Alcoholic liver disease by Sunil Kumar Daha
•Download as PPTX, PDF•
56 likes•15,690 views

please find the powerpooint presentation on Alcoholic liver disease presented by sunil kumar daha (me) and my friend Bishnu Ranjan Patel.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Alcoholic liver disease by Sunil Kumar Daha
Similar to Alcoholic liver disease by Sunil Kumar Daha (20)
More from sunil kumar daha
More from sunil kumar daha (20)
Recently uploaded
Recently uploaded (20)
Alcoholic liver disease by Sunil Kumar Daha
- 1. Alcoholic Liver Disease Presented by: Bishanu Ranjan Patel Sunil Kumar Daha
- 2. Introduction • Hepatic manifestations of alcoholic over consumption. 1. Fatty liver 2. Alcoholic Hepatitis 3. Alcoholic cirrhosis • ALD doesn’t occur below a threshold of alcohol consumption of :- • <14units/week in women • <21units/week in men • Alcoholics vs ALD 1 unit-8 gm
- 3. Risk factors • Quantity of alcohol — In men, 40–80 g/d of ethanol produces fatty liver; in women, 20-40 g/d is enough — 160 g/d for 10–20 years causes hepatitis or cirrhosis • Drinking pattern: Continuous vs. intermittent • Gender: Female twice > men • Genetics: Monozygotic twins Vs. dizygotic • Nutrition • Obesity • Malnutrition specially choline-deficient diet • Hepatitis C infection
- 5. Amount of alcohol in average drink Alcohol type % alcohol by volume Amount Units Beer 3.5 9 440 ml 440 ml 2 4 Wine 10 12 125 ml 750 ml 1 9 Alcopops 6 330 ml 2 Sherry 17.5 750 ml 13 Vodka/rum/gin 37.5 25 ml 1 Whisky/brandy 40 700 ml 28 Ref: Devidson’s 22nd edition
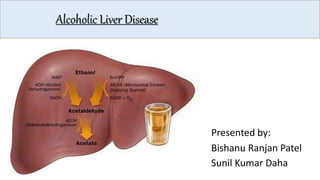
- 6. Metabolism of Alcohol Ethanol(80%) Acetaldehyde Acetyl co-A and Acetate Ethanol(20%) Acetate •Alcohol is metabolized in liver via 2 pathways :- NAD NADH Cyt CYP2E1Alcohol dehydrogenase Aldehyde dehydrogenase
- 7. Pathogenesis
- 10. 1. Alcoholic fatty liver • Accumulation of triglycerides within hepatocytes • Can be reversed if alcohol consumption is stopped or reduced significantly • Has a good prognosis, disappears after 3 months of abstinence
- 11. 2. Alcoholic Hepatitis • Hepatocyte injury is characterized by- • Mallorys Hyaline, Centrilobular necrosis, Fatty change, Hepatocyte ballooning, PMN infiltrate, Pericellular fibrosis • Worse prognosis than fatty liver disease • Precursors to cirrhosis • Potentially reversible with alcohol abstinence
- 12. 3. Alcoholic Liver cirrhosis • “A condition in which there is continuing fibrosis resulting in the subdivision of the liver into nodules of proliferating hepatocytes surrounded by scar tissue as the direct result of chronic alcohol abuse.” • Irreversible condition even with abstinence • Present in up to 50% of patients with biopsy-proven alcoholic hepatitis
- 13. Contd… Vicious circle of Chronic inflammation Fibrosis Nodular regeneration Distortion of architecture Hepatocellular necrosis
- 14. Clinical syndromes of Alcoholic Liver Diseases Fatty Liver Alcoholic hepatitis Cirrhosis • Asymptomatic • Abnormal liver biochemistry • Normal or large liver • RUQ discomfort • Nausea • Rarely jaundice • Asymptomatic • Jaundice • Malnutrition • Hepatomegaly • Features of portal hypertension e.g. ascites • encephalopathy • Stigmata of chronic liver diseases • Ascites/varices/enc ephalopathy • Large, normal or small liver • Hepatocellular carcinoma
- 15. Investigations • Macrocytosis in the absence of anaemia, may suggest and support a history of alcohol misuse • Unexplained rib fractures, particularly bilateral, on a chest X-ray are also suggestive of alcohol misuse • Presence of jaundice suggests alcoholic hepatitis Test Comment AST Increased two- to seven fold, <400 U/L, greater than ALT ALT Increased two- to sevenfold, <400 U/L AST/ALT Usually >1 GGTP Not specific to alcohol, easily inducible, elevated in all forms of fatty liver Bilirubin May be markedly increased in alcoholic hepatitis despite modest elevation in alkaline phosphatase PT Prolonged Albumin Hypoalbuminemia PMN If>5500/ml Predicts severe alcoholic hepatitis when discriminant function > 32
- 16. Contd… • We can also send for: • Ultrasonography: fatty infiltration and determine liver size portal vein flow reversal, ascites, and intra-abdominal collaterals indicates serious liver injury with less potential for complete reversal of liver disease • Liver Biopsy:
- 17. Prognosis • Critically ill patients with alcoholic hepatitis have short- term (30-day) mortality rates >50% • Presence of ascites, variceal hemorrhage, deep encephalopathy, or hepatorenal syndrome predicts a dismal prognosis • Pathologic stage of the injury by liver biopsy
- 18. Discriminant Function (DF) • Aka ‘Maddrey score’ DF = (4.6 x increase in PT sec. )) + (serum bilirubin mg/dl) • To assess prognosis in alcoholic hepatitis A value over 32 implies severe liver disease with a poor prognosis
- 19. Glasgow Alcoholic Hepatitis Score Score 1 2 3 Age < 50 > 50 WCC (× 109/L) < 15 > 15 > 2.0 Urea (mmol/L) < 5 > 5 > 250 PT ratio < 1.5 1.5-2.0 Bilirubin (μmol/L) < 125 125-250 A score > 9 is associated with a 40% 28-day survival, compared to 80% for patients with a score < 9
- 20. Model for End-stage Liver Disease (MELD) 1-year survival (%) MELD score No complications Complications < 9 97 90 10-19 90 85 20-29 70 65 30-39 70 50 MELD from SI units 10 × (0.378[In serum bilirubin (μmol/L) + 1.12[In INR] + 0.957[In serum creatinine (μmol/L)] + 0.643) MELD from non-SI units 3.8 [In serum bilirubin (mg/dL)] + 11.2 [In INR] + 9.3 [In serum creatinine (mg/dL)] + 6.4
- 21. Management 1. Alcohol Abstinence 2. Nutritional Support 3. Corticosteroid Therapy 4. Pentoxifylline 5. Liver Transplantation * We also have to manage for :- • Alcohol withdrawal and Wernicke's encephalopathy • Treatment for complications of cirrhosis, such as variceal bleeding, encephalopathy and ascites
- 23. 1. Alcohol abstinence • Most important treatment of all • Effective in preventing progression of disease • Alcohol withdrawal syndrome and Wernicke’s encephalopathy need parallel treatment too
- 24. 2. Nutritional support • Protein supplementation • Vit A • Folate • Vit B6 • Thiamine
- 25. 3. Corticosteroids • Glucocorticoids have been found to be beneficial in patients with severe alcoholic hepatitis (Maddrey’s DF score ≥32). • Survival rate found to be increased in those with Glasgow score >9 • Sepsis is the main side effect • Should not be given to patients with active GI bleeding, sepsis, renal failure or pancreatitis.
- 26. 4. Pentoxifylline • Anti- TNF action • Reduce incidence of hepato-renal failure • Given in severe alcoholic hepatitis in whom corticosteroids cannot be given
- 27. References • Harrison’s Principle of Medicine,19th edition • Davidson’s Principle and Practice of Medicine, 22nd edition • Kumar and Clark’s Clinical Medicine, 8th edition
- 28. Thank You!
Editor's Notes
- Although alcohol is considered a direct hepatotoxin, only between 10 and 20%of alcoholics will develop alcoholic hepatitis. The explanation for this apparent paradox is unclear but involves the complex interaction of facilitating factors, such as drinking patterns, diet, obesity, and gender. There are no diagnostic tools that can predict individual susceptibility to alcoholic liver disease.
- Quantity and duration of alcohol intake are the most important risk factors involved in the development of alcoholic liver disease.
- Alcohol directly affects stellate cells, transforming them into collagen producing myofibroblast cells