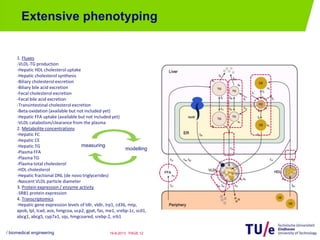
![Preclinical study of pharmaceutical
intervention
• Longitudinal data: control, treated for 1, 2, 4, 7, 14, and 21 days
/ biomedical engineering PAGE 1319-8-2013
0 10 20
0
100
200
Hepatic TG
Time [days]
[umol/g]
0 10 20
0
1
2
3
Hepatic CE
Time [days]
[umol/g]
0 10 20
0
2
4
6
Hepatic FC
Time [days]
[umol/g]
0 10 20
0
50
100
Hepatic TG
Time [days]
[umol]
0 10 20
0
0.5
1
1.5
Hepatic CE
Time [days]
[umol]
0 10 20
0
2
4
Hepatic FC
Time [days]
[umol]
0 10 20
0
1000
2000
3000
Plasma CE
Time [days]
[umol/L]
0 10 20
0
1000
2000
3000
HDL-CE
Time [days]
[umol/L]
0 10 20
0
500
1000
1500
Plasma TG
Time [days]
[umol/L]
0 10 20
6
8
10
12
VLDL clearance
Time [days]
[-]
0 10 20
100
200
300
400
ratio TG/CE
Time [days]
[-]
0 10 20
0
5
10
15
VLDL diameter
Time [days]
[nm]
0 10 20
0
1
2
3
VLDL-TG production
Time [days]
[umol/h]
0 10 20
1
2
3
Hepatic mass
Time [days]
[gram]
0 10 20
0
0.2
0.4
DNL
Time [days]
[-]
Grefhorst et al. Atherosclerosis, 2012, 222: 382– 389](https://image.slidesharecdn.com/vanriel-final-130819064525-phpapp01/85/Systems-Medicine-and-Metabolic-Diseases-13-320.jpg)
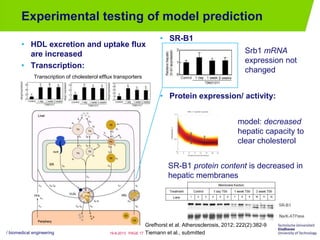
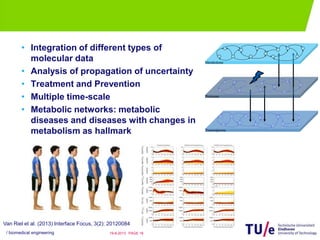
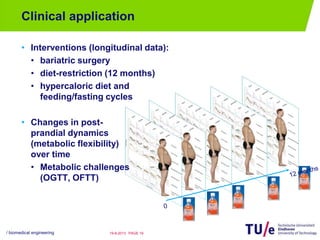


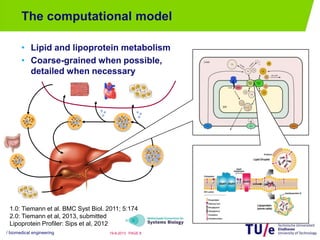
Natal van Riel from Eindhoven University of Technology presented on systems biology approaches for understanding metabolic diseases. She discussed (1) using systems biology models and data integration to understand the complex networks underlying metabolic syndrome and related diseases, (2) applying these approaches to analyze the effects of therapies and interventions over time, and (3) opportunities for clinical application including analyzing changes from bariatric surgery, diet, and metabolic challenges.




















































































