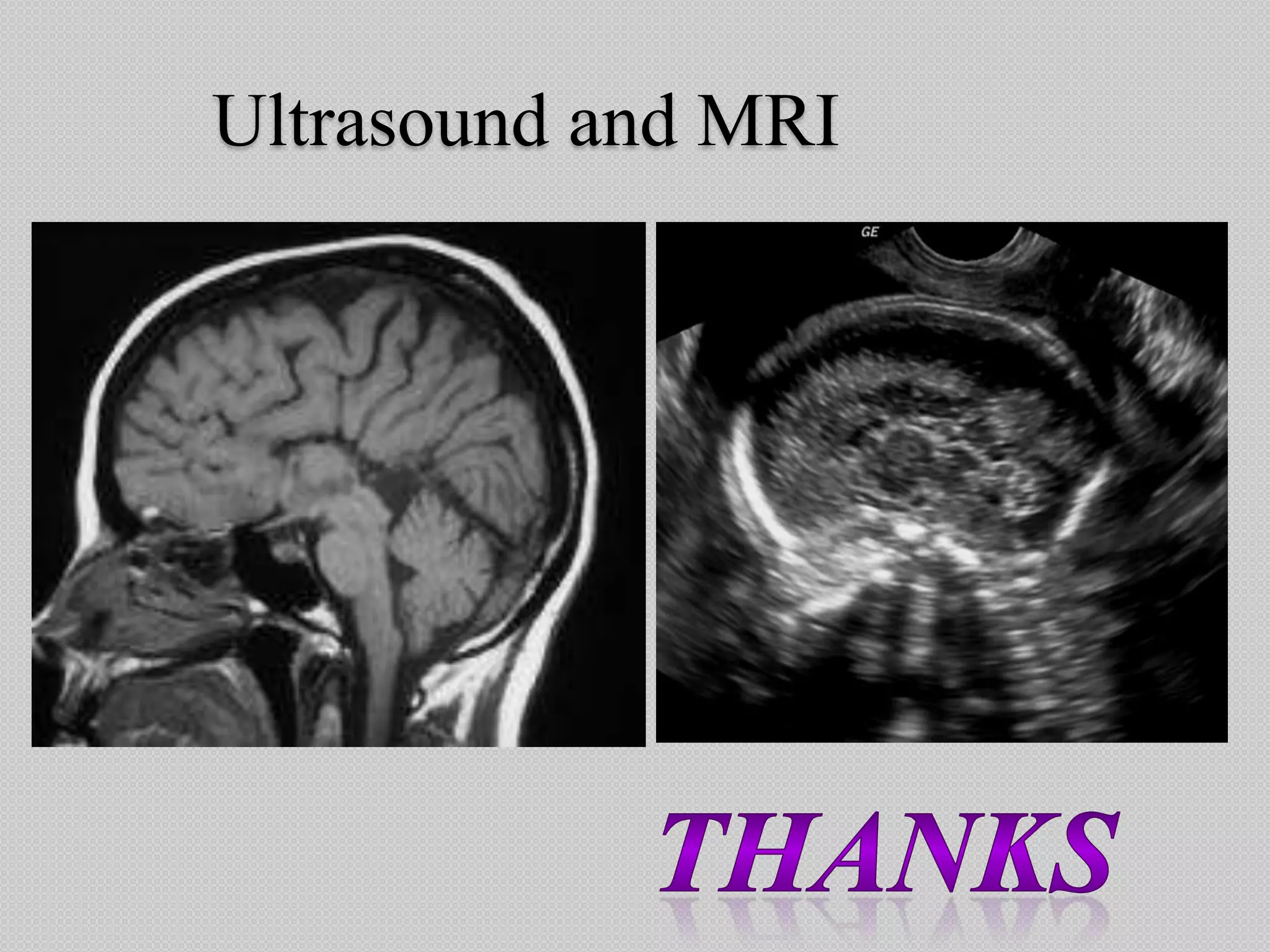
Abnormalities of the corpus callosum are frequently missed on prenatal ultrasound scans. Imaging the entire corpus callosum is not routinely performed, but is important for accurate diagnosis. Indirect markers like the cavum septum pellucidum seen on axial views can indicate abnormalities, but have limitations. A midline sagittal view of the brain is needed to directly visualize the corpus callosum and rule out abnormalities, but this view is often omitted from routine scans. Proper imaging of the corpus callosum is crucial for diagnosing conditions like agenesis of the corpus callosum.