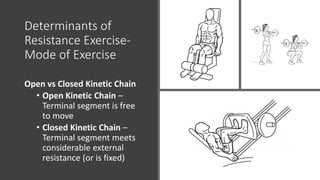
This document provides information on principles of treatment for impaired motor performance through resistance exercise. It defines key concepts like strength, power, endurance and motor control and describes how resistance training can enhance muscle performance in these areas. It discusses determinants of resistance exercise programs including frequency, intensity, time, type, mode, velocity and integration to function. Precautions and contraindications to resistance exercise are also reviewed.











































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)












