
Recommended
More Related Content
What's hot
What's hot (20)
Similar to pneumonia_nursing_care_plan.docx
Similar to pneumonia_nursing_care_plan.docx (20)
Recently uploaded
Recently uploaded (20)
pneumonia_nursing_care_plan.docx
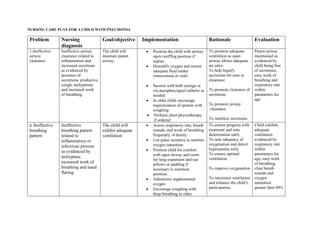
- 1. NURSING CARE PLAN FOR A CHILD WITH PNEUMONIA Problem Nursing diagnosis Goal/objective Implementation Rationale Evaluation 1.Ineffective airway clearance Ineffective airway clearance related to inflammation and increased secretions as evidenced by presence of secretions, productive cough, tachypnoea and increased work of breathing. The child will maintain patent airway. Position the child with airway open (sniffing position if supine Humidify oxygen and ensure adequate fluid intake (intravenous or oral) Suction with bulb syringe or via nasopharyngeal catheter as needed. In older child, encourage expectoration of sputum with coughing Perform chest physiotherapy if ordered To promote adequate ventilation as open airway allows adequate air entry. To help liquefy secretions for ease in clearance. To promote clearance of secretions. To promote airway clearance. To mobilize secretions. Patent airway maintained as evidenced by child being free of secretions, easy work of breathing and respiratory rate within parameters for age. 2. Ineffective breathing pattern Ineffective breathing pattern related to inflammatory or infectious process as evidenced by tachypnea, increased work of breathing and nasal flaring. The child will exhibit adequate ventilation Assess respiratory rate, breath sounds, and work of breathing frequently -4 hourly. Use pulse oximetry to monitor oxygen saturation. Position child for comfort with open airway and room for lung expansion and use pillows or padding if necessary to maintain position. Administer supplemental oxygen Encourage coughing with deep breathing in older To ensure progress with treatment and note deterioration early. To note adequacy of oxygenation and detect hypoxaemia early. To ensure optimal ventilation. To improve oxygenation To maximize ventilation and enhance the child’s participation. Child exhibits adequate ventilation evidenced by respiratory rate within parameters for age, easy work of breathing, clear breath sounds and oxygen saturation greater than 94%
- 2. children which can be done through play Problem Nursing diagnosis Goal/objective Implementation Rationale Evaluation 2. Impaired Gas exchange. Impaired Gas exchange related to airway plugging, hyperinflation and atelectasis as evidenced by cyanosis and decreased oxygen saturation The child will have adequate gas exchange • Monitor oxygen saturation via pulse oximetry • Encourage clearance of secretions via coughing, expectoration, chest physiotherapy and suctioning.. • Administer bronchodilators if ordered(e.g. salbutamol) To detect alterations in oxygenation. Mobilization of secretions improves gas exchange To treat broncho spasms and improve gas exchange. Gas exchange adequate evidenced by oxygen saturation within normal parameters and absence of cyanosis 3. Risk of Fluid volume deficit Risk of Fluid volume deficit related to decreased oral intake, insensible losses due to fever, tachypnea, or diaphoresis Fluid volume will be maintained • In the initial stages, administer intravenous fluids as orderd. (e,g ½ strength darrows). In nil per oral state administer oral fluids via naso gastric tube • Allow oral intake as childs condition improves and no longer in respiratory distress. Encourage oral fluids by giving favourite fluids. • Assess for signs of adequate hydration (good skin turgor, moist mucosa, adequate urine output). To maintain adequate hydration To prevent aspiration To maintain adequate hydration. To note improvement To identify fluid imbalance Fluid volume maintained evidenced by moist oral mucosa, good skin turgor and urine output at least 1 to 2 mL/kg/hr.
- 3. • Strictly monitor fluid intake and output Problem Nursing diagnosis Goal/objective Implementation Rationale Evaluation 4. Altered nutrition less than body requirements Altered nutrition less than body requirements related to inability to feed or loss of appetite as evidenced by poor oral intake Child will maintain adequate nutritional intake Introduce small frequent feeds as child’s condition improves. In older children, oral toilet can be done. Assist family and child to choose higher-calorie, protein-rich foods Coax younger children to eat better by playing games and offering favourite foods Small frequent meals are better tolerated To increases child’s appetite To optimize growth potential. To improve food intake. Adequate nutritional intake maintained as evidenced by weight gain or weight maintenance. 5, Activity intolerance Activity intolerance related to high respiratory demand as evidenced by increased work of breathing and requirement for frequent rest when playing. Child will resume normal activity level Provide rest periods balanced with periods of activity. Carry out nursing procedures collectively and allow visiting of the child at scheduled times. Activity increases myocardial oxygen demand so must be balanced with rest. • Provide small, frequent meals • Encourage quiet activities that do not require exertion • Allow gradual increase in activity as tolerated, keeping pulse To allow for sufficient rest hence promoting activity tolerance when awake To prevent overtiring and abdominal distension as infants and younger children use abdominal muscles for breathing To prevent boredom. To minimize risk for further respiratory compromise. Child able to tolerate activity without difficulty breathing. Pulse oximetry reading within normal range
- 4. oximetry reading within normal parameters. Problem Nursing diagnosis Goal/objective Implementation Rationale Evaluation 6. Fear and anxiety Fear and anxiety related to difficulty breathing, unfamiliar personnel, procedures, and environment (hospital) as evidenced by clinging, crying, fussing, verbalization, or lack of cooperation To allay anxiety and reduce fear • Establish trusting relationship with the child and family. • Explain procedures to child at developmentally appropriate level • Provide favourite blanket or toy to the child, as well as comfort measures preferred by child such as rocking or music. • Involve parents in care of the child, allow caretaker to spend enough time with the child and allow for periods of play To decrease anxiety and fear. To decrease fear of unknown. For added security To allay anxiety and decrease fear. Fear and anxiety allayed evidenced by decreased episodes of crying or fussing, child appears happy and will be able to play. 7. Altered family processes. Family processes altered, related to child’s illness or hospitalization as evidenced by family’s presence in the hospital, missed work and demonstration of inadequate coping Parents will demonstrate adequate coping and decreased anxiety. • Encourage parent’s verbalization of concerns related to child’s illness. • Explain therapy, procedures, and child’s behaviour to parents. This allows for identification of concerns and demonstrates to the family that the nurse cares about them as well. To develop an understanding of the child’s current status which helps decrease anxiety Parents demonstrate adequate coping and decreased anxiety: Parents are involved in child’s care, ask appropriate questions and are able to
- 5. •Encourage parental involvement in child’s care. This makes parents feel needed and valued. discuss child’s care and condition calmly. TIME SPECIFIC OBJECTIVE CONTENT TEACHING METHOD AUDIO VISUAL AIDS TEACHER’S ACTIVITY STUDENT’S ACTIVITY EVALUATION List the complication of pneumonia Pleural effusion Empyema Lung abscess Sepsis pneumothorax Lecture/ Discussion Flip chart LCD Markers Explaining. Asking questions Listening Taking notes Asking questions What are the complications of pneumonia?
- 6. REFERENCES Hull J and Johnson D.I (1999). Essential Paediatrics. 4th edition. Churchill. London. Lassauer T and Clayden G. (2001). Illustrated Textbook of Paediatrics. 2nd edition. Mosby. London. Royle A.J and Walsh M, (1992), Watson’s Medical – Surgical Nursing and Related Physiology, 4th Edition, Butler and Tanner Ltd, Frome and London, Great Britain. Ignatavicius D.D and Workman M.L, (2002), Medical Surgical Nursing: Critical Thinking for Collaborative care, 4th Edition, W.B. Saunders Company, Philadelphia, USA