Local anaesthetics (LA)
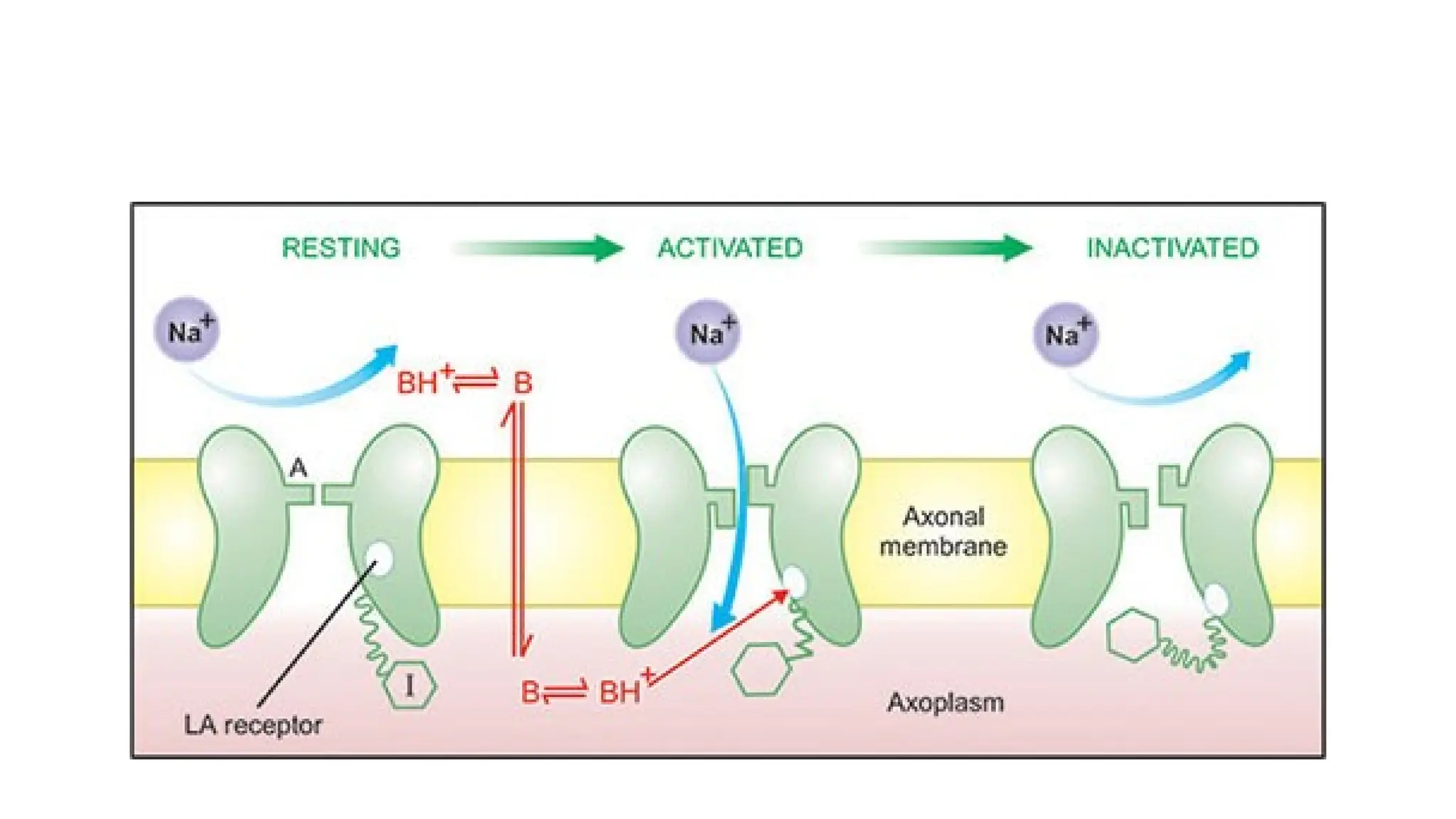
•Local anaesthetics (LA) are drugs that block nerve conduction when
applied locally to nerve tissue in appropriate concentrations.
• Their action is completely reversible.
• They act on every type of nerve fibre and can cause both sensory and
motor paralysis in the innervated area.
• Cocaine was the first agent to be isolated by Niemann in 1860.
• Unlike general anaesthetics, they neither cause a loss of
consciousness, nor need a proper maintenance of vital functions
during surgery.
PHARMACOKINETICS OF LA
•The presence of ester or amide bond in a LA molecule governs its
biotransformation and possibility of causing hypersensitivity
reactions.
• The ester-type LAs ( e.g. Tetracaine, Chloroprocaine) are usually
hydrolysed by pseudo cholinesterase or by liver esterase’s.
• Hypersensitivity reactions are common with ester type of LAs;
because they are hydrolysed to para-amino-benzoic acid (PABA) that
are known to be potential allergens.
• The amide type of LAs (Lidocaine, Bupivacaine) are degraded by
hepatic microsomes. As a result they have a longer duration of action.
7.
PHARMACOLOGICAL ACTION OFLA
• Depending on concentration attained in the plasma_. any LA can
produce systemic effects.
• CNS, autonomic ganglia, NMJ and all muscles are affected.
1. CNS:
• Local anaesthetics depress the cortical inhibitory pathway thereby
allowing unopposed activity of excitatory components.
• The central stimulation is followed by generalised CNS depression and
death may result from respiratory failure.
8.
2. CVS:
• Theprimary site of action is the myocardium- Lignocaine decreases
excitability, conduction rate and force of contraction ( quinidine like effects).
• Bupivacaine is more cardiotoxic than other LAs.
3. Blood vessels:
LAs cause hypotension which is due to sympathetic blockade. They also cause
arteriolar dilatation.
4. Smooth muscle:
LAs depress contractions in the intact bowel. They also relax vascular and
bronchial smooth muscles.
5. Local actions:
On local administration, LAs bring about reversible loss of sensation as
already discussed.
9.
ADVERSE EFFECTS OFLA
1. Allergic reactions
• The ester type of LAs are metabolised to PABA or lts derivatives, which cause
allergic reactions.
• The result is contact dermatitis, rashes and asthma.
• Amide group of LAs do not cause allergic reactions.
2.CVS
• LAs block sodium channels and depress abnormal cardiac pacemaker activity,
excitability and conduction.
• Most LAs produce hypotension.
• Bupivacaine is cardiotoxic, cause ventricular tachycardia & fibrillation.
• Lignocaine has a quinidine-like action on heart and is used in the treatment of
cardiac arrhythmia.
10.
3. Blood
• Largedoses of Prilocaine cause accumulation of its metabolite called
orthotoluidine, which oxidises haemoglobin to methaemoglobin.
• Higher levels of methaentoglobin can cause cyanosis.
• Methylene blue or ascorbic acid can be used to restore haemoglobin.
4.CNS
• At low doses, LAs cause tongue numbness, sleepiness, mild headache,
visual and auditory disturbances.
• At high dose, they cause nystagmus and muscular twitching.
11.
DRUG INTERACTIONS &PRECAUTION OF LA
• Before injecting the LA, aspirate lightly to avoid intravascular injection.
• Inject the LA slowly and take care not to exceed the maximum safe dose, especially in
children.
Propranolol ( other beta blocker) also may reduce metabolism of Lidocain & other amide Local
anaesthetic by reducing hepatic blood flow.
• Vasoconstrictor (adrenaline) containing Local anaesthetic should be I avoided for patient
with :-
• Ischemia heart disease,
• Cardiac arrhythmias,
• Thyrotoxicosis,
• Uncontrolled hypertension
• Those receiving BETA-blocker or Tricyclic arrhythmias.
12.
1. Lignocaine
• Itis the most widely used LA. It is fast and long-acting.
• It is useful for all types of blocks,
• Maximum anaesthetic effect is seen in 2-5 minutes and lasts for 30-
45 minutes.
• In contrast to other LAs, lignocaine causes drowsiness and mental
clouding.
13.
Cocaine:
• It isa benzoyl methylecgonine hydrochloride ( an ester of benzoic acid).
• It is an alkaloid extracted from the leaves of coca tree (E,ythroxylum coca).
• Pharmacological Actions
i. It stimulates CNS & causes restlessness, excitement, euphoria, tachycardia,
tachypnea, and hypertension.
ii. It also stimulates respiratory, vasomotor & vomiting centres.
iii. It has a direct toxic effect on myocardium.
iv. In small doses it causes bradycardia due to central vagal stimulation.
v. In larger dose it causes sympathetic stimulation resulting in tachycardia,
peripheral vasoconstriction, hypertension, and ventricular fibrillation.
14.
• Pharmacokinetics:
1. Cocaineundergoes slow absorption from mucous membrane due to its
vasoconstriction.
2. It gets eliminated slowly so toxic symptoms easily occur.
3. It is mostly detoxicated in the liver and a small unchanged quantity is
excreted via kidneys.
• Adverse effect
✓ Cocaine is unique among drugs of abuse.
✓ Cocaine also stimulates vagal centre bradycardia
➔
✓ Vasomotorcentre rise in BP;
➔
✓ Vomiting centre nausea & vomiting
➔
✓ Temperature regulating centre pyrexia
➔