Downloaded 13 times


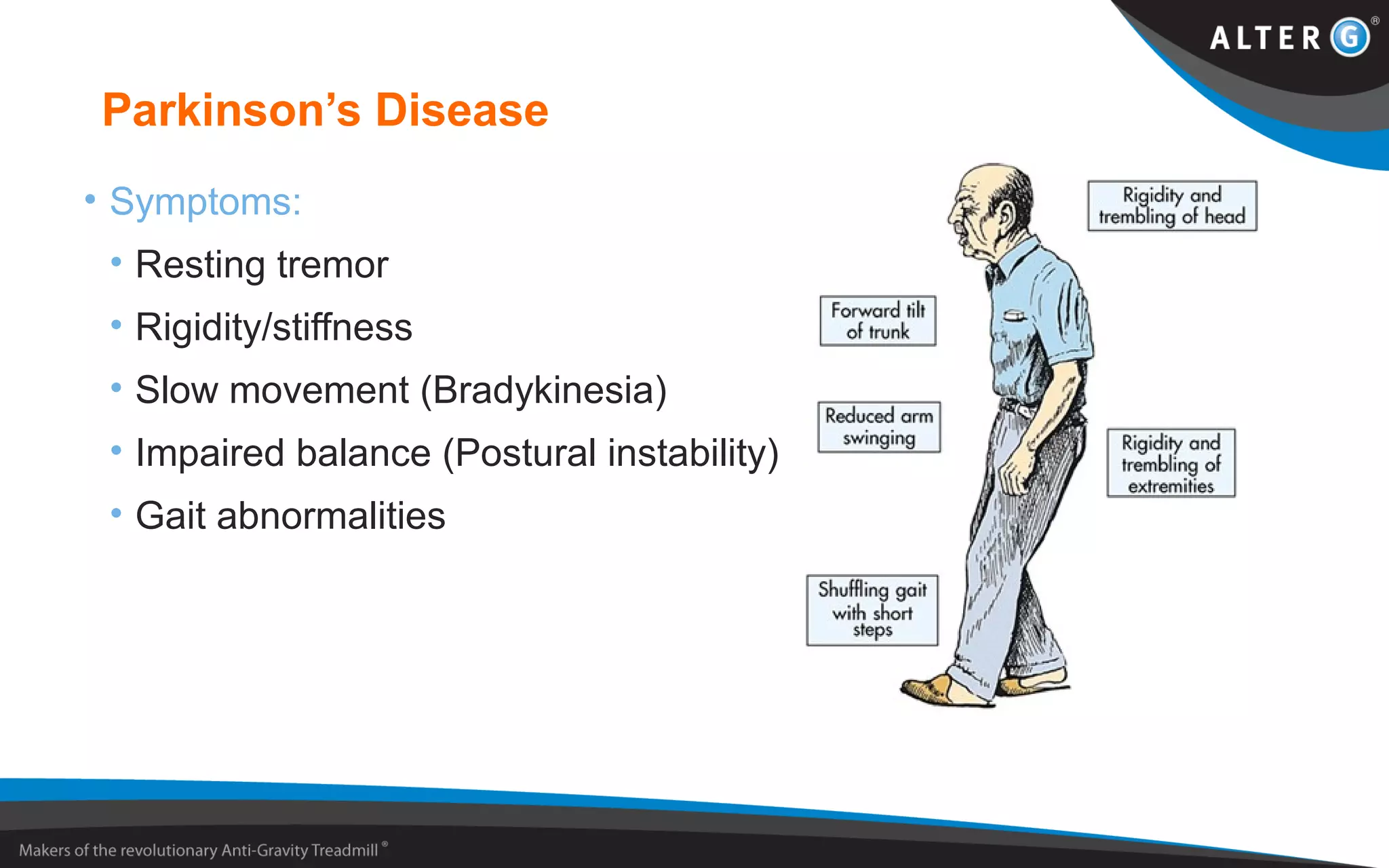
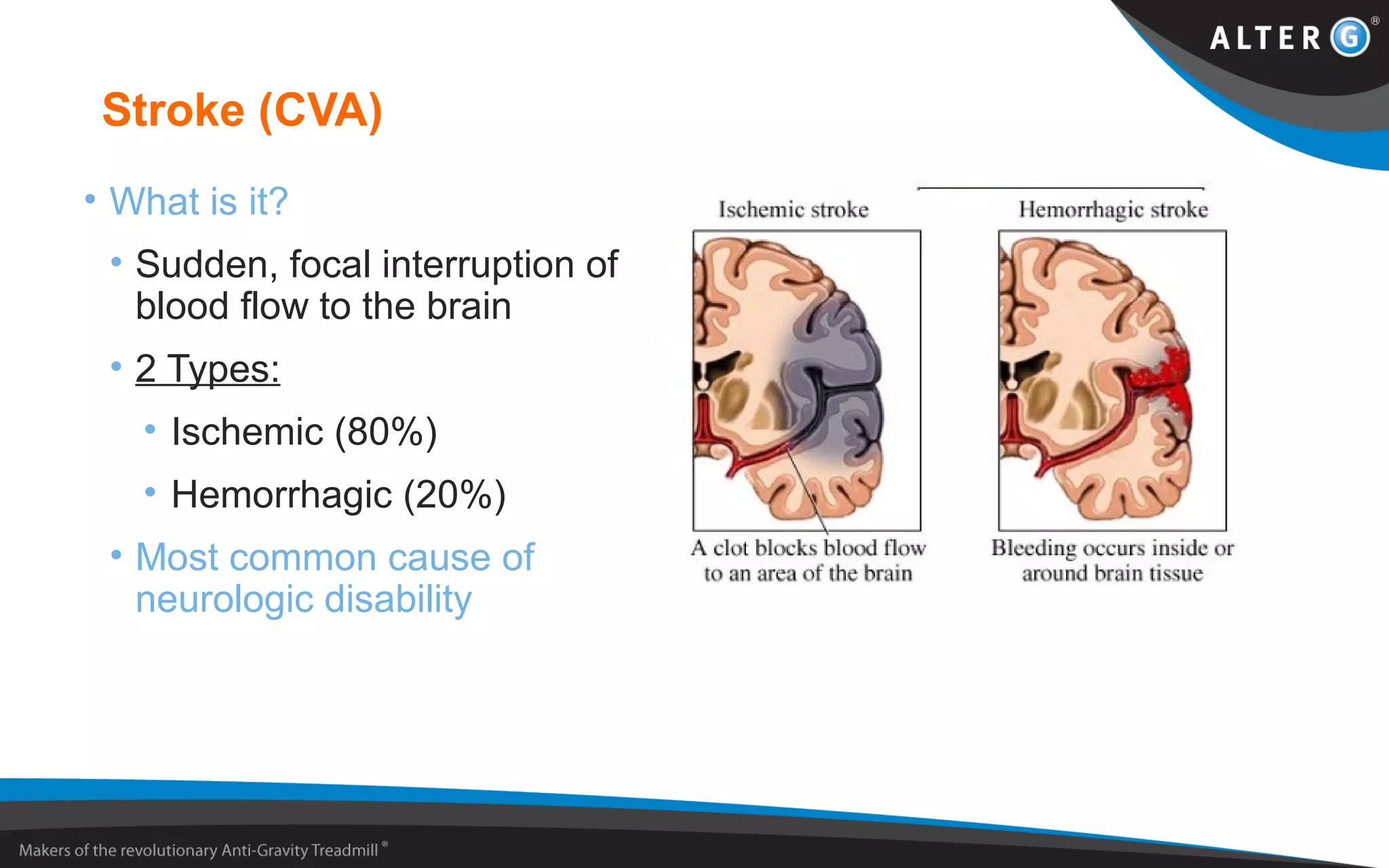
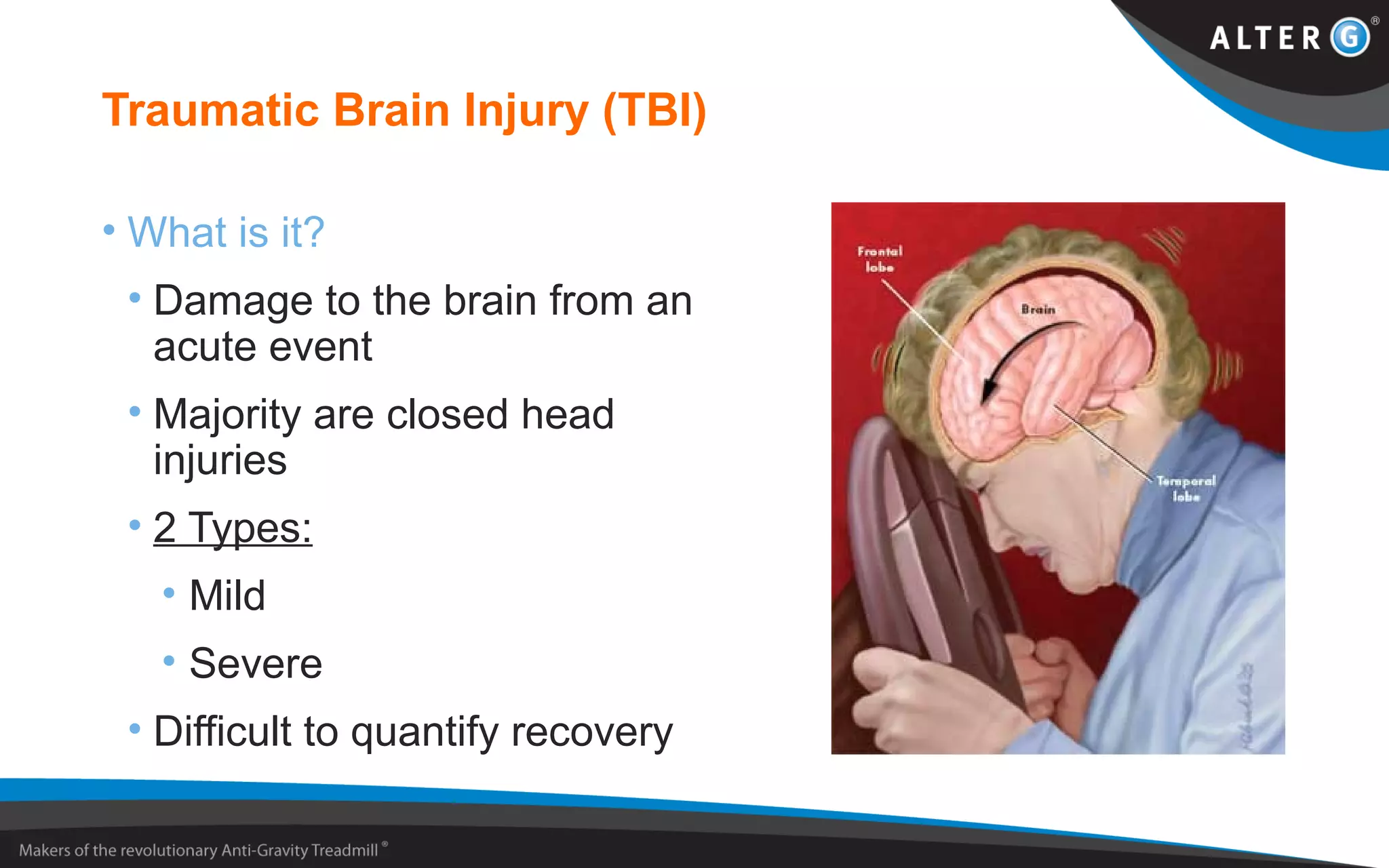
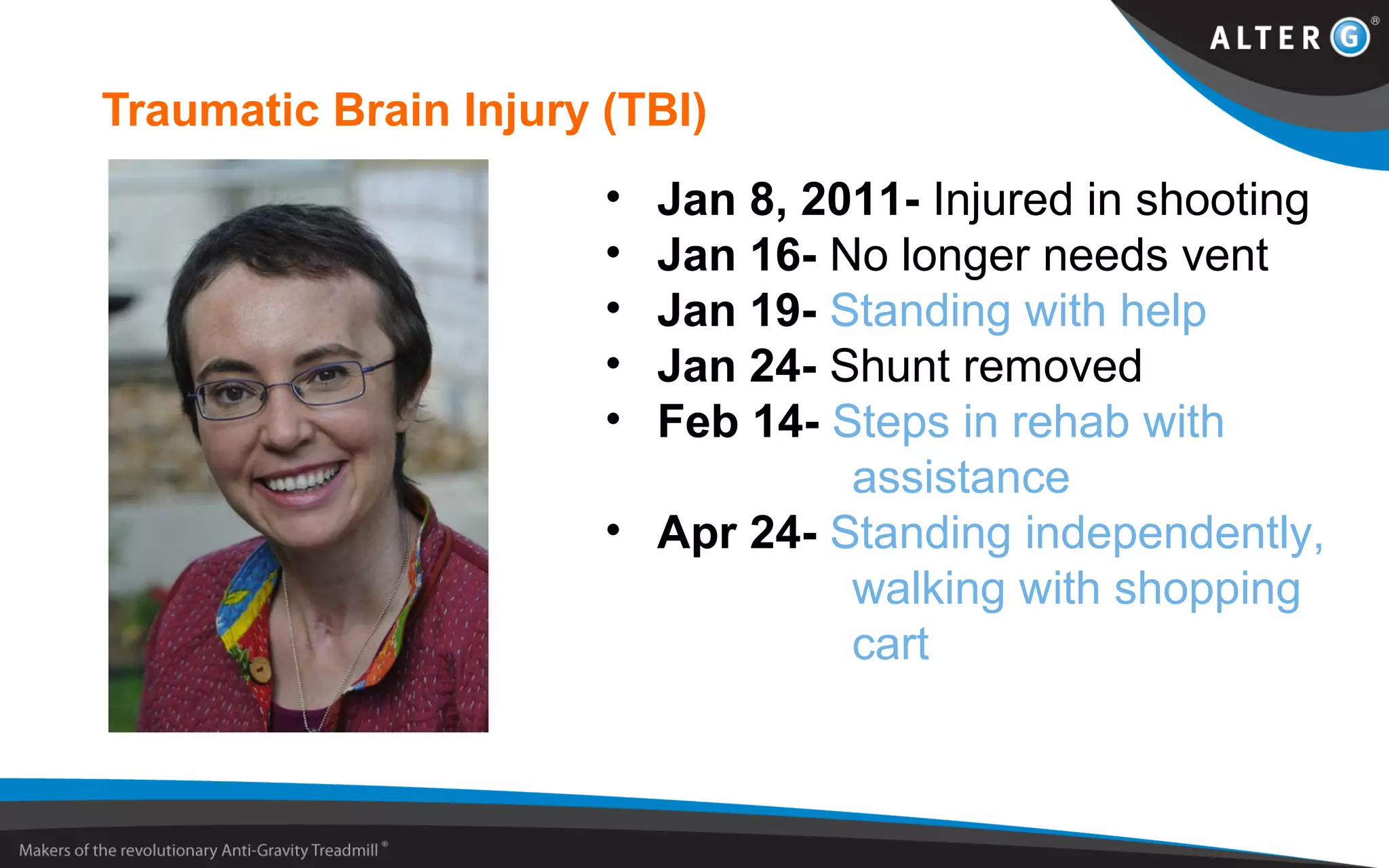
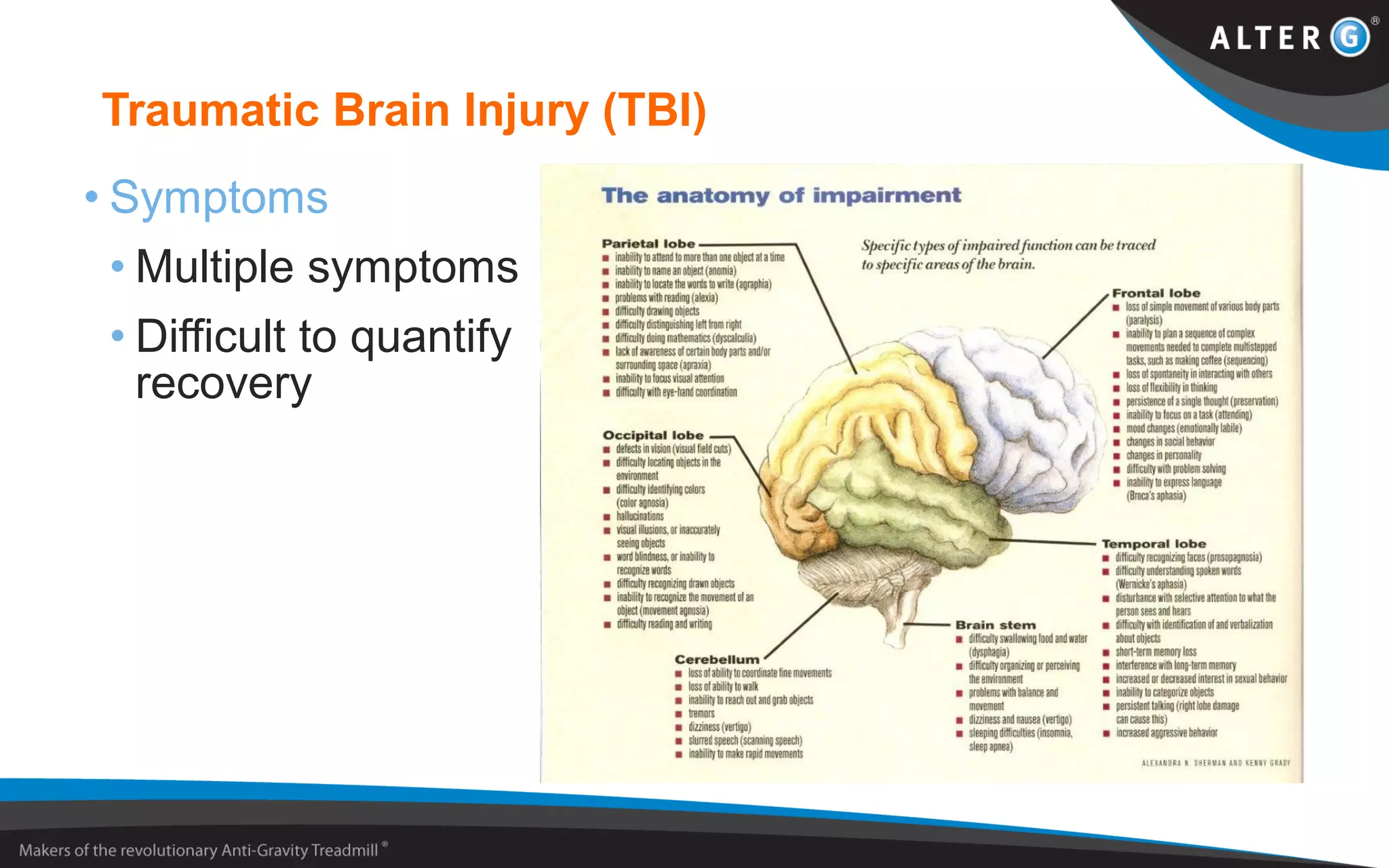

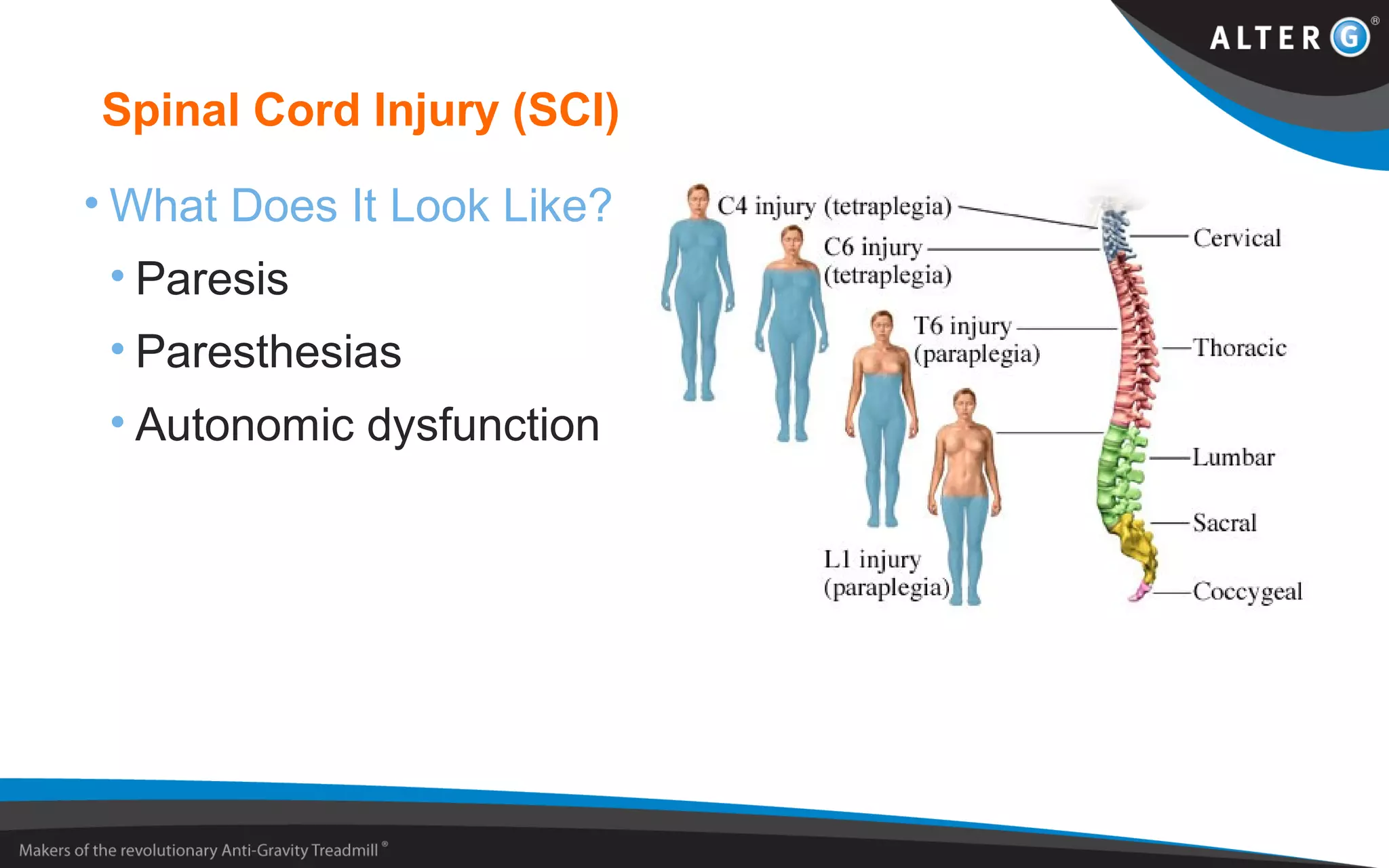
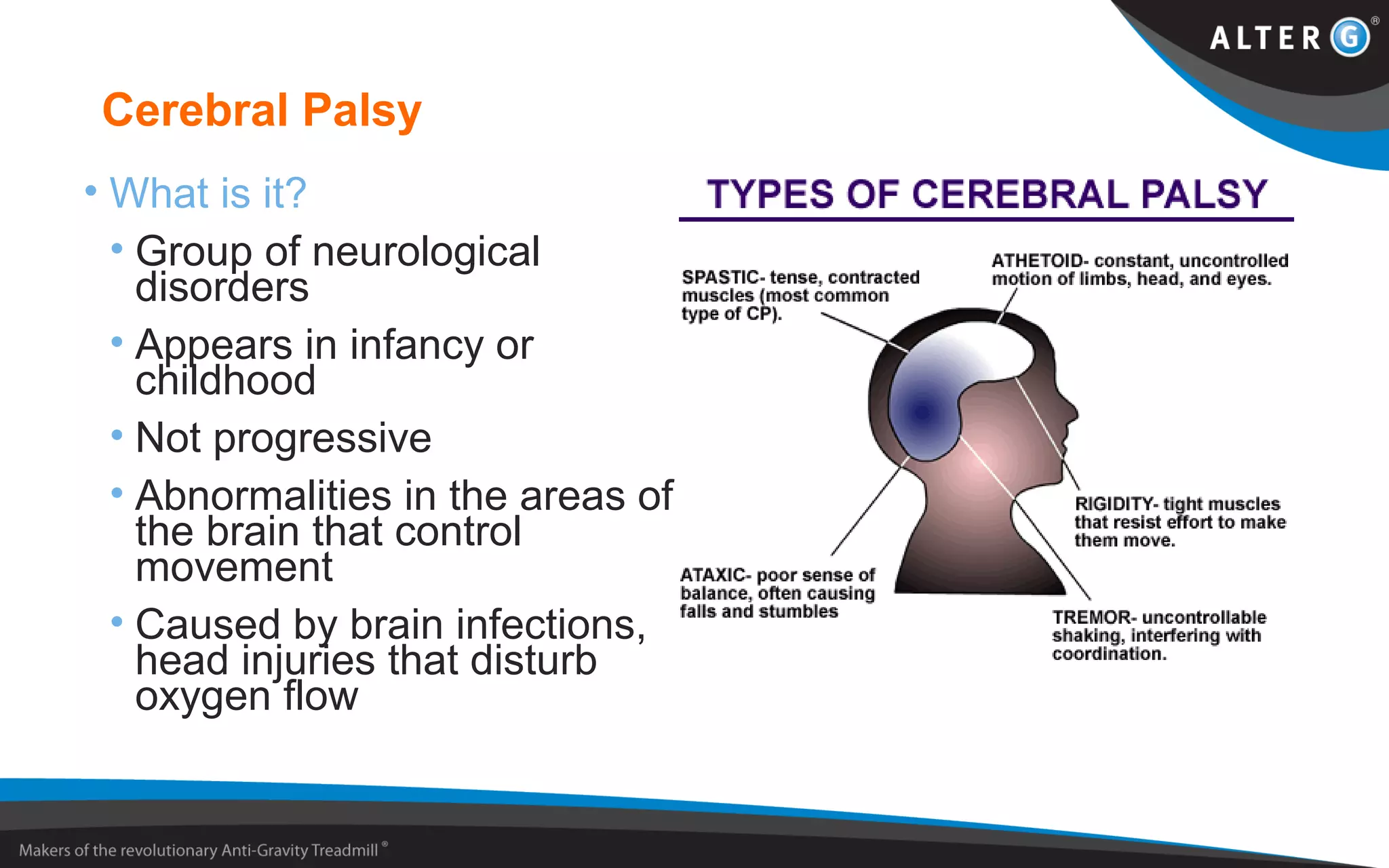

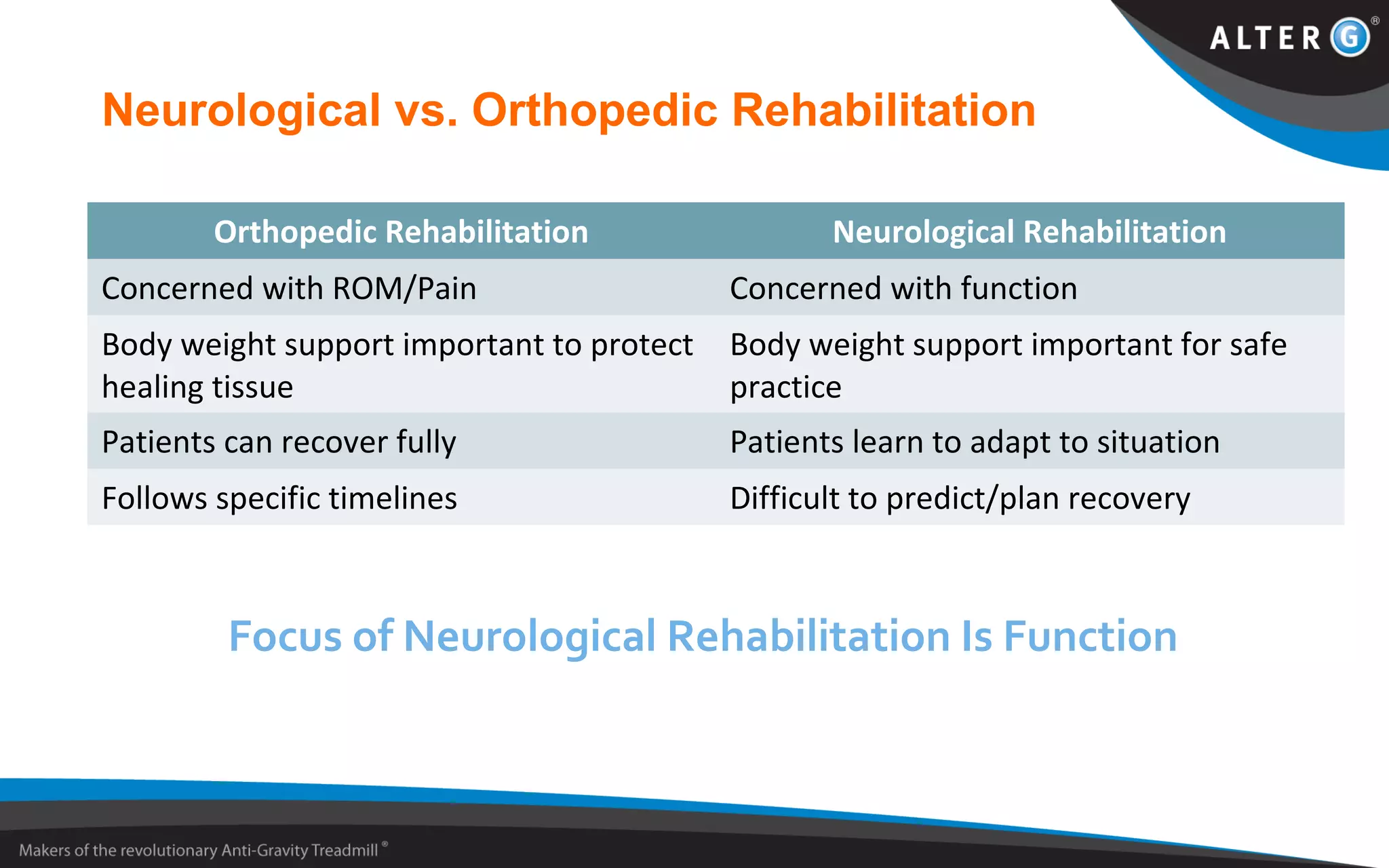


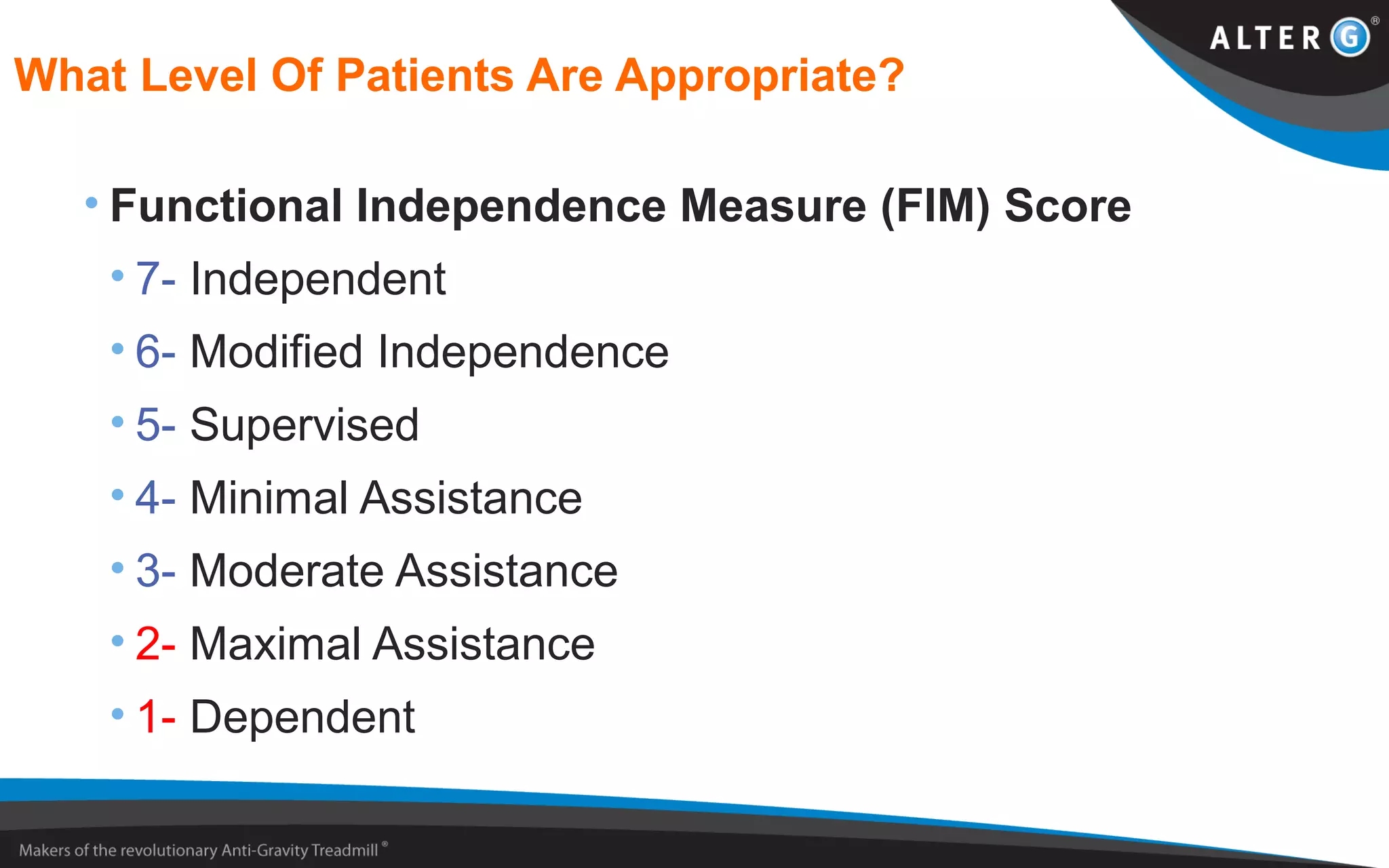
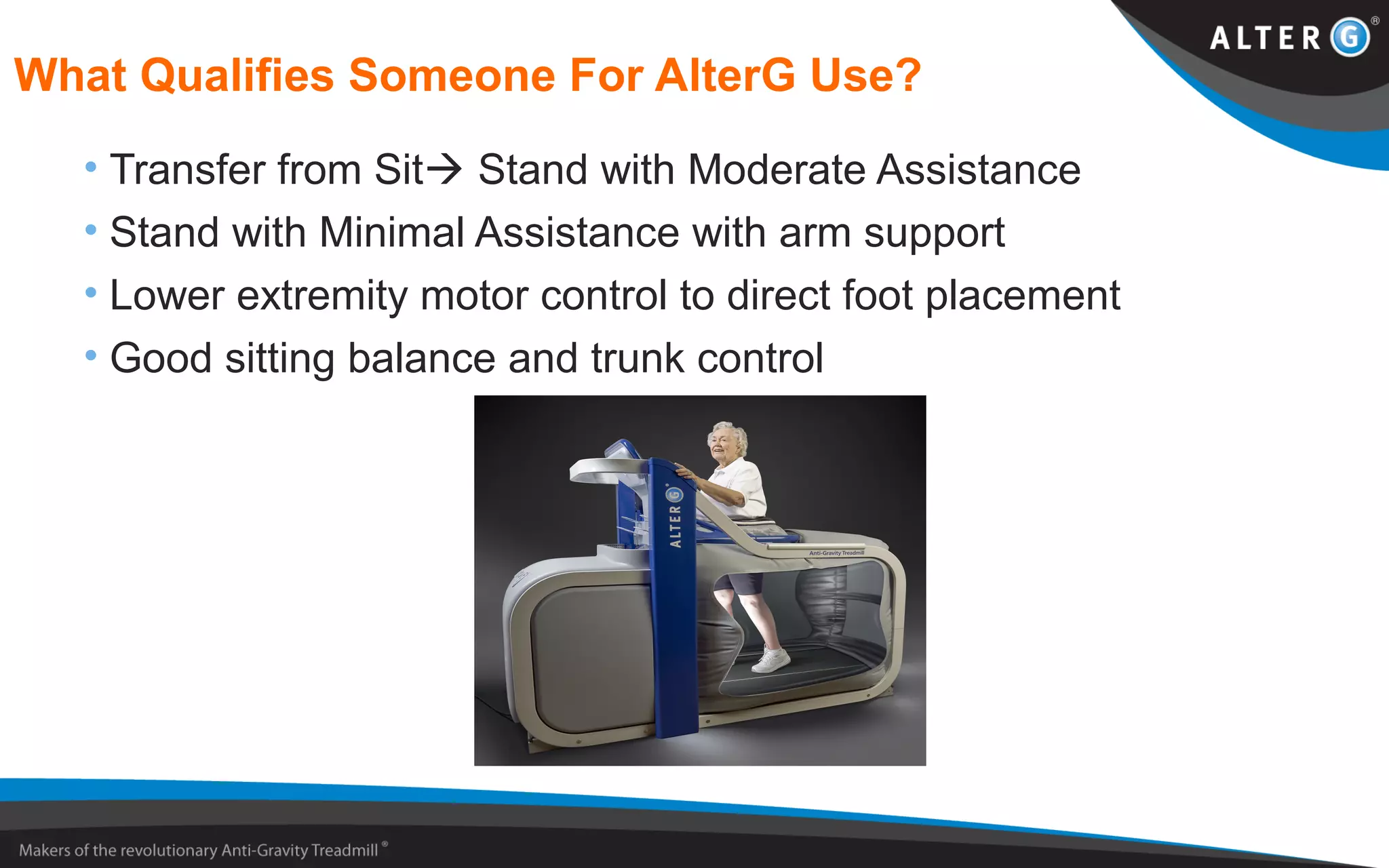


This document discusses how the AlterG anti-gravity treadmill can be used for neurological rehabilitation. It outlines common neurological disorders like Parkinson's disease, stroke, traumatic brain injury, spinal cord injury, and cerebral palsy. For each disorder, it describes symptoms and recovery timelines. Neurological rehabilitation focuses on regaining function rather than range of motion or pain relief. The AlterG allows patients to walk earlier and with less weight-bearing stress, promoting motor learning. It is appropriate for patients with moderate assistance or higher functional independence. Physical therapists can use the AlterG to assist patients in improving gait, balance, and achieving functional rehabilitation goals.


























































