This document summarizes evidence on improving health and welfare for people living in slums. It presents a three-level causal model for analyzing interventions: macro-level national policies; meso-level slum-specific policies like tenure; and micro-level targeted interventions. Relocation is often disappointing and in-situ upgrading through measures like sanitation, health services, and secure tenure is generally preferable. Future policy and research should consider slums' heterogeneous contexts and potential for increasing returns through neighborhood effects of interventions.
Mattingly "AI & Prompt Design: The Basics of Prompt Design"
www.thelancet.com Vol 389 February 4, 2017 559Series.docx
1. www.thelancet.com Vol 389 February 4, 2017 559
Series
The health of people who live in slums 2
Improving the health and welfare of people who live in slums
Richard J Lilford, Oyinlola Oyebode, David Satterthwaite, G J
Melendez-Torres, Yen-Fu Chen, Blessing Mberu, Samuel I
Watson, Jo Sartori,
Robert Ndugwa, Waleska Caiaff a, Tilahun Haregu, Anthony
Capon, Ruhi Saith, Alex Ezeh
In the fi rst paper in this Series we assessed theoretical and
empirical evidence and concluded that the health of
people living in slums is a function not only of poverty but of
intimately shared physical and social environments. In
this paper we extend the theory of so-called neighbourhood eff
ects. Slums off er high returns on investment because
benefi cial eff ects are shared across many people in densely
populated neighbourhoods. Neighbourhood eff ects also
help explain how and why the benefi ts of interventions vary
between slum and non-slum spaces and between slums.
We build on this spatial concept of slums to argue that, in all
low-income and-middle-income countries, census
tracts should henceforth be designated slum or non-slum both to
inform local policy and as the basis for research
surveys that build on censuses. We argue that slum health
should be promoted as a topic of enquiry alongside
poverty and health.
Introduction
2. The fi rst paper in this Series was concerned with health
in slums and with the determinants of health.1 We noted
that the intimately shared physical and social
environment in slums is likely to generate strong
neighbourhood eff ects. In this second paper, we consider
what can be done to improve health and health care in
slums and show how factors operating at the
neighbourhood level can be turned to advantage when
we intervene. We start by discussing general
epidemiological principles that should be taken into
account in interpreting the results of studies in slums.
Next, we describe an intellectual framework to organise
evidence on interventions. We then present such
evidence as we were able to glean according to this
intellectual framework. Lastly, we discuss the
implications of the fi ndings from this Series as a whole
for policy and research.
Three factors interact to determine how an intervention
can play out in slum neighbourhoods. First, densely
packed slum neighbourhoods promote the spread of
disease but also provide opportunities for economies of
scale when interventions are promulgated. An iconic
example is the dramatic eff ect John Snow achieved when
he aborted a cholera epidemic by disenabling a water
pump in Soho, London in 1854.
Second, we showed in paper one that slums are not
homogeneous, but present very diff erent social and
physical environments. Context should therefore be taken
Lancet 2017; 389: 559–70
Published Online
October 16, 2016
3. http://dx.doi.org/10.1016/
S0140-6736(16)31848-7
This is the second in a Series of
two papers about the health of
people who live in slums
Warwick Centre for Applied
Health Research and Delivery,
University of Warwick,
Coventry, UK
(Prof R J Lilford DSc,
O Oyebode PhD,
G J Melendez-Torres PhD,
Y-F Chen PhD, S I Watson PhD,
J Sartori BA); International
Institute for Environment and
Development, London, UK
(D Satterthwaite PhD); African
Population and Health
Research Centre, Manga Cl,
Nairobi, Kenya (B Mberu PhD,
T Haregu PhD, A Ezeh PhD);
School of Public Health,
University of Witwatersrand,
Johannesburg, South Africa
(A Ezeh); Global Urban
Observatory, Research and
Capacity Development Branch,
United Nations Human
Settlements Programme,
Nairobi, Kenya (R Ndugwa PhD);
School of Medicine, Federal
University of Minas Gerais,
Brazil (Prof W Caiaffa PhD);
United Nations University,
4. Kuala Lumpur, Malaysia
(Prof A Capon PhD); and
Oxford Policy Management,
New Delhi, India (R Saith PhD)
Correspondence to:
Richard J Lilford, Warwick Centre
for Applied Health Research and
Delivery, Warwick Medical
School, University of Warwick,
Coventry CV4 7AL, UK
[email protected]
Search strategy and selection criteria
To identify key literature for slum health, we did a systematic
overview of reviews of determinants of health in slum
settings and interventions that aim to improve the health of
people who live in slums. We also identifi ed randomised
controlled trials done in a slum setting as part of a
bibliometric analysis assessing the relative volume of research
studies concerning rural, urban, and slum settings (see
appendix p 3 in paper one). Acknowledging the important
roles that international, governmental, and
non-governmental organisations have in this area, we
systematically searched the grey literature and reviewed
relevant documents.
Key messages
• The neighbourhood eff ects in slums are likely to off er
economies of scale and increasing returns to investments
to create a healthy environment
• Although relocation and resettlement can be necessary for
safety reasons, slum upgrading in situ is usually preferable
to improve the health and welfare of people living in slums
5. • Sanitation, which started the public health revolution in
Europe and America during the 19th century, remains a
key neighbourhood challenge in slums
• Health services should be designed specifi cally to overcome
barriers to utilisation, such as distance and cost, for people
who live in slums
• Health services should be proactive in health protection—
eg, by immunisation and surveillance for childhood
malnutrition
• People who live in slums and their organisations should
have an active say in the prioritisation, design,
implementation, and evaluation of interventions in
slums
• Slum enumeration areas should be identifi ed in all census
listings and sampling frames to enable clearer
understanding of the neighbourhood eff ects of slums
• Enabled by this spatial construct, much more research is
needed on slum health and how to improve it, and a
greater proportion of this research should be based on
multicentre studies with contemporaneous controls
• Finally, we advocate the development of capacity for
research into slum health and the emergence of this as an
academic specialty
http://crossmark.crossref.org/dialog/?doi=10.1016/S0140-
6736(16)31848-7&domain=pdf
Series
6. 560 www.thelancet.com Vol 389 February 4, 2017
into account when interpreting the results of intervention
studies. For example, the eff ect of raising the fl oors
of slum dwelling to reduce contamination from the
surroundings may have a much smaller eff ect on rates of
childhood diarrhoea if water supply and sewage disposal
have been upgraded than if they have not.
And fi nally, the relationship between dose and response
must be considered. This relationship may be non-linear,
especially in dynamic scenarios where one person’s risk
aff ects another person’s risk, either because the disease
is infectious, or because one person’s behaviour
infl uences the health of others. In such a scenario,
increasing returns on investment are likely. An example
that we will discuss later concerns provision of sanitation
which is likely to exhibit increasing returns to scale as
faecal contamination is progressively reduced. Failure to
realise the steep part of the curve by supplying sanitation
at insuffi cient scale or intensity might explain why
many sanitation improvement projects have yielded
disappointing results and point the way for development
and evaluation of more intense interventions.
In fi gure 1, we model the ways that context and
dose-response correlations can interact.
Framework for review
We organised our analysis using a generic three level
causal model2,3 that has been applied in previous research
of slum upgrading4 and in a Cochrane Review of this
topic.5 Figure 2 shows these three levels. The fi rst or
macro-level is constituted of institutions and policies
7. aff ecting all citizens, including press freedom, an
independent judiciary, monetary and fi scal policy, and
other national or supranational infl uences. Second is the
middle or meso-level relating to slum specifi c policies.
These policies, such as those for land zoning and
provision of tenure, set the context where targeted
interventions, such as improved sanitation, play out. It is
therefore referred to as the enabling layer in the
Cochrane Review.5 And fi nally, the micro-level
encompassing interventions targeted at specifi c
problems such as faecal contamination of the
environment; referred to as the direct level in the
Cochrane Review.
We will not consider the fi rst (macro) level because it
concerns politics and economics and although these are
important infl uences on health, much can be done to
improve health pending an improved macro-economic
environment.7,8 Massive gains in health have been
recorded even in countries with poor national
governance9 and it is worth refl ecting that infant mortality
in slums is currently about 46 per 1000 livebirths,10
whereas in Victorian England (1837–1901) the upper class
infant mortality rate in 1899 was three times higher
(136 per 1000).11 The search strategy and selection criteria
panel shows how we searched for key literature on
interventions to improve slum health.
x1 x2 x3 T1
(before)
Intervention 1
x3→x2
T
2
9. Exposure
A
B
C
Δ1 Δ1
Δ2
Δ3
Δ3
Δ2
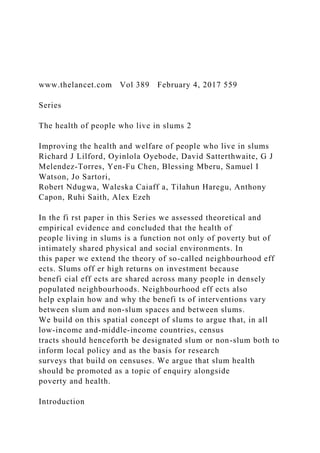
Figure 1: Hypothetical model of the association between
exposure to a risk factor for a disease of interest and prevalence
of the disease in three diff erent
neighbourhoods and observed eff ectiveness of an intervention
aimed at reducing a specifi c exposure, with success measured
by examination of prevalence
of the disease of interest
Δ=intervention eff ect. This model shows how interventions
designed to reduce the prevalence of a target disease will have
diff ering levels of eff ectiveness in diff erent
areas and within the same area over time, depending on the
conditions prevailing when the intervention is adopted, or
whether there is a suffi cient dose of the
intervention. The left hand panel depicts three diff erent dose
response curves. Line A shows an inelastic response where
increasing dose results in little change in
outcome. Line C represents a scenario where there is little
headroom for further improvement. Line B shows rapidly
10. increasing and then decreasing responses to dose.
The shape of the response curve can yield scenarios of
increasing returns to investment. The right hand panel shows
the wide range of possible intervention eff ects
that can be measured in a study depending on these factors. In A
and C, prevalence is quite inelastic over varying levels of
exposure, perhaps because another
powerful risk factor is present such as in A or because there is a
ceiling eff ect as prevalence is already low such as in C,
perhaps because the population has been
vaccinated against the risk factor. In B, the dose response is
non-linear so that an intervention might show increasing (and
then decreasing) returns to scale. For this
group, when an intervention is implemented that aims to reduce
exposure to the risk factor, the eff ects are small in
neighbourhoods A and C where this risk factor is
not the main determinant of disease. In B, the pre-intervention
exposure and the intervention dose have a crucial eff ect on the
intervention eff ectiveness because
of the non-linear dose response, so an intervention that reduces
the exposure from × 3 to × 2 has much less eff ectiveness than
an intervention that reduces the
exposure from × 2 to × 1.
Series
www.thelancet.com Vol 389 February 4, 2017 561
Meso-level policies directed at slums
Restriction of migration or benign neglect
Restriction of free movement of citizens within a country
is an illiberal policy reminiscent of apartheid
South Africa—we believe that the days of pass laws
should be consigned to history. The converse of
11. authoritarian restrictions on movement is a laissez-faire
policy of benign neglect. Proponents of this hands-off
policy adhere to modernisation principles, arguing
that slums are a temporary phenomenon, and that
intervening to improve the lives of people in slums is
self-defeating because it encourages inward migration—
the so-called Todaro eff ect.12 This argument can be
rejected because we have seen (paper one) that slums in
low-income and middle-income countries (LMICs) are
anything but temporary and continue to enlarge even
when economic growth is stagnant and that migration is
no longer the main driver of slum growth in many
countries—eg, 86% of people in South America already
live in urban centres.13
Resettlement and reallocation programmes
During the reign of Napoleon III in France (1852–70),
Baron Haussmann rebuilt central Paris, destroying the
medieval city but installing a massive sewerage system
and creating the current cityscape. Haussmann’s
intervention was not assessed scientifi cally but the
results of resettlement programmes in LMICs are often
disappointing.14–16 Sometimes this is because the
programmes are a covert form of expropriation when
rents on new buildings are unaff ordable for displaced
residents. Even when residents are resettled in alternative
accommodation, they are liable to fi nd themselves
ghettoised in the suburbs of cities, where land is cheap.
Commuting times are extended and in some instances
settlers return to their original settlement. Absent
development of infrastructure (eg, transport, water,
electricity, high quality housing, and sewerage) and the
cheaper policy of in-situ slum upgrading is generally
preferable to relocation.17 A lottery system enabling
people to move to better-off neighbourhoods that was
12. successful in the USA18 was not successful in India
largely because many residents returned to their original
location.19 Of course relocation is sometimes necessary
for the safety of residents, but should be done with as
much community assent as possible, high quality
housing must be provided, and mixed-income
destinations give rise to better outcomes than dense
areas of deprivation.18
Security of tenure
Many slums are informal settlements in which residents
do not have title or secure tenure. According to economic
theory, people are unlikely to invest in their properties
unless they feel secure against summary eviction,20 a
theory confi rmed empirically with respect to farm land.21
Further empirical support comes from two natural
experiments of providing tenure to slum residents,22,23
one in Peru that showed a sharp increase in investment
in home infrastructure, including sanitation, in the
intervention slums;22 and the second in Uruguay that
showed a signifi cant reduction in a score based on
number of reported illnesses.23 Title is maximally
eff ective when fi nancial systems that allow residents to
release collateral value exist (ie, when fi nancial systems
are in place to allow residents to borrow against the
collateral value in their homes).24 Furthermore, awarding
title might be a long-winded and expensive legal process.
In such cases, systems of tenure or registration that instil
confi dence that homes will not be bulldozed might be
enough to encourage residents to invest in developments
likely to promote health.25
Independent judiciary
Free press
13. Dispersion of law-making powers
Monetary and fiscal policies
International trade agreement
Limit migration and benign neglect
Resettlement and relocation
Tenure and title
City governance
Community engagement
Upgrading physical environment and
infrastructure (clean water, sewage
system, improved cooking stoves,
lighting, access roads, solid waste
management, home improvement)
Health/public health (health service
provision, health protection, health
improvement)
Educational interventions
Fostering individual economic stability
(eg, conditional cash transfers)
The general (macro-level) policy
environment
Policy environment for slums specifically
(meso-level; enabling level)*
14. Slum specific (micro-level; direct level)
interventions†
Outcomes
Health
Education
Productivity
and wealth
Human
wellbeing
Figure 2: Representation of causal pathways aff ecting the lives
of people who live in slums
*Topics under this heading were adapted from the framework in
the Cochrane Review5 augmented from the literature review.
†Topics under this heading were based
on the Social Determinants of Health, Offi ce of Disease
Prevention and Health Promotion.6 We do not discuss microfi
nance here because none of the three systematic
reviews evaluated this topic for slums specifi cally. We do not
cover education because this substantial topic is worthy of its
own review.
Series
562 www.thelancet.com Vol 389 February 4, 2017
Governance
Failures in planning and governance contribute to the
15. generation and maintenance of large slums,1 so good local
authority policies promulgated by the Healthy Cities
movement are conducive to slum health, as discussed in
the Lancet Commission on healthy cities in China.26 Local
government can help to ensure that land markets work
effi ciently and that the playing fi eld is not tilted in favour of
powerful elites wishing to build expensive houses for the
middle-class and that building restrictions do not price the
poorest people out of the market.27 Although such planning
processes can be corrupt or incompetent, leading to ghost
cities,28,29 they can also be successful (eg, in Porto Alegre
and Belo Horizonte in Brazil).30–32 Formalisation of slum
areas to provide rights and entitlements33 is associated with
improved education and health, and might partly explain
the results of a recent Indian study in which infant
mortality was 25 per 1000 livebirths on average in notifi ed
slums versus 58 per 1000 in a non-notifi ed slum in the
same city.34 However, only half of Indian slums are notifi ed,
and Chinese people who migrate to cities cannot gain
access to basic services without registration numbers
(Hukou).35 Access to amenities should not be made
contingent on tenure.36
Community engagement
There is an expanding literature confi rming the
eff ectiveness of interventions to promote local
engagement, action, and innovation,37,38 and the more the
community drives the intervention the greater the
eff ect.39 A systematic review40 of women’s groups to
improve perinatal outcomes included seven randomised
clinical trials. Although the results were positive overall,
most of these studies were done in rural settings and the
eff ect was highly dependent on participation rates.
Findings of the one study done in a slum showed a null
result probably because participation rates were low.41
This trial provides an example of an intervention that
16. might need to be modifi ed to take into account the
exigencies of slum life, perhaps by providing support
groups at places of work.
Several examples exist of successful grass-roots
networks in slums.39,42–45 The programme in Porto Alegre,
Brazil, incorporated participatory budgeting in which
communities were included in setting priorities.30,46 Such
groups have provided important help for women in
labour in Nairobi slums, in Kenya,47 enhanced protection
for sex workers in Zimbabwe,48 and improved self-
organisation of waste pickers in slums who have gone on
to bid successfully for municipal contracts.49 City and
national slum dwellers federations have been active in
conducting slum surveys using these to provoke and
plan action with local authorities.50
Specifi c (micro-level) interventions in slums
Here we discuss specifi c physical and engineering
approaches to slum upgrading and service development
(fi gure 2). We augment the few studies done specifi cally
in slums with studies that cover slums and other areas;
the systematic reviews we rely on are listed in the
appendix pp 5–7).
Physical and engineering approaches in slum upgrading
Water and sanitation
The poor quality of water and inadequate sanitation in
slums and the resulting high incidence of diarrhoea,
especially in children younger than 5 years, was
documented in paper one.1 The problem can be tackled
with behavioural interventions or physical interventions.
Physical interventions can be targeted at water provision,
sanitation, and point of use methods to decontaminate
water (eg, fi lters). A Cochrane Review5 of physical and
17. engineering interventions (appendix p 7) in slums cited
three main studies that satisfi ed its quality threshold and
included a health outcome. In one of these studies51
investigators noted reduced incidence of diarrhoea in
households connected to a water supply but confi dence
intervals were wide (risk ratio [RR] 0·53; 95% CI
0·27–1·04). A multi-component intervention52 that
included piped water in homes and lavatories connected
to a sewer along with street paving and drainage reported
a substantial reduction in waterborne diseases (RR 0·64;
0·27–0·98). Finally, a study of improved water and
sanitation53 that looked only at eff ect on sanitation-
related mortality reported no change (RR and CIs not
given). The appendix (pp 1–4) provides results for case
studies based in slums. Another important study54 that
was not specifi c to slums used the Demographic Health
Survey to analyse data from 70 countries and noted
reductions in the incidence of diarrhoea of 13% and 7%,
respectively, for improved water and sanitation.55
Therefore, the eff ect sizes recorded in the mentioned
studies are highly variable and some are disappointing
in view of the theoretical headroom for improvement
and the results credited to the 19th century sanitary
revolution in Europe and North America. A plausible
explanation for these eff ect sizes can be found in the
analysis of context and increasing returns to scale
(fi gure 1).
Wolf and colleagues56 provide a classifi cation of
intervention water comprehensiveness, a proxy for dose.
Water provision can be improved (according to the
United Nations [UN] defi nition) by making it readily
available from standpipes outside the house, or it can be
piped into the home, or piped and quality assured.
Likewise, sanitation can be improved by providing pit
latrines or it can be extended to include sewer
18. connections. The literature on slums specifi cally is
insuffi cient to further examine the role of dose and we
therefore turned to systematic reviews on water and
sanitation interventions generally (ie, including but not
restricted to slums).56–58 Results show increasing returns
to comprehensiveness (ie, dose) of the intervention
(appendix pp 1–2 and fi gure 3), conforming to the
See Online for appendix
Series
www.thelancet.com Vol 389 February 4, 2017 563
theoretical representation in fi gure 1. Although the UN
classifi es pit latrines as improved sanitation, these
fi ndings suggest that they are of minimal eff ectiveness.
Furthermore, some researchers have reported that they
do little to reduce environmental contamination in
congested slum neighbourhoods.59 When adequately
quality assured piped water cannot be provided, point of
use methods provide an alternative since the above
systematic reviews consistently show substantial eff ect
sizes (relative risk 0·65, 95% CI 0·48–0·88) in Fewtrell’s
review58 and 0·55 (0·38–0·81) for fi ltered and safely
stored water in Wolf’s review.56
Eff ectiveness is probably aff ected by contextual factors
as well as dose. For example, eff ectiveness will be
attenuated if people do not make use of facilities; the
likely explanation for null results in two recent cluster
randomised clinical trials of making pit latrines
available in India.60,61 A further reason for variable
results from physical interventions could be poor
19. maintenance of facilities and inadequate installations;
piped water distribution systems are often
contaminated.59 It might be expected that combining
sanitation and water interventions would be more
eff ective than either alone, but this remains unproven
(appendix pp 1–4).
Home improvements
The Cochrane review of slum interventions identifi ed a
natural experiment62 in Mexico in which the provision of
a cement fl oor reduced the incidence of diarrhoea in
children younger than 6 years (RR 0·87, 0·76–1·00).
Findings of a subsequent experimental study63 done in
El Salvador, Mexico, and Uruguay that assessed home
improvements including a raised fl oor also showed
a signifi cant reduction in diarrhoea incidence
(2·7% absolute risk reduction from 15·1%) if Uruguay,
which had low rates at baseline, is excluded from the
analysis.
Lighting, repaving, and garbage removal
Improved street lighting and paving have been strongly
recommended by UN-Habitat on the basis of observational
studies but the one randomised clinical trial in the
Cochrane Review4 did not confi rm improved security or
health.64 Removal of solid waste is undoubtedly a good
idea in view of its eff ects on health and wellbeing,1 but
little evidence was found on how best to dispose of garbage
or on the health benefi ts of doing so.
Taken together, the literature provides several case
studies of interventions but very few large-scale studies
in which in-depth fi ndings complement comparisons
across sites, such as can be found, for example, in studies
of home improvements in high-income countries.65
20. Health and public services
Several health improvement studies have been done
in general populations but also replicated in slums
specifi cally. First, results of a meta-analysis of 11 studies
across urban and rural locations showed that
behavioural interventions to promote handwashing
resulted in a lower prevalence of diarrhoea,58 and this
was also shown in trials specifi cally in slums in
Pakistan66 and Nepal.67 Second, a systematic review
looking at paediatric burn prevention identifi ed
30 studies from high-income and low-income countries
(appendix p 6). The benefi ts of reducing hazards such as
unsafe paraffi n cook-stoves were replicated in a
randomised clinical trial in a slum environment (in
South Africa).68 Finally, a systematic review69 of
behaviour change interventions to reduce indoor
pollution across 20 countries reported that these could
result in an 88% fall in indoor particulate levels
(13·2–1·6 parts per million), a 21% reduction in
respiratory disease (absolute risk not given) and savings
on fuel costs. Two of the interventions were conducted
in slums (Bangladesh and Uganda), but results are not
broken down by location.
Many individual randomised clinical trials of health
promotion interventions have been done specifi cally in
slums (appendix pp 8, 9) yielding positive results
concerning behavioural interventions to reduce obesity
in women and children in Brazil,70,71 childhood
malnutrition in Peru,72 breastfeeding in Kenya,67 and
so-called delinquent behaviour in Uganda.73 Provision of
fortifi ed snack bars resulted in improved nutritional
status in India74 and Bangladesh75 (arguably avoiding the
Level 3 Level 2 Level 1 Baseline¶
22. Water
(mixed slum
and non-slum)†
Sanitation
(mixed slum
and non-slum)†
DHS (sanitation)‡
DHS (water)‡
Figure 3: Representation of magnitude of eff ect by
comprehensiveness of
intervention across studies in slum and non-slum systematic
reviews and
the DHS
DHS=Demographic and Health Surveys. *Relative risk ratio for
episodes of
diarrhoea or waterborne disease in the Cochrane review5 of
interventions in
slums. †Wolf’s review.56 ‡DHS study.54 §Butala and
colleagues, 2010.52
¶Water: level 1=improved supply of piped water into vicinity of
homes; level
2=piped into home; level 3=piped into home and quality
assured. Sanitation:
level 1=improved (pit latrine); level 3=pit latrine connected to
sewage system.
This classifi cation is based on Wolf and colleagues, 2014.56
Series
23. 564 www.thelancet.com Vol 389 February 4, 2017
harmful eff ects resulting from imbalance of competing
elements—eg, zinc and copper, with chemical
formulations of micro-nutrients).
Taken together, these results support the theory that
slum populations benefi t from health promotion
measures as long as they receive them. This conclusion,
that access is the rate-limiting step to achieving benefi t
for people who live in slums, seems to also apply to
health protection. Child immunisation is regarded as
the most cost-eff ective intervention for health in
LMICs,76 yet children in slums are less likely to be
vaccinated than other urban infants.77 This situation is
especially unjust because slums are often used as a
convenient sample in vaccine trials (appendix p 4 in
paper one). In terms of screening, we are unaware of
studies specifi c to slums, but rates are very low across
low-income countries; 4·1% and 2·2%78 in the relevant
populations for cervical and breast cancer respectively,
for example. However, slum populations benefi t when
access to health protection is provided. For example,
results of fi ve randomised clinical trials done in
slums79–83 showed that parasite loads can be reduced by
treatment targeted at high risk groups and some showed
improved child growth (although the latter is a highly
contested topic across all populations).84
The problem with clinical services is also one of
access on the assumption that indications for treatment
do not change because a person lives in a slum. The
unifying theme across health provision of all types in
slums is the need to improve access. Services need to
be available outside normal offi ce hours and be pro-
24. active for the reasons listed in paper one related to
determinants of health. Such services include a
judicious and comprehensive mix of community health
workers, local clinics, and use of mobile technology to
ensure coverage with respect to health protection,
health improvement, and clinical services. A recent
paper85 in the Lancet Series on universal healthcare,
markets, profi t and the public good noted that providing
a network of accessible free clinics crowded out low
quality, under-qualifi ed providers. Further work to
design services that meet local preferences86 is urgently
required and we note that high population densities
allow many people to be reached per unit of staff time;
another potential example of increased economies to
scale when intervening at the neighbourhood level in
slums. In the table we summarise the literature on the
likely eff ectiveness of both enabling (meso-level) and
specifi c (micro-level) interventions.
Recommendations for policy and research
In paper one, we noted that very little research has been
devoted to the subject of slum health. Consequently,
despite nearly 1 billion people already living in slum
locations in LMICs, we do not understand enough about
their health vulnerabilities and what eff ect slum-focused
health interventions could have. In particular, we need
to understand how neighbourhood eff ects operate so
that we can get the intensity of interventions right
(fi gure 1).
Identifi cation and study of slums as spatial entities
Although slums are easily identifi able physically in
many cities in LMICs, they remain invisible in many
data systems that drive research and policy. Slums are
rarely identifi ed in national censuses, which form the
sampling frames for national surveys. We recommend
25. that all censuses include identifi cation for slum and
non-slum clusters for all urban areas. This inclusion will
encourage all studies and national surveys to generate
separate health indicators for slum and non-slum areas
both for research purposes and to identify local priorities
for action—eg, to establish where diarrhoea and stunting
are most prevalent. As we have seen repeatedly in this
Series, most research provides data for urban areas as a
whole. Such data are of limited value; for example, if
slums have worse outcomes than non-slum urban areas
and the slum population (as a proportion of urban
population), has been changing, then urban trend
indicators may represent nothing more than diff erences
Aim Eff ect
Meso-level (enabling policies)
Limit free
movement
Discourage growth of slums Does not solve underlying problem,
illiberal, and is
not a permanent solution
Benign neglect Limit size of slums on the
grounds that they are self-
correcting
Leaves vulnerable people in prolonged and severe
need and generates poverty traps; too late for
many countries where urbanisation is already
advanced
Relocation and
resettlement
26. Clear slums and provide
alternative, improved living
environment
Countries with large slums generally have
insuffi cient resources or lack political will to do a
proper job, and provide necessary infrastructure;
this approach often promises more than it delivers
Title and tenure Encourage in-situ regeneration
by giving people a stake in their
community and homes
Providing title is eff ective but might not be
possible where title is disputed; security of tenure
without title might be suffi cient
City governance Recognising slums and
conferring rights creates
conditions conducive to
health; land zoning protects
vulnerable citizens
Many examples of good and bad practice;
providing rights and services is an eff ective policy
Community
engagement and
empowerment
Uses assets of the community;
empowers citizens
Many empirical examples of success; most
eff ective when citizens are genuinely empowered
27. Specifi c (micro-level) interventions
Physical methods of
slum improvement
Uncontaminated water piped
into homes and point of use
decontamination; reduces
environmental contamination
through sanitation
Dose-dependent eff ect; pit latrines have very small
benefi t especially in slums; point of use methods
of decontamination eff ective where clean tap
water not provided
Home and
environment
Improve home insulation, street
paving, lighting and drainage;
garbage removal
Sensible measures for reasons given in paper one1
but poorly studied in slum contexts
Health services Improve access to health
protection, health
improvement, and clinical care
Public health and clinical services eff ective in
slums as elsewhere, barriers to access have been
studied,1 but the most cost-eff ective mix of
services is in need of urgent study
28. Table: Summary of intervention eff ectiveness across both
meso-level and micro-level interventions
Series
www.thelancet.com Vol 389 February 4, 2017 565
in the respective growth rates of slum versus non-slum
urban populations.
All measures of place of residence should move from a
binary urban–rural construct to one that splits urban into
slum and non-slum (panel). Pending implementation of
the recommended changes to include identifi cation of
slums in censuses, individual researchers can estimate
the locations of high risk areas using geo-located data.
We illustrate this idea by mapping the prevalence of
diarrhoea and stunting in children to well-known slums
in three urban areas in Nairobi, Kenya, Port-au-Prince,
Haiti, and Lagos, Nigeria using data from the
Demographic Health Survey in fi gure 4. There is
clustering of cases in the vicinity of well known slums
but precision would be much improved if slum areas
were clearly demarcated.
Child health
Although the evidence base in slum health is
underdeveloped, some recommendations for
improvement can be made. In particular, the evidence in
paper one highlighted the plight of children who are
exposed to high risk of infection while their immune
systems are immature. Children are also a priority
because conditions at the start of life will limit their
subsequent life chances. Interventions that should be
29. considered, contingent on local circumstances, include:
improved uptake of vaccination; promotion of
breastfeeding, nutrition, clean water, and sanitation; and
indoor protection against burns, and inhalation of
particles and noxious fumes. As they grow into young
adulthood, violent crime is a big challenge, although
we need to better understand how supportive and
destructive neighbourhood cultures develop and hence
how interventions can help.
Sanitation and water quality
Improvements in water supply and sanitation have
yielded modest health benefi ts in modern slums by
comparison with the massive eff ects credited to the
major works carried out in European and
North American cities during the so-called sanitary
awakening in the 19th century.55 We speculate that there
is a straightforward reason for this which turns on the
issue of increasing returns to scale described in the
introduction; most interventions have simply not
achieved their aims. Piped water installations have
been prone to contamination, and sanitation has
removed insuffi cient waste to reduce faecal
contamination of the environment to the tipping point
where rapidly increasing returns to scale might be
achieved (fi gure 1). The international community might
even have exacerbated the problem by setting standards
for improved sanitation (eg, pit latrines) that are
unsuitable for densely crowded slum conditions.50
Therefore, we recommend that this inadequate
standard should be withdrawn for slum contexts and
that, working with local communities, comprehensive
installations (eg, linked to a sewerage system) should
be installed as a matter of urgency within the framework
of robust large-scale comparative studies to work out
30. which types of installation are suitable for which types
of slum environment.
The art of the possible in slum improvement
If some standards are set too low, others might be too
high. It has become fashionable for scholars to argue that
the whole slum nexus should be tackled in a coordinated
way.87–89 At the limit, such an approach amounts to a
programme to convert slum to non-slum. Although this
is a laudable aim, we are concerned that the ideal should
not become the enemy of the good; as Buckley90 has
argued, cost-eff ective interventions, such as vaccination
and installing sanitation systems, should not wait until
the moment is propitious for a holistic strategy, and
access to amenities should not be dependent on title or
tenure.91 We also caution that reliance on community
assets should not be taken too far; work in rural areas
shows that the greatest potential health and wellbeing
gains are among those most deeply trapped in poverty
and hence most in need of outside help.92,93
Panel: Suggested process to identify slums for inclusion
in censuses
To identify slums and include them in censuses so that
studies and surveys based on a census sampling frame can
distinguish between slum and non-slum locations, the
following are necessary: fi rst, enumeration areas should be
designated (ie, tagged) to one of three categories (slum,
non-slum, or rural) in such a way that no one urban
enumeration area straddles slum and non-slum areas;
second, while nations classify slums according to their own
context, their methods should be transparent, and should
consider the fi ve household level criteria in the UN-Habitat
defi nition; and fi nally, quality assurance should check that all
clusters are enumerated and then that all dwellings are
31. recorded within each cluster. This approach will ensure all
national surveys and data systems can eff ectively sample and
report indicators using three residential domains: rural, urban
slum, and urban non-slum. Some countries, notably Kenya
and Bangladesh, already follow a process to identify slum
enumeration areas and include identifi cation of slum and
non-slum clusters in national master sampling frames. This is
why these countries were selected for the study in paper one.
It would be impossible (or at least it would take a very long
time) to negotiate a common defi nition of a slum across all
countries and, in any case, a common defi nition is not a
prerequisite for examination of the proposed spatial
construct of slum health. The subject can develop,
notwithstanding diff erences in defi nitions, just as the topic of
urban health has developed despite diff erent national
defi nitions of an urban area.
Series
566 www.thelancet.com Vol 389 February 4, 2017
Nairobi, Kenya
Diarrhoea, children aged <5 years Childhood stunting
Port-au-Prince, Haiti
Lagos, Nigeria
A A
C C
33. Series
www.thelancet.com Vol 389 February 4, 2017 567
A call for multicentre studies with contemporaneous
controls
The literature on policy interventions and on physical
upgrading of slums is based largely on case studies. We
do not wish to disparage such studies, but we advocate
balancing the literature with a greater proportion of
studies with contemporaneous controls.94,95 While not
reifying experimental methods, Field and Kremer cite
empirical evidence that supports theoretical arguments
for use of experimental methods in a slum context.96–98
Consideration of several outcomes and populations
The eff ects of policy and service are often broad; they
spill over to aff ect outcomes diff erent to the original
target. For instance, improving water and sanitation
has benefi cial eff ects on education, wellbeing, and
productivity in addition to those on health (appendix
pp 1–3). A corollary is the importance of capturing both
dimensions of health (eg, disability-adjusted life-years)
and of subjective wellbeing (eg, happiness, life
satisfaction, and mental health). Special attention should
be paid to groups who are marginalised or especially
vulnerable,99 and cost-eff ectiveness analyses should seek
to examine dimensions of equity, particularly catastrophic
out-of-pocket expenses, and proportions of people
pushed below the poverty line (US$2 per day at
purchasing power parity).100
Slum health as an academic discipline
34. This Series has been predicated on the idea that there is
merit in abstracting the idea of slum health from that of
poverty in general or urban health in particular. In view
of the importance of space, and the massive scale of
modern slums, we think there is a need for a subject
dedicated to improving conditions in slums. We identify
four groups of people who can promote this cause: those
who control the purse strings, those who control the
intervention, those whose lives are at stake, and those
who have experience and expertise in the design,
conduct, and reporting of academic studies.
Organisations that promulgate interventions across
jurisdictions, such as the World Bank, agencies of the
UN, and major donors, are in a good position to exert
both the necessary leadership and provide practical
support to kick-start a community of practice across the
above four groups. Multidisciplinary research
collaboration will be needed to make progress in
improving slum health.
Conclusion
While it is no longer true to say that people who live in
slums are invisible, they are insuffi ciently visible and as
a result continue to be marginalised. Many slums are
not identifi ed in national surveys based on census
sampling frames; research eff ort in slums is
incommensurate with the size of the issue (especially
with respect to multicentre controlled studies); people
who live in slums remain politically weak and subject
to expropriation; and conditions in slums are improving
only slowly. The profi le of slum health and welfare
needs to be raised, and the time to do so is propitious in
view of the forthcoming UN-Habitat III conference, the
third of its type in 40 years, and the fi rst UN global
summit after the adoption of the 2030 Agenda for
35. Sustainable Development and the Sustainable
Development Goals. The time is ripe to revisit the
Urban Agenda with a strong emphasis on slum health
and slum upgrading and on strengthening the
capacities of urban governments to work with people
who live in slums to act on these. This will help in
securing commitments to ensure that policies are
backed up with adequate fi nance. Above all, we advocate
the academic development of slum health in the form
of a partnership between policy makers, academics,
and representatives of those who live in slums, so that
knowledge can grow in tandem with eff orts to improve
health and wellbeing.
The supposed neighbourhood eff ect in slums is both a
problem and an opportunity. It is a problem because it
is likely to amplify health hazards and it is an
opportunity because one intervention can sim
ultaneously improve so many lives in one densely
packed community. It is time for a concerted eff ort to
generate political momentum and bear down heavily on
known threats to health and wellbeing in slums.
Because young children are especially vulnerable in
slums, and because the eff ects of chronic illnesses are
indelible, we recommend a concerted and sustained
international movement to provide eff ective
interventions to improve child health such as
vaccinations, water and sanitation, breastfeeding and
nutrition, and safe non-polluting cook stoves.
Contributors
This Series on slum health has been an international
collaboration led
by the University of Warwick, African Population and Health
Research
Centre, United Nations Human Settlements Programme (UN-
Habitat),
36. International Institute for Environment and Development,
United
Nations University, Federal University of Minas Gerais, and
Oxford
Policy Management Institute. RJL and AE jointly
conceptualised the
intellectual framework and initial draft of this report. GJM-T,
JS, SIW,
and Y-FC conducted the systematic reviews and OO led on the
health
aspects. All authors provided references and material and
contributed
actively to the drafting and reviewing of the report.
Declaration of interests
We declare no competing interests.
Acknowledgments
The authors thank Aileen Clarke, Christine MacArthur, Trevor
Hancock,
and Trudy Harpham for their useful review comments during the
writing process; and Peter Chilton for his help with references,
and
preparing the fi gures and manuscript for publication. RJL and
OO are
supported by the National Institute for Health Research (NIHR)
Collaborations for Leadership in Applied Health Research and
Care
(CLAHRC) West Midlands initiative. WC is supported by the
Brazilian
National Council for Scientifi c and Technological Development
(CNPq).
The African Population and Health Research Centre (APHRC)
team are
supported in part from core support grants from the Hewlett
Foundation, the Swedish International Development
37. Cooperation
Agency (Sida), and an anonymous funder. This paper presents
Series
568 www.thelancet.com Vol 389 February 4, 2017
independent research and the views expressed are those of the
authors
and not necessarily those of the funding sources, the National
Health
Service (NHS), or the UK Department of Health.
References
1 Ezeh A, Oyebode O, Satterthwaite D, et al. The history,
geography,
and sociology of slums and the health problems of people who
live
in slums. Lancet 2016; published online Oct 13. http://dx.doi.
org/10.1016/S0140-6736(16)31650-6.
2 Lilford RJ, Chilton PJ, Hemming K, Girling AJ, Taylor CA,
Barach P. Evaluating policy and service interventions:
framework to
guide selection and interpretation of study end points. BMJ
2010;
341: c4413.
3 Donabedian A. Explorations in Quality Assessment and
Monitoring, Volume I: The Defi nition of Quality and
Approaches
to Its Assessment. Ann Arbor, MI: Health Administration Press,
1980.
38. 4 Hardoy JE, Cairncross S, Satterthwaite D. The Poor Die
Young:
Housing and Health in Third World Cities. London:
Earthscan Publications, 1990.
5 Turley R, Saith R, Bhan N, Rehfuess E, Carter B. Slum
upgrading
strategies involving physical environment and infrastructure
interventions and their eff ects on health and socio-economic
outcomes. Cochrane Database Syst Rev 2013; 1: CD010067.
6 Offi ce of Disease Prevention and Health Promotion.
Social Determinants of Health. 2016.
https://www.healthypeople.
gov/2020/topics-objectives/topic/social-determinants-of-health
(accessed Feb 17, 2016).
7 Baker J. Urban Poverty: A Global View. Washington, DC: The
World
Bank, 2008.
8 Abuya B, Kassahun A, Ngware M, Onsomu E, Oketch M.
Free primary education and implementation in Kenya: the role
of
primary school teachers in addressing the policy gap.
SAGE Open 2015: 1–10.
9 WHO. World Health Statistics. Geneva: World Health
Organization,
2015.
10 Kyu HH, Shannon HS, Georgiades K, Boyle MH. Association
of
urban slum residency with infant mortality and child stunting in
low and middle income countries. BioMed Res Int 2013; 2013:
39. 1–12.
11 Mitchell S. Victorian Britain Encyclopedia. New York:
Garland
Publishing, 1988.
12 Harris JR, Todaro MP. Migration, unemployment and
development: a two-sector analysis. Am Econ Rev 1970; 60:
126–42.
13 UN-Habitat. World Cities Report 2016: Urbanization and
Development Emerging Futures. Nairobi, Kenya: UN–Habitat,
2016.
14 Xavier HN, Magalhães F. Urban slums report: The case of
Rio de Janeiro. London: University College London, 2003.
15 Bradlow B, Bolnick J, Shearing C. Housing, institutions,
money:
the failures and promise of human settlements policy and
practice
in South Africa. Environ Urban 2011; 3: 267–75.
16 Kapse V, Pofale A, Mathur M. Paradigm of relocation of
urban poor
habitats (slums): case study of Nagpur city.
Int J Soc Behav Educ Econ Bus Ind Eng 2012; 6: 2916–23.
17 Collins W, Shester KL. Slum clearance and urban renewal in
the
United States. Am Econ J: Appl Econ 2013; 5: 239–73.
18 Chetty R, Hendren N, Katz L. The eff ects of exposure to
better
neighbourhoods on children: new evidence from the moving to
opportunity experiment. Am Econ Rev 2016; 106: 855–902.
40. 19 Barnhardt S, Field E, Pande R. Moving to opportunity or
isolation?
Network eff ects of a randomised housing lottery in urban India.
NBER working paper 21419. Massachusetts: National Bureau of
Economics, 2015.
20 Patel SB. Dharavi: makeover or takeover? Econ Polit
Weekly 2010;
45: 47–54.
21 Banerjee A, Gertler P, Ghatak M. Empowerment and effi
ciency:
tenancy reform in west Bengal. J Polit Econ 2002; 110: 239–80.
22 Field E. Property rights and investment in urban slums.
J Eur Econ Assoc 2005; 3: 279–90.
23 Gandelman N. Property rights and chronic diseases: evidence
from
a natural experiment in Montevideo, Uruguay 1990–2006.
Econ Hum Biol 2010; 8: 159–67.
24 Buckley RM, Kalarickal J. Housing Policy in Developing
Countries:
Conjectures and Refutations. Oxford: Oxford University Press,
2005.
25 Handzic K. Is legalized land tenure necessary in slum
upgrading?
Learning from Rio’s land tenure policies in the Favela Bairro
Program. Habitat Int 2010; 34: 11–17.
26 Rydin Y, Bleahu A, Davies M, et al. Shaping cities for
health:
complexity and the planning of urban environments in the
41. 21st century. Lancet 2012; 379: 2079–108.
27 Muller A, Mitlin D. Securing inclusion: strategies for
community
empowerment and state redistribution. Environ Urban 2007;
19: 425–39.
28 Njoku J. Why Festac, Shagari housing schemes failed
29th April 2014. http://www.vanguardngr.com/2014/04/festac-
shagari-housing-schemes-failed-expert/ (accessed March 4,
2016).
29 Etim EE, Atser J, Akpabio F. The new social housing scheme
in
Nigeria: how benefi cial for the less privileged? Glob J Soc Sci
2007;
6: 1–6.
30 Vlahov D, Caiaff a WT. Healthy urban governance and
population
health. Participatory budgeting in Belo Horizonte, Brazil.
In: Sclar ED, Volavka-Close N, Brown P, eds. The urban
transformation: health, shelter and climate change. London:
Taylor & Francis, 2013: 63–81.
31 Viero OM, Cordeiro AP. New Rules, New Roles: Does PSP
Benefi t
the Poor? The Case for Public Provisioning in Pôrto Alegre.
Pôrto Alegre: Wateraid, 2003.
32 Goldsmith WW, Vainer CB. Participatory budgeting and
power politics
in Porto Alegre. Land Lines 2001; 13: 1.
33 Wang F, Xuejin Z. Inside China’s cities: institutional
barriers and
42. opportunities for urban migrants. Am Econ Rev 1999; 89: 276–
80.
34 Subbaraman R, O’Brien J, Shitole T, et al. Off the map: the
health
and social implications of being a non-notifi ed slum in India.
Environ Urban 2012; 24: 643–63.
35 Qiu P, Yang Y, Zhang J, Ma X. Rural-to-urban migration
and its
implication for new cooperative medical scheme coverage and
utilization in China. BMC Public Health 2011; 11: 520.
36 Mudege NN, Zulu EM. Discourses of illegality and
exclusion:
when water access matters. Glob Public Health 2011; 6: 221–33.
37 Brunton G, Caird J, Stokes G, et al. Review 1: Community
engagement for health via coalitions, collaborations and
partnerships: a systematic review. London: EPPI Centre UCL,
2015.
38 Cyril S, Smith BJ, Possamai-Inesedy A, Renzaho AM.
Exploring the
role of community engagement in improving the health of
disadvantaged populations: a systematic review.
Glob Health Act 2015; 8: 29842.
39 Rosato M. A framework and methodology for diff
erentiating
community intervention forms in global health.
Community Dev J 2015; 50: 244–63.
40 Prost A, Colbourn T, Seward N, et al. Women’s groups
practising
participatory learning and action to improve maternal and
43. newborn
health in low-resource settings: a systematic review and
meta-analysis. Lancet 2013; 381: 1736–46.
41 More NS, Bapat U, Das S, et al. Community mobilization in
Mumbai slums to improve perinatal care and outcomes: a cluster
randomized controlled trial. PLoS Med 2012; 9: e1001257.
42 Dias S. Overview of Legal Framework for Social Inclusion
in Solid
Waste Management in Brazil. Cambridge, USA: WIEGO, 2010.
43 Chen M, Vanek J, Lund F, Heintz J, Jhabvala R, Bonner C.
Progress of the World’s Women 2005: Women, Work and
Poverty:
United Nations Develeopment Fund for Women (UNIFEM).
New York: United Nations, 2005.
44 Chen M, Jhabvala R, Kanbur R, Richards C. Membership
based
organisations of the poor. London: Routledge, 2007.
45 Chen M, Snodgrass D. Managing resources, activities, and
risk in
urban India: The impact of SEWA Bank. Washington, DC:
AIMS,
2001.
46 Cabannes Y. The impact of participatory budgeting on basic
services; municipal practices and evidence from the fi eld.
Environ Urban 2015; 27: 257–84.
47 Bakibinga P, Ettarh R, Ziraba AK, et al. The eff ect of
enhanced
public–private partnerships on maternal, newborn and child
health services and outcomes in Nairobi-Kenya: the
44. PAMANECH
quasi-experimental research protocol. BMJ Open 2014;
4: e006608.
Series
www.thelancet.com Vol 389 February 4, 2017 569
48 Kerrigan D, Kennedy CE, Morgan-Thomas R, et al. A
community
empowerment approach to the HIV response among sex
workers:
eff ectiveness, challenges, and considerations for
implementation
and scale-up. Lancet 2015; 385: 172–85.
49 Fergutz O, Dias S, Mitlin D. Developing urban waste
management
in Brazil with waste picker organizations. Environ Urban 2011;
23: 597–608.
50 Patel S, Baptist C. Documenting by the undocumented.
Environ Urban 2012; 24: 3–12.
51 Galiani S, Gonzalez-Rozada M, Schargrodsky E. Water
expansions
in Shantytowns: Health and Savings. Washington DC:
Inter-American Development Bank, 2007.
52 Butala NM, VanRooyen MJ, Patel RB. Improved health
outcomes in
urban slums through infrastructure upgrading. Soc Sci Med
2010;
71: 935–40.
45. 53 Soares F, Soares Y. The socio-economic impact of Favela–
Bairro.
What do the data say? Washington DC: Inter-American
Development Bank, 2005.
54 Gunther I, Gunther F. Water, sanitation and children’s
health:
evidence from 172 DHS surveys. Policy Research working paper
WPS 5275. Washington, DC: The World Bank, 2010.
55 Chaplin SE. Cities, sewers and poverty: India’s politics of
sanitation.
Environ Urban 1999; 11: 145–58.
56 Wolf J, Prüss-Ustün A, Cumming O, et al. Assessing the
impact of
drinking water and sanitation on diarrhoeal disease in low- and
middle-income settings: systematic review and meta-regression.
Trop Med Int Health 2014; 19: 928–42.
57 Clasen TF, Bostoen K, Schmidt WP, et al. Interventions to
improve
disposal of human excreta for preventing diarrhoea.
Cochrane Database Syst Rev 2010; 6: CD007180.
58 Fewtrell L, Kaufmann RB, Kay D, Enanoria W, Haller L,
Colford JM,
Jr. Water, sanitation, and hygiene interventions to reduce
diarrhoea
in less developed countries: a systematic review and meta-
analysis.
Lancet Infect Dis 2005; 5: 42–52.
59 Nakagiri A, Niwagaba CB, Nyenje PM, Kulabako RN,
Tumuhairwe JB, Kansiime F. Are pit latrines in urban areas of
46. sub-Saharan Africa performing? A review of usage, fi lling,
insects
and odour nuisances. BMC Public Health 2016; 16: 120.
60 Clasen T, Boisson S, Routray P, et al. Eff ectiveness of a
rural
sanitation programme on diarrhoea, soil-transmitted helminth
infection, and child malnutrition in Odisha, India:
a cluster-randomised trial. Lancet Glob Health 2014; 2: e645–
53.
61 Patil SR, Arnold BF, Salvatore AL, et al. The eff ect of
India’s total
sanitation campaign on defecation behaviors and child health in
rural Madhya Pradesh: a cluster randomized controlled trial.
PLoS Med 2014; 11: e1001709.
62 Cattaneo M, Galiani S, Gertler P, Martinez S, Titiunik R.
Housing, Health and Happiness. Am Econ J: Econ Policy 2009;
1: 75–105.
63 Galiani S, Gertler P, Cooper R, Martinez S, Ross A,
Undurraga R.
Shelter from the storm: upgrading housing infrastructure in
Latin American slums. Working Paper 19322. Cambridge, MA:
National Bureau of Economics, 2013.
64 Gonzalez-Navarro M, Quintana-Domeque C. Urban
infrastructure
and economic development: experimental evidence from street
pavement. IZA discussion paper No. 5346. Germany, 2010.
65 Thomson H, Thomas S, Sellstrom E, Petticrew M. Housing
improvements for health and associated socio-economic
outcomes.
Cochrane Database Syst Rev 2013; 2: CD008657.
47. 66 Bowen A, Agboatwalla M, Luby S, Tobery T, Ayers T,
Hoekstra RM.
Association between intensive handwashing promotion and
child
development in Karachi, Pakistan: a cluster randomized
controlled
trial. Arch Pediatr Adolesc Med 2012; 166: 1037–44.
67 Ernst KC, Phillips BS, Duncan BD. Slums are not places for
children to live: vulnerabilities, health outcomes, and possible
interventions. Adv Pediatr 2013; 60: 53–87.
68 Parbhoo A, Louw QA, Grimmer–Somers K. Burn prevention
programs for children in developing countries require urgent
attention: a targeted literature review. Burns 2010; 36: 164–75.
69 Goodwin NJ, O’Farrell SE, Jagoe K, et al. Use of behavior
change
techniques in clean cooking interventions: a review of the
evidence and scorecard of eff ectiveness. J Health Commu 2015;
20: 43–54.
70 Alves JG, Gale CR, Souza E, Batty GD. Eff ect of physical
exercise on
bodyweight in overweight children: a randomized controlled
trial in
a Brazilian slum. Cad Saude Publica 2008; 24: S353–59.
71 Alves JG, Gale CR, Mutrie N, Correia JB, Batty GD. A 6-
month
exercise intervention among inactive and overweight favela-
residing
women in Brazil: the Caranguejo Exercise Trial.
Am J Public Health 2009; 99: 76–80.
48. 72 Penny ME, Creed-Kanashiro HM, Robert RC, Narro MR,
Caulfi eld LE, Black RE. Eff ectiveness of an educational
intervention
delivered through the health services to improve nutrition in
young
children: a cluster-randomised controlled trial. Lancet 2005;
365: 1863–72.
73 Rotheram-Borus MJ, Lightfoot M, Kasirye R, Desmond K.
Vocational training with HIV prevention for Ugandan youth.
AIDS Behav 2012; 16: 1133–37.
74 Kehoe SH, Chopra H, Sahariah SA, et al. Eff ects of a food–
based
intervention on markers of micronutrient status among Indian
women of low socio-economic status. Br J Nutr 2015; 113: 813–
21.
75 Ahmed T, Choudhury N, Hossain MI, et al. Development and
acceptability testing of ready-to-use supplementary food made
from
locally available food ingredients in Bangladesh. BMC Pediatr
2014;
14: 164.
76 Shillcutt SD, Walker DG, Goodman CA, Mills AJ. Cost eff
ectiveness
in low- and middle-income countries: a review of the debates
surrounding decision rules. Pharmacoeconomics 2009; 27: 903–
17.
77 Mathew JL. Inequity in childhood immunization in India: A
systematic review. Indian Pediatr 2012; 49: 203–23.
78 Akinyemiju TF. Socio-economic and health access
determinants of
49. breast and cervical cancer screening in low-income countries:
analysis of the World Health Survey. PLoS one 2012; 7:
e48834.
79 Pilger D, Heukelbach J, Khakban A, Oliveira FA, Fengler G,
Feldmeier H. Household-wide ivermectin treatment for head lice
in
an impoverished community: randomized observer-blinded
controlled trial. Bull World Health Organ 2010; 88: 90–96.
80 Awasthi S, Peto R, Pande VK, Fletcher RH, Read S, Bundy
DA.
Eff ects of deworming on malnourished preschool children in
India: an open-labelled, cluster-randomized trial.
PLoS Negl Trop Dis 2008; 2: e223.
81 Sur D, Saha DR, Manna B, Rajendran K, Bhattacharya SK.
Periodic deworming with albendazole and its impact on growth
status and diarrhoeal incidence among children in an urban slum
of India. Trans R Soc Trop Med Hyg 2005; 99: 261–67.
82 Sarkar NR, Anwar KS, Biswas KB, Mannan MA. Eff ect of
deworming on nutritional status of ascaris infested slum
children
of Dhaka, Bangladesh. Indian Pediatr 2002; 39: 1021–26.
83 Awasthi S, Pande VK. Six-monthly de-worming in infants to
study
eff ects on growth. Indian J Pediatr 2001; 68: 823–27.
84 Taylor-Robinson DC, Maayan N, Soares-Weiser K, Donegan
S,
Garner P. Deworming drugs for soil-transmitted intestinal
worms
in children: eff ects on nutritional indicators, haemoglobin, and
school performance. Cochrane Database Syst Rev 2015; 7:
50. CD000371.
85 McPake B, Hanson K. Managing the public–private mix to
achieve
universal health coverage. Lancet 2016; 388: 622–30.
86 Samb B, Evans T, Dybul M, et al. An assessment of
interactions
between global health initiatives and country health systems.
Lancet 2009; 373: 2137–69.
87 Keare D, Parris S. Evaluation of shelter programs for the
urban
poor: principal fi ndings. Washington, DC: The World Bank,
1982.
88 Thieme T, Kovacs E. Services and slums: rethinking
infrastructures
and provisioning across the nexus. The Nexus Network Think
Piece
Series, Paper 004. Brighton: The Nexus Network, 2015.
89 Lobo J. The science and practice of urban planning in slums.
2016.
URL: https://ugecviewpoints.wordpress.com/2016/05/31/the-
science-and-practice-of-urban-planning-in-slums/ (accessed
June 29, 2016).
90 Buckley R. Social inclusion in Mumbai: economics matters
too.
Environ Urban 2011; 23: 277–84.
91 Murthy SL. Land security and the challenges of realizing the
human
right to water and sanitation in the slums of Mumbai, India.
Health Hum Rights 2012; 14: 61–73.
51. 92 Banerjee A, Dufl o E, Chattopadhyay R, Shapiro J. Targeting
the
hard-core poor: an impact assessment. New York: Public Aff
airs,
2011.
Series
570 www.thelancet.com Vol 389 February 4, 2017
93 Banerjee AV, Dufl o E. Mandated empowerment: handing
antipoverty policy back to the poor? Reducing the impact of
poverty
on health and human development: scientifi c approaches.
Ann N Y Acad Sci 2008; 1136: 333–41.
94 Brown C, Hofer T, Johal A, et al. An epistemology of patient
safety
research: a framework for study design and interpretation.
Part 2. Study design. Qual Saf Health Care 2008; 17: 163–69.
95 Chen YF, Hemming K, Stevens AJ, Lilford RJ. Secular
trends and
evaluation of complex interventions: the rising tide
phenomenon.
BMJ Qual Saf 2016; 25: 303–10.
96 Field E, Kremer M. Impact evaluation for slum upgrading
interventions. Washington DC: The World Bank, 2006.
97 Hemming K, Haines TP, Chilton PJ, Girling AJ, Lilford RJ.
The stepped wedge cluster randomised trial: rationale, design,
analysis, and reporting. BMJ 2015; 350: h391.
52. 98 Girling AJ, Hemming K. Statistical effi ciency and optimal
design
for stepped cluster studies under linear mixed eff ects models.
Stat Med 2016. 35: 2149–66.
99 Sweeney S, Vassall A, Foster N, et al. Methodological issues
to
consider when collecting data to estimate poverty impact in
economic evaluations in low-income and middle-income
countries.
Health Econ 2016; 25: 42–52.
100 Greco G, Lorgelly P, Yamabhai I. Outcomes in economic
evaluations of public health interventions in low- and
middle-income countries: health, capabilities and subjective
wellbeing. Health Econ 2016; 25: 83–94.
Improving the health and welfare of people who live in
slumsIntroductionFramework for reviewMeso-level policies
directed at slumsRestriction of migration or benign
neglectResettlement and reallocation programmesSecurity of
tenureGovernanceCommunity engagementSpecific (micro-level)
interventions in slumsPhysical and engineering approaches in
slum upgradingWater and sanitationHome
improvementsLighting, repaving, and garbage removalHealth
and public servicesRecommendations for policy and
researchIdentification and study of slums as spatial
entitiesChild healthSanitation and water qualityThe art of the
possible in slum improvementA call for multicentre studies with
contemporaneous controlsConsideration of several outcomes
and populationsSlum health as an academic
disciplineConclusionAcknowledgmentsReferences
Nursing in 3D: Diversity, Disparities, and Social Determinants
54. shape health
in powerful ways . We use “medical care” rather than “health
care” to refer to
clinical services, to avoid potential confusion between “health”
and “health
care .” The World Health Organization’s Commission on the
Social Determi-
nants of Health has defined SDH as “the conditions in which
people are born,
grow, live, work and age” and “the fundamental drivers of these
conditions .”
The term “social determinants” often evokes factors such as
health-related
features of neighborhoods (e .g ., walkability, recreational
areas, and accessibil-
ity of healthful foods), which can influence health-related
behaviors . Evidence
has accumulated, however, pointing to socioeconomic factors
such as income,
wealth, and education as the fundamental causes of a wide range
of health
outcomes . This article broadly reviews some of the knowledge
accumulated to
date that highlights the importance of social—and particularly
socioeconomic—
factors in shaping health, and plausible pathways and biological
mechanisms
that may explain their effects . We also discuss challenges to
advancing this
knowledge and how they might be overcome .
http://crossmark.crossref.org/dialog/?doi=10.1177%2F00333549
141291S206&domain=pdf&date_stamp=2014-01-01
55. Determinants
Public Health Reports / 2014 Supplement 2 / Volume 129
A large and compelling body of evidence has accu-
mulated, particularly during the last two decades, that
reveals a powerful role for social factors—apart from
medical care—in shaping health across a wide range
of health indicators, settings, and populations.1–16 This
evidence does not deny that medical care influences
health; rather, it indicates that medical care is not the
only influence on health and suggests that the effects
of medical care may be more limited than commonly
thought, particularly in determining who becomes sick
or injured in the first place.4,6,7,17,18 The relationships
between social factors and health, however, are not
simple, and there are active controversies regarding
the strength of the evidence supporting a causal role
of some social factors. Meanwhile, researchers increas-
inglyare calling into question the appropriateness of
traditional criteria for assessing the evidence.17,19–22
The limits of medical care are illustrated by the
work of the Scottish physician, Thomas McKeown,
who studied death records for England and Wales
from the mid-19th century through the early 1960s.
He found that mortality from multiple causes had
fallen precipitously and steadily decades before the
availability of modern medical-care modalities such
as antibiotics and intensive care units. McKeown
attributed the dramatic increases in life expectancy
since the 19th century primarily to improved living
conditions, including nutrition, sanitation, and clean
water.23 While advances in medical care also may have
contributed,23–26 most authors believe that nonmedical
56. factors, including conditions within the purview of tra-
ditional public health, were probably more important;24
public health nursing, including its role in advocacy,
may have played an important role in improved living
standards.27 Another example of the limits of medical
care is the widening of mortality disparities between
social classes in the United Kingdom in the decades
following the creation of the National Health Service in
1948, which made medical care universally accessible.28
Using more recent data, Martinson found that although
health overall was better in the United Kingdom than
in the United States, which lacks universal coverage,
disparities in health by income were similar in the two
countries.29 Large inequalities in health
according to
social class have been documented repeatedly across
different European countries, again despite more
universal access to medical care.30–32
Another often-cited example of the limits of medi-
cal care is the fact that, although spending on medical
care in the U.S. is far higher than in any other nation,
the U.S. has consistently ranked at or near the bottom
among affluent nations on key measures of health, such
as life expectancy and infant mortality; furthermore,
the country’s relative ranking has fallen over time.33,34
A recent report from the National Research Council
and Institute of Medicine has documented that the
U.S. health disadvantage in both morbidity and mor-
tality applies across most health indicators and all
age groups except those older than 75 years of age; it
applies to affluent as well as poor Americans, and to
non-Latino white people when examined separately.35
Other U.S. examples include the observation that,
while expansions of Medicaid maternity care around
57. 1990 resulted in increased receipt of prenatal care by
African American women,36,37 racial disparities in the
key birth outcomes of low birthweight and preterm
delivery were not reduced.38 Although important for
maternal health, traditional clinical prenatal care
generally has not been shown to improve outcomes
in newborns.39–44
THE IMPACTS OF SOCIOECONOMIC
AND OTHER SOCIAL FACTORS ON
MOST HEALTH OUTCOMES
A number of studies have attempted to assess the
impact of social factors on health. A review by McGin-
nis et al. estimated that medical care was responsible
for only 10%–15% of preventable mortality in the
U.S.;45 while Mackenbach’s studies suggest that this
percentage may be an underestimate, they affirm the
overwhelming importance of social factors.25,26 McGin-
nis and Foege concluded that half of all deaths in
the U.S. involve behavioral causes;18 other evidence
has shown that health-related behaviors are strongly
shaped by social factors, including income, education,
and employment.46,47 Jemal et al., studying 2001 U.S.
death data, concluded that “potentially avoidable fac-
tors associated with lower educational status account
for almost half of all deaths among working-age adults
in the U.S.”48 Galea and colleagues conducted a meta-
analysis, concluding that the number of U.S. deaths
in 2000 attributable to low education, racial segrega-
tion, and low social support was comparable with the
number of deaths attributable to myocardial infarction,
cerebrovascular disease, and lung cancer, respectively.49
The health impact of social factors also is supported
by the strong and widely observed associations between
58. a wide range of health indicators and measures of
individuals’ socioeconomic resources or social position,
typically income, educational attainment, or rank in
an occupational hierarchy. In U.S. as well as European
data, this association often follows a stepwise gradient
pattern, with health improving incrementally as social
position rises. This stepwise gradient pattern was first
noted in the United Kingdom.28,50 Although research
Public Health Reports / 2014 Supplement 2 / Volume 129
on the socioeconomic gradient has been more limited
in the U.S., the results of U.S. studies have mirrored
the European findings. Figures 1–5 illustrate a few
examples using U.S. data, with social position reflected
by income or by educational attainment. Using national
data, the National Center for Health Statistics’ “Health,
United States, 1998” documented socioeconomic gra-
dients in the majority of numerous health indicators
measured across different life stages.51 Braveman and
colleagues confirmed those findings using recent U.S.
data.52 Both Pamuk et al.51 and Braveman et al.52 found
that socioeconomic gradient patterns predominated
when examining non-Latino black and white groups
but were less consistent among Latino people. Minkler
and colleagues found dramatic socioeconomic gradi-
ents in functional limitations among people aged 65–74
years. This finding is particularly remarkable because
income gradients generally tend to flatten in old age.53
As illustrated in Figure 5, and in both Pamuk et al.51
and Braveman et al.,52 these socioeconomic gradients
in health have been observed not only in the U.S.
59. population overall, but within different racial/ethnic
groups, demonstrating that the socioeconomic differ-
ences are not explained by underlying racial/ethnic
differences. Indeed, most studies that have examined
racial/ethnic differences in health after adjusting for
socioeconomic factors have found that the racial/
ethnic differences disappeared or were substantially
reduced.54–56 This does not imply that the only differ-
ences in experiences between racial/ethnic groups
are socioeconomic; for example, racial discrimination
could harm the health of individuals of all socioeco-
nomic levels by acting as a pervasive stressor in social
interactions, even in the absence of anyone’s conscious
intent to discriminate.57,58 Furthermore, the black-white
disparity in birth outcomes is largest among highly
educated women.59 Living in a society with a strong
legacy of racial discrimination could damage health
through psychobiologic pathways, even without overtly
discriminatory incidents.60–62
How do widespread and persistent socioeconomic
gradients in health add to evidence that social fac-
tors are important influences on health? Strong links
between poverty and health have been observed for
centuries.63–65 Observing a graded relationship (as
opposed to a simple threshold, for instance at the pov-
erty line) of socioeconomic factors with many different
health indicators suggests a possible dose-response rela-
tionship, adding to the likelihood that socioeconomic
factors—or factors closely associated with them—play
a causal role. Although the effects of abject poverty on
health are rarely disputed, not everyone concurs about
the effects of income and education on health across
the socioeconomic spectrum. Some have argued that
income-health or education-health relationships reflect
60. reverse causation (i.e., sickness leading to income loss
and/or lower educational achievement).66 Although ill
health often results in lost income, and a child’s poor
Figure 1. Life expectancy in the U.S. at age 25, by education
and gender, 2006a
aSource: Department of Health and Human
Services (US), National Center for Health
Statistics. Health, United States 2011: with
special feature
on socioeconomic status and health. Life expectancy
at age 25, by sex and education level [cited
2012 Nov 29]. Available from: URL: http://
www .cdc .gov/nchs/data/hus/2011/fig32 .pdf . Reported in:
Braveman P, Egerter S . Overcoming obstacles to health in 2013
and beyond: report for
the Robert Wood Johnson Foundation Commission to Build a
Healthier America . Princeton (NJ): Robert Wood Johnson
Foundation; 2013 .
L
if
e
e
x
p
e
ct
a
n
cy
61. a
t
a
g
e
2
5
(
in
y
e
a
rs
)
Diversity, Disparities, and Social
Determinants
Public Health Reports / 2014 Supplement 2 / Volume 129
health could limit educational achievement, evidence
from longitudinal and cross-sectional studies indicate
that these do not account for the strong, pervasive
relationships observed.67 Links between education and
health, furthermore, cannot be explained by reverse
causation because once attained, educational attain-
ment is never reduced.
62. The aforementioned evidence reflects associations
that by themselves do not establish causation. However,
the observational examples cited as illustrations are
backed up by extensive literature employing a range
of techniques (e.g., multiple regression,
instrumental
variables, matched case-control designs, and propensity
score matching) to reduce bias and confounding due
to unmeasured variables.3,4,7,17,19 This knowledge base
is also enriched by natural experiments,3,36,68,69 quasi-
experiments,70 and some, albeit limited, randomized
controlled experiments.71–74 The overwhelming weight
of evidence demonstrates the powerful effects of socio-
economic and related social factors on health, even
when definitive knowledge of specific mechanisms
and effective interventions is limited. Accumulated
knowledge also reveals, however, that the effects of any
given social (including socioeconomic) factor are often
contingent on a host of other factors.17,75 The third
section of this article discusses challenges in studying
the effects of socioeconomic factors that are relatively
“upstream” (i.e., closer to underlying or fundamental
causes)76 from their health effects located “down-
stream” (i.e., near where health effects are observed).
MULTIPLE MECHANISMS EXPLAIN
IMPACTS OF SOCIOECONOMIC AND
OTHER SOCIAL FACTORS ON HEALTH
Despite countless unanswered questions, knowledge of
the pathways and biological mechanisms connecting
social factors with health has increased exponentially
during the past 25 years. Mounting evidence supports
63. causal relationships between many social—including
socioeconomic—factors and many health outcomes,
not only through direct relationships but also through
more complex pathways often involving biopsychoso-
cial processes.77
Some aspects of socioeconomic factors are con-
nected to health via responses to relatively direct and
rapid-acting exposures. For instance, lead ingestion
in substandard housing contributes to low cognitive
function and stunted physical development in exposed
children;78,79 pollution and allergens, also more com-
mon in disadvantaged neighborhoods, can exacerbate
asthma.80,81 Socioeconomic and other social factors also
Figure 2. Infant mortality rate in the U.S., by mother’s
education, 2009a
aSource: Mathews TJ, MacDorman MF . Infant mortality
statistics from the 2009 period linked birth/infant death dataset .
Natl Vital Stat Rep
2013;61:1-28. Also available from: URL:
http://www.cdc.gov/nchs/data/nvsr/nvsr61/nvsr61_08.pdf
[cited 2013 Feb 14]. Reported in: Braveman
P, Egerter S . Overcoming obstacles to health in 2013 and
beyond: report for the Robert Wood Johnson Foundation
Commission to Build a
Healthier America . Princeton (NJ): Robert Wood Johnson
Foundation; 2013 .
In
fa
n
t
65. Public Health Reports / 2014 Supplement 2 / Volume 129
may contribute to worse health through pathways that
play out over relatively short time frames (e.g., months
to a few years) but are somewhat more indirect. Fac-
tors affecting the social acceptability of risky health
behaviors are a case in point. For instance, exposure
to violence can increase the likelihood that young
people will perpetrate gun violence;82 and the avail-
ability of alcohol in disadvantaged neighborhoods can
influence its use among young people, affecting rates
of alcohol-related traumatic injury.83 Socioeconomic
factors can influence sleep, which can be affected by
work, home, and neighborhood environments, and
which can have short-term health effects.84,85 Working
conditions can shape health-related behaviors, which,
in turn, may impact others; for example, workers with-
out sick leave are more likely to go to work when ill,
increasing the likelihood of disease spread to cowork-
ers or customers.86
In addition to these relatively rapid health impacts,
the effects of socioeconomic and other social factors
on health-related behaviors can influence disease
outcomes that only manifest much later in life.
Neighborhood socioeconomic disadvantage and
higher concentration of convenience stores have been
linked to tobacco use, even after adjusting for several
individual-level characteristics, such as educational
attainment and household income.87 Lower availability
of fresh produce, combined with concentrated fast-food
66. outlets and few recreational opportunities, can lead
to poorer nutrition and less physical activity.88,89 The
health consequences of the chronic diseases related
to
these conditions generally will not appear for decades.
The strong and pervasive relationships between
socioeconomic factors and physical health outcomes
can reflect even more complex and long causal path-
ways, which may or may not involve health behaviors
as key mediators or moderators. Evans and Schamberg
showed that the association between duration of child-
hood poverty and adult cognitive function appears
to be explained not only by poverty-related material
deficits, but also partly by chronic childhood stress.90
Cutler et al. described widening mortality disparities
by educational achievement that are not explained by
behavioral risk factors such as tobacco use or obesity.91
Children growing up in socioeconomically disadvan-
taged neighborhoods face greater direct physical chal-
lenges to health status and health-promoting behaviors;
they also often experience emotional and psychological
stressors, such as family conflict and instability arising
from chronically inadequate resources. Adjusting for
depression, anxiety, and other negative emotional
states, however, has not completely explained the
effects of social factors on health.92
Several recent reviews93–98 have described the bio-
logical “wear-and-tear” resulting from chronic expo-
sure to social and environmental stressors, commonly
Figure 3. U.S. children aged <17 years with less than very good
health, by family income, 2011–2012a
aSource: National Survey of Children’s Health.
67. NSCH 2011/2012. Data query from the Child
and Adolescent Health Measurement Initiative,
Data Resource Center for Child and Adolescent
Health [cited 2013 May 10]. Available from:
URL: http://www.childhealthdata.org/browse/survey
/results?q=2456&r=1&g=458. Reported in: Braveman P,
Egerter S. Overcoming obstacles to health in
2013 and beyond: report for the Robert
Wood Johnson Foundation Commission to Build a Healthier
America . Princeton (NJ): Robert Wood Johnson Foundation;
2013 .
P
e
rc
e
n
t
o
f
ch
ild
re
n
<
1
7
y
e
a
69. a
lt
h
Determinants
Public Health Reports / 2014 Supplement 2 / Volume 129
referred to as allostatic load.99 Allostatic load is a
multicomponent construct that reflects physiologic
changes across different biological regulatory systems
in response to chronic social and environmental stress.
Examples include observations that stress can induce
pro-inflammatory responses, including production of
IL-6100 and C-reactive protein,101 and that lower income
and educational achievement contribute to higher
blood pressure and unfavorable cholesterol profiles.102
Physiological regulatory systems thought to be affected
by social and environmental stressors have included
the hypothalamic-pituitary-adrenal axis; sympathetic
(autonomic) nervous system; and immune/inflamma-
tory, cardiovascular, and metabolic systems.93,95 These
systems overlap peripherally and in the brain.
Another area of rapidly evolving knowledge involves
the role of socioeconomic and other social factors in
epigenetic processes that regulate whether genes are
expressed or suppressed.103 Evidence from primate
studies suggests that social status can affect the regula-
tion of genes controlling physiologic functions (e.g.,
immune functioning).104 In addition, educational
attainment,105,106 occupational class (e.g., manual vs.
70. non-manual work),107 work schedules,108 perceived
stress,109,110 and intimate partner violence111 have all
been linked with changes in telomere length.112 Telo-
meres are DNA-protein complexes capping the ends
of chromosomes, protecting them against damage.
Telomere shortening is considered a marker of cellular
aging113 that is controlled by both genetic and epigen-
etic factors. Multiple biological mechanisms appear
to be involved in causal pathways from social factors
to health outcomes. For example, an allostatic load
index combining information on multiple biomarkers
of health risk appears to explain more of the impact
of education on mortality than any single biological
indicator alone.114 Associations between psychosocial
processes and physiology are further complicated by
the effects of timing, such as when and for how long a
stressor is experienced in an individual’s lifespan.115,116
Early-life socioeconomic disadvantage has been repeat-
edly associated with vulnerability to a range of adoles-
cent and adult diseases,117 independent of adolescent
or adult socioeconomic status/position.118–121 Overall,
there appear to be both cumulative effects of socioeco-
nomic and related social stressors across the lifespan,
manifesting in chronic disease in later adulthood,
and heightened effects of experiences occurring at
particularly sensitive periods in life (e.g., before age 5).
The physiologic effects of chronic stress is an area of
active biological, psychological, and social research that
seeks to explain the impact of many social factors on
health outcomes.
Despite considerable evidence indicating important
Figure 4. Percent of U.S. adults aged >25 years with activity-
limiting chronic disease,
71. by family income, 1988–1998a
aSource: Analyses by Braveman, Egerter, Cubbin, Pamuk, and
Johnson of data from the National Longitudinal Mortality
Study, 1988–1998, first
reported in: Braveman P, Egerter S . Overcoming obstacles to
health: report from the Robert Wood Johnson Foundation to the
Commission to
Build a Healthier America . Princeton (NJ): Robert Wood
Johnson Foundation; 2008 .
P
e
rc
e
n
t
o
f
a
d
u
lt
s
>
2
5
y
e
73. ic
d
is
e
a
se
Public Health Reports / 2014 Supplement 2 / Volume 129
effects of social factors on health, however, not every
individual exposed to socioeconomic or other adversity
develops disease. Protective social factors, such as social
support, self-esteem, and self-efficacy, may mitigate
the deleterious effects of adverse social conditions.92,95
Income and education have not predicted health as
consistently among Latino immigrants in the U.S. as
among other groups; hypothesized explanations have
included protective factors such as social support or
attitudes and norms that confer resilience.122,123 Simi-
larly, low income may have less impact on the health of
individuals in settings in which basic needs—including
food, housing, education, and/or medical care—are
met by the state or family.124 This may be due partly
to access to needed goods and services through routes
other than income, and also to an alleviation of insecu-
rity about meeting basic needs. Income may have less
health impact where there is less social stigma associ-
ated with having limited economic means. Genetics
also may play a role in an individual’s vulnerability
or resilience to socioeconomic adversity: different
74. individuals’ biological responses to the same socio-
environmental trigger can vary markedly according to
specific genetic polymorphisms.125 At the same time, as
noted, research has demonstrated that socioeconomic
and related social factors can alter whether a deleteri-
ous (or protective) gene is expressed or suppressed.
The graded relationships repeatedly observed (and
illustrated in Figures 1–5) between socioeconomic fac-
tors and diverse health outcomes may reflect gradients
in resources and exposures associated with socioeco-
nomic factors. They also may reflect the impact of
subjective social status (i.e., where one perceives oneself
as fitting relative to others in a social hierarchy deter-
mined by wealth, influence, and prestige).126 A growing
body of research in multiple disciplines—including
psychology, neurology, immunology, education, child
development, demography, economics, sociology,
and epidemiology—examines the interplay of socio-
economic factors, psychological and other mediating
factors, and biology. Evidence has clearly demonstrated
that relationships between socioeconomic factors and
health are complex, dynamic, and interactive; that they
may involve multiple mechanisms including epigenetic
processes that alter gene expression; and that, at times,
they may only manifest decades after exposure.
CHALLENGES OF STUDYING HOW
SOCIOECONOMIC AND OTHER UPSTREAM
SOCIAL FACTORS AFFECT HEALTH
While great advances in documenting and understand-
ing the social, including socioeconomic, determinants
of health have been made, unanswered questions
about
75. the mechanisms underlying their effects on health are
at least as plentiful as the answers we have to date. All
Figure 5. Socioeconomic gradients in poor/fair health among
adults aged 25–74 years within
racial/ethnic groups in the U.S., 2008–2010a
aSource: Analyses by Cubbin of Behavioral Risk Factor
Surveillance System survey data, 2008–2010, reported in:
Braveman P, Egerter S .
Overcoming obstacles to health in 2013 and beyond: report for
the Robert Wood Johnson Foundation Commission to Build a
Healthier
America . Princeton (NJ): Robert Wood Johnson Foundation;
2013 .
P
e
rc
e
n
t
o
f
a
d
u
lt
s
a
g
77. Determinants
Public Health Reports / 2014 Supplement 2 / Volume 129
rigorous research is challenging, but research on the
upstream social determinants of health (SDH) faces
particular challenges, based in part on the complexity
of the causal pathways and the long time periods during
which they often play out.17,127–131 Some of these barriers
are illustrated by the following example.
Figure 6 presents very simply three general pathways
through which education can influence many health
outcomes, reflecting links that have been described
in the literature. While there is not necessarily a con-
sensus about each step depicted here, all are plausible
in light of current knowledge, including biological
knowledge.132 The first pathway is widely accepted:
education increases knowledge and skills and, thus,
can facilitate healthier behaviors. The second path-
way also is biologically plausible. However, while its
left-sided branches (i.e., education leading to better,
higher-paid work) are not disputed, subsequent
links
from income to health through various pathways, such
as work-related benefits, neighborhood opportunities,
and stress, are not typically considered as education
effects. The third pathway depicts health effects of
education through psychobiological processes such
as control beliefs, subjective social status, and social
networks, again based on existing literature.123 Figure 6
illustrates two of the most daunting challenges facing
research on the socioeconomic and other upstream
determinants of health:
78. 1. Complex, multifactorial causal pathways do not
lend themselves to testing with randomized
experiments. This diagram is greatly oversimpli-
fied: the pathways appear linear, and the dia-
gram does not include the multitude of arrows
representing how the factors depicted may inter-
act with each other and with other variables not
depicted, such as genetic and epigenetic factors.
Despite the oversimplification, it illustrates how
Figure 6. Pathways through which education can affect healtha
aSource: Egerter S, Braveman P, Sadegh-Nobari T, Grossman-
Kahn R, Dekker M . Education matters for health . Exploring
the social determinants
of health: issue brief no . 6 . Princeton (NJ): Robert Wood
Johnson Foundation; 2011 .
How could education affect health?
Public Health Reports / 2014 Supplement 2 / Volume 129
upstream socioeconomic determinants such as
income, wealth, and education could exert their
effects over complicated multifactorial path-
ways.133 At each juncture, there are opportuni-
ties for confounding and interactions. A glance
at this diagram should make it clear that this
intricate series of causal relationships does not
lend itself to testing with randomized controlled
trials. Nevertheless, it may be possible to study
79. small pieces of the causal web with randomized
experiments, making incremental contributions
to understanding the overall pathways.17 Innova-
tive approaches to modeling complex, dynamic
systems are being developed to address these
challenges; however, it is uncertain whether
these systems will live up to expectations.134
2. There are long time lags for health effects to
manifest. The links between social factors and
health often play out over decades or genera-
tions; for example, chronic disease often takes
multiple decades to develop. Although we may
be able to use intermediate biomarkers (such as
C-reactive protein or IL-6) or certain behaviors
as proxies for health outcomes, it could be two
decades or more after the relevant exposures
(e.g., childhood adversity) before even these
intermediate markers manifest. Few studies
are able to follow participants for more than a
few years. The long time lag between indepen-
dent and dependent variables represents both
a scientific and a political challenge. Funders
and politicians want results within timeframes
for which they can take credit. The Office of
Management and Budget generally requires a
five-year-or-less time window for assessing policy
impact.
Another barrier to understanding the effects of
social factors on health is the difficulty of obtaining
information across multiple sectors (e.g., as education,
planning, housing, labor, and health) and even across
multiple programs within a given sector. Access to
cross-sectoral information could improve our under-
standing54 and ability to intervene effectively. However,
80. cross-sectoral collaborations face multiple barriers,
including differing priorities, funding streams, and
timelines across agencies; overcoming these barriers
will require a major shift in financial and
political incen-
tives.135 Some institutions, nevertheless, have begun to
encourage these collaborations. For example, the U.S.
Department of Housing and Urban Development has
developed a health council to incorporate health con-
siderations into federal housing policy.136 The Robert
Wood Johnson Foundation (RWJF) Commission to
Build a Healthier America has issued recommenda-
tions for several nonmedical care initiatives to improve
health overall while reducing health disparities, includ-
ing a strong emphasis on high-quality earlychild-
care
programs.137 The Federal Reserve Bank has recently
collaborated with RWJF to convene a series of national
and regional forums to discuss intersections between
community development and health improvement
CONCLUSIONS
Despite challenges, controversies, and unanswered
questions, the tremendous advances in knowledge
that
have occurred in the past 25 years leave little room for
doubt that social factors are powerful determinants of
health. The consistency and reproducibility of strong
associations between social (including socioeconomic)
factors and a multitude of health outcomes in diverse
settings and populations have been well documented,
and the biological plausibility of the influence of social
factors on health has been established. It is not sur-
prising that exceptional examples of health indicators,
81. settings, and subgroups in which health does not nec-
essarily improve with greater social advantage can be
found. There may be thresholds above which a higher
degree of a given social factor (e.g., income) no longer
yields better health. Exceptions would also be expected
as the effects of any given factor are contingent upon
the presence of myriad other factors—social, economic,
psychological, environmental, genetic, and epigenetic.
Considering the long, complex causal pathways leading
from social factors—particularly upstream ones such
as income and education—to health, with opportuni-
ties for countless interactions at each step, it is indeed
remarkable that there are so few exceptions to the
general rule.
The relative importance of social vs. genetic factors
is often debated. The emerging awareness of gene-
environment interactions, however, has drastically
altered nature-vs.-nurture debates. Social and genetic
causes of disease can no longer be seen as mutually
exclusive. We now know that adverse genetic endow-
ment is not necessarily unalterable, that a “bad” (or
“good”) gene may be expressed only in the presence
of triggers in the social or physical environment, and
that these environments potentially can be modified
by social policies.
Despite gaps in current knowledge, the case for
needing to address upstream socioeconomic factors
is strong, and enough is known to inform interven-
tions, which must be rigorously evaluated.17 Given
that SDH—including socioeconomic conditions such
as income, wealth, and education—are by definition