Downloaded 47 times




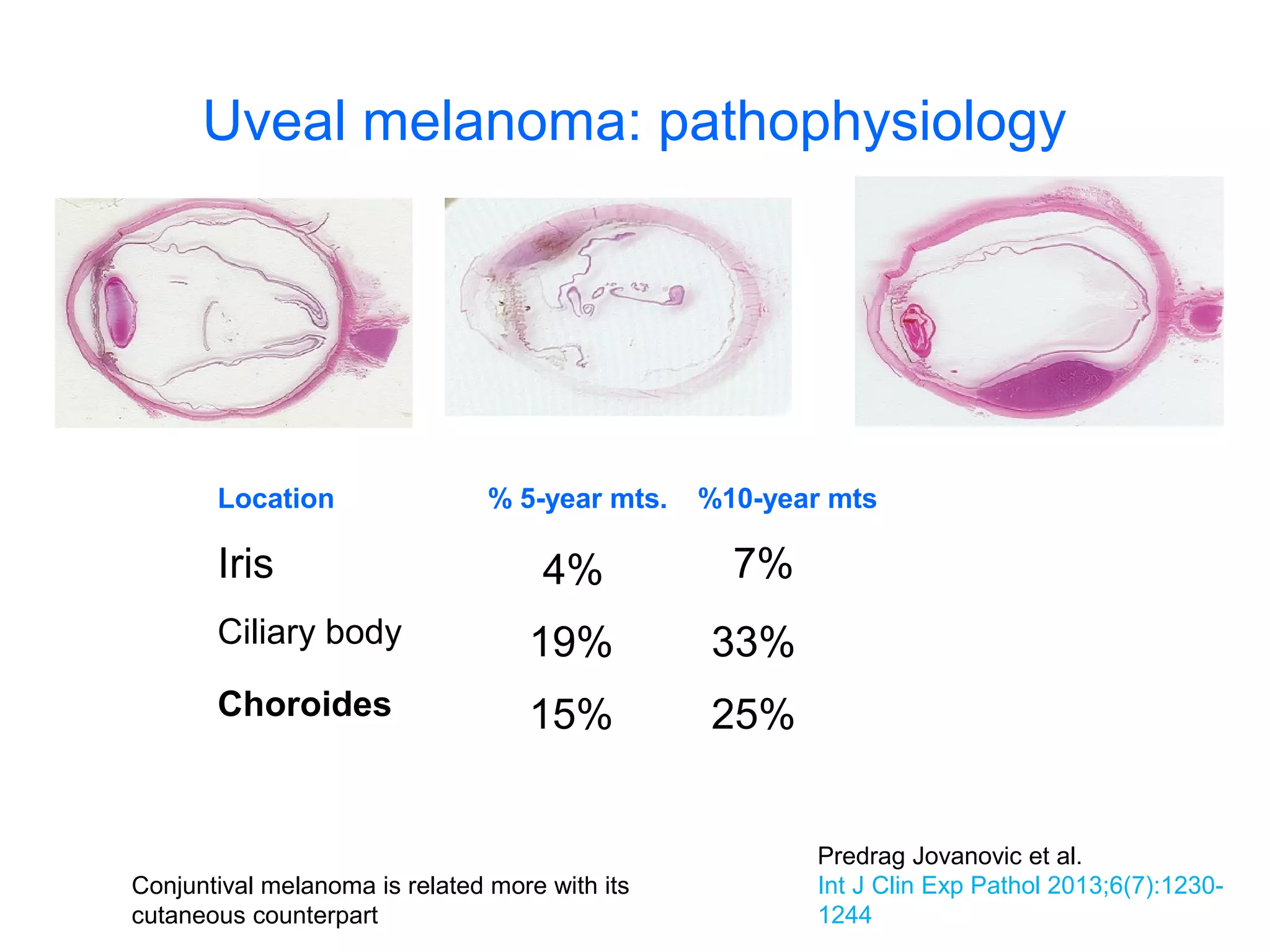






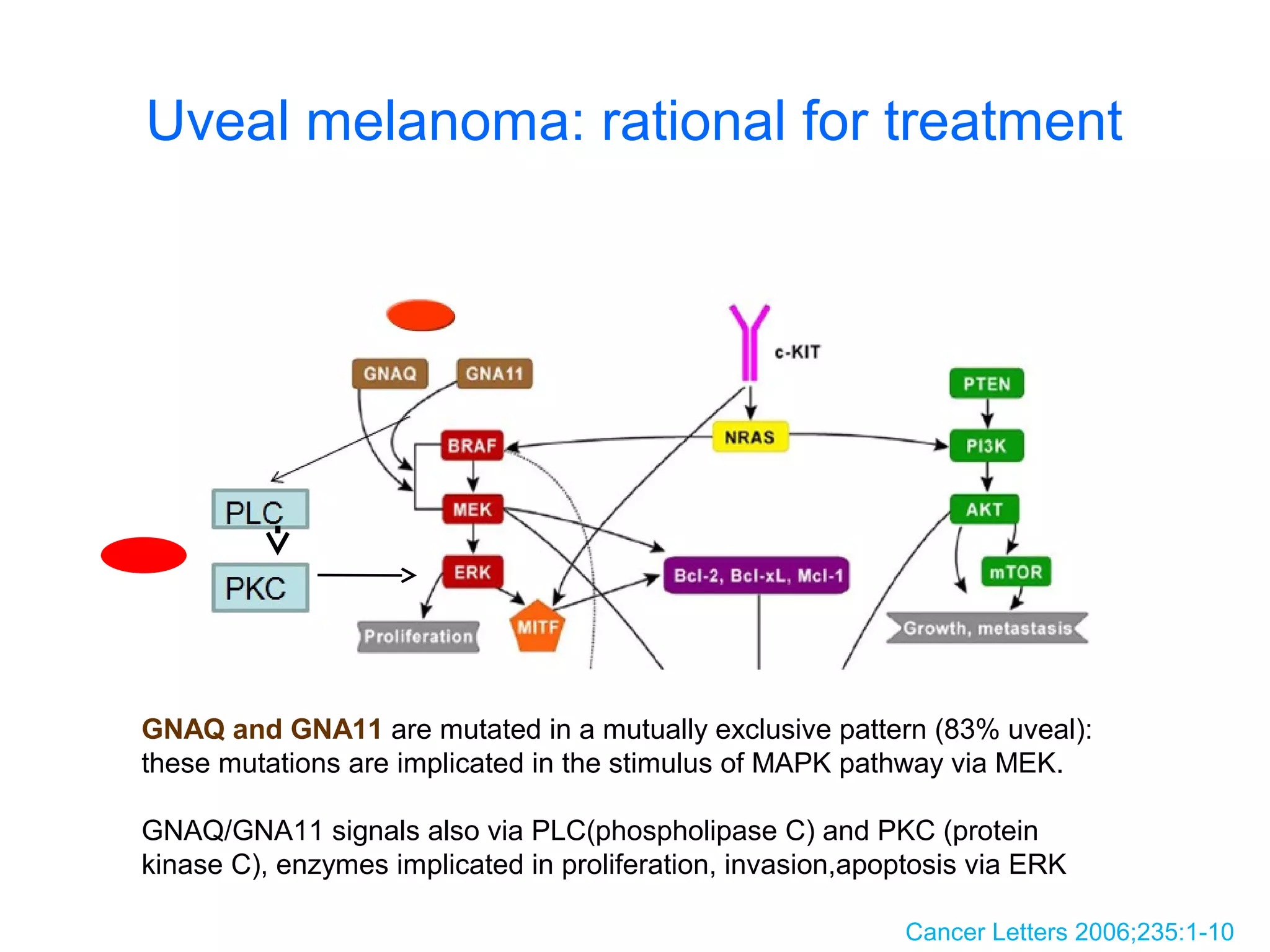



Melanoma can metastasize to various atypical locations beyond skin and subcutaneous tissues, with uveal melanoma being the most common primary eye malignancy. Key mutations in gnaq and gna11 are involved in 80% of uveal melanoma cases, influencing treatment options such as ipilimumab and targeted therapies like mek and pak inhibitors. Clinical outcomes show that ipilimumab provides over 30% one-year survival in metastatic cases, highlighting the need for further exploration of these mutations in therapeutic strategies.


















































































