Download to read offline
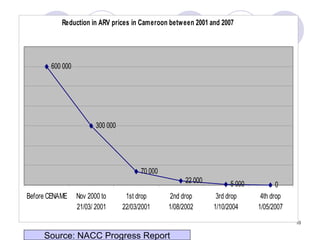
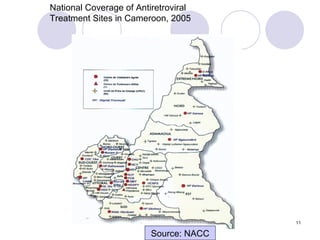
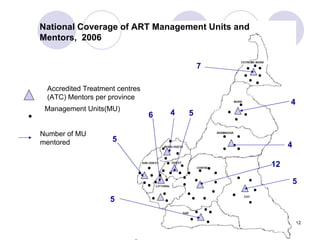
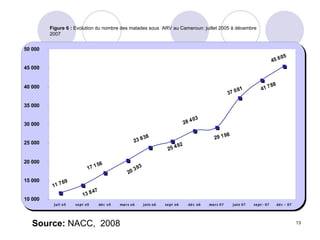
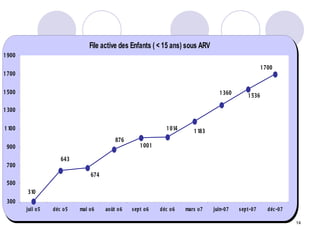
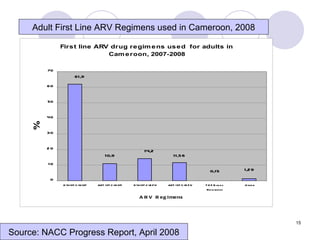
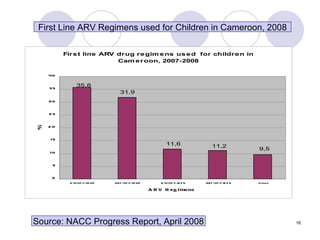


The document summarizes the experience of scaling up HIV treatment in Cameroon through operational research. Cameroon implemented a public health approach to decentralize HIV treatment from central and regional hospitals to district hospitals between 2001-2005. This was supported by standardized treatment guidelines, subsidies for laboratory tests, and a mentorship strategy. Operational research evaluated the impact and found early outcomes were better at district levels, including improved access, quality of care, adherence, and patient perceptions of decentralization. However, challenges remain around sustained drug supply, prevention of unsafe sex, and health worker satisfaction.























































































