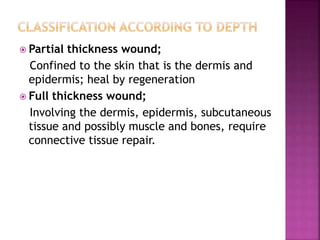
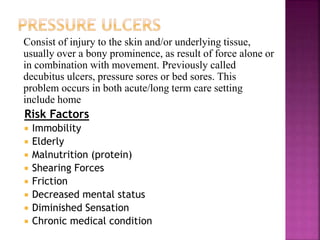
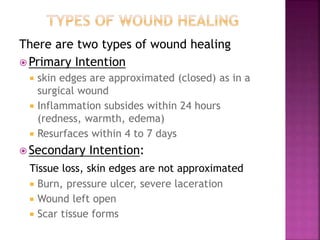
The skin is the largest organ of the body and acts as a barrier and regulator. Wounds are breaks in the skin that can be intentional from surgery or unintentional from trauma. Wounds are classified by depth and cleanliness. Pressure ulcers develop from prolonged pressure and poor positioning and are a risk for immobile patients. Wound healing involves inflammation, proliferation of new tissue, and remodeling. Dressings protect wounds and maintain a moist environment to aid healing. Infection and dehiscence are complications that can delay healing.



![ Pressure ulcer scale for healing (figure 4)
When pressure ulcer is present. Nurse note the
followings
1. Location
2. Size in centimeter(length, width, depth) beginning
with length [head to toe] and then width [side to
side]
3. Presence of undermining or sinus tract, location
described by position on the face of a clock, 12 o’
clock as the client head.
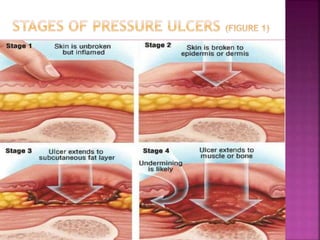
4. Stage of sore
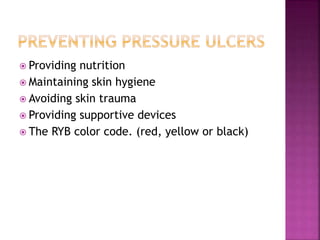
5. Color of sore. The RYB color code. (red, yellow or
black)
6. Condition of wound margin
7. Clinical signs of infection](https://image.slidesharecdn.com/uintno6skinintegrety-230926195855-2c676f72/85/uint_no_6_skin_integrety-ppt-12-320.jpg)
![Skin integrity and wound care [autosaved] (2)](https://cdn.slidesharecdn.com/ss_thumbnails/skinintegrityandwoundcareautosaved2-130319145819-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


![Skin integrity and wound care [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/skinintegrityandwoundcareautosaved-130319145813-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)







































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)











