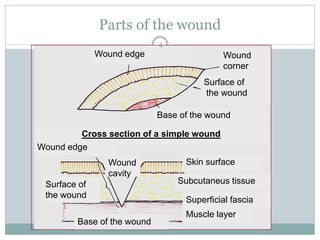
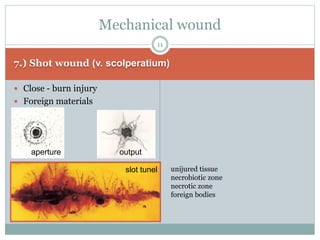
This document provides information on wound classification and management. It begins with defining a wound and its various parts. It then discusses assessing injured patients using the ABCDE mnemonic. The document thoroughly classifies wounds based on their origin, including mechanical, chemical, radiation, and thermal wounds. It also covers wound contamination levels and depths. Principles of wound healing and factors affecting it are explained. Various wound management techniques and complications are outlined. The document concludes with a section on bleeding and hemostasis methods.