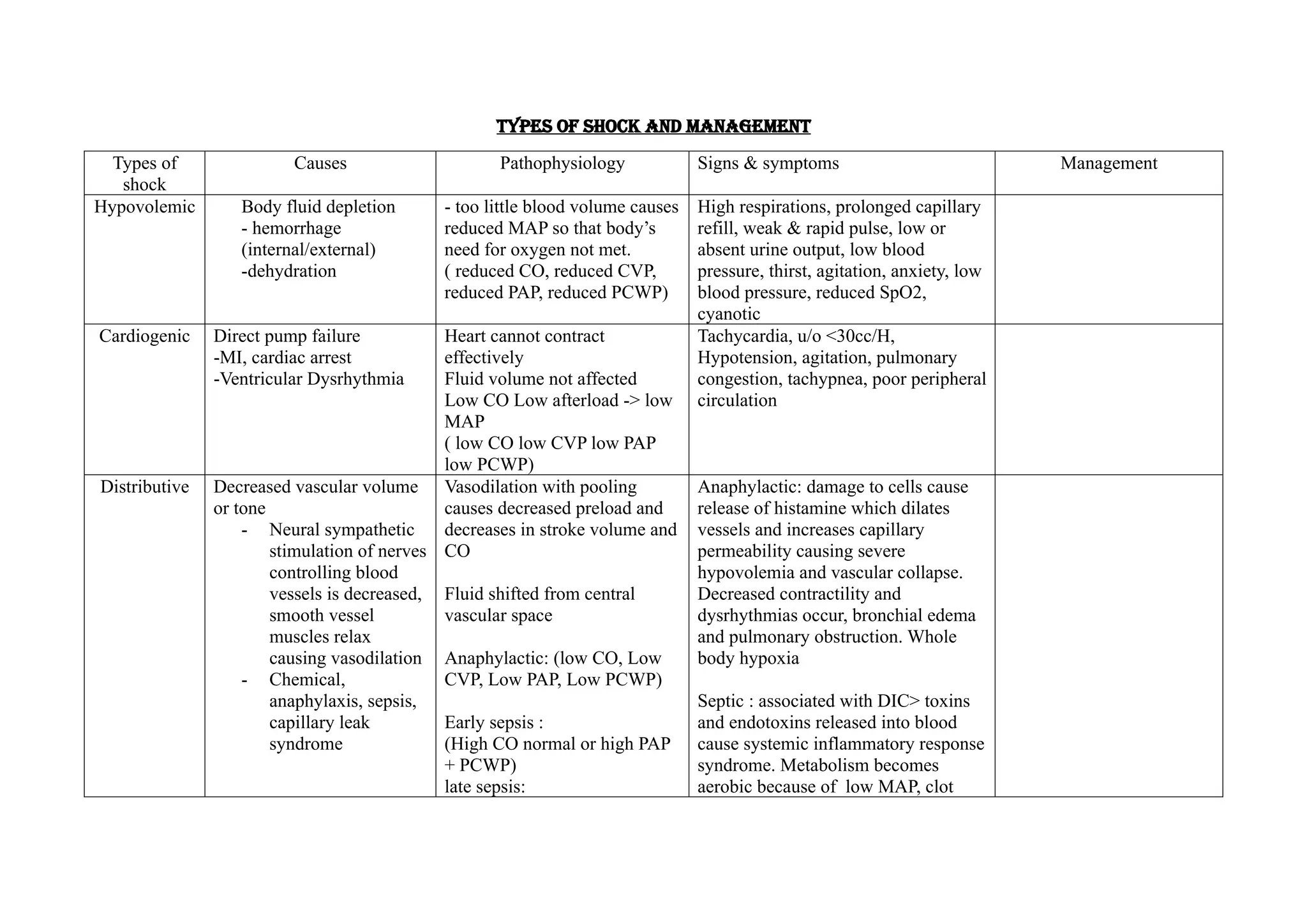
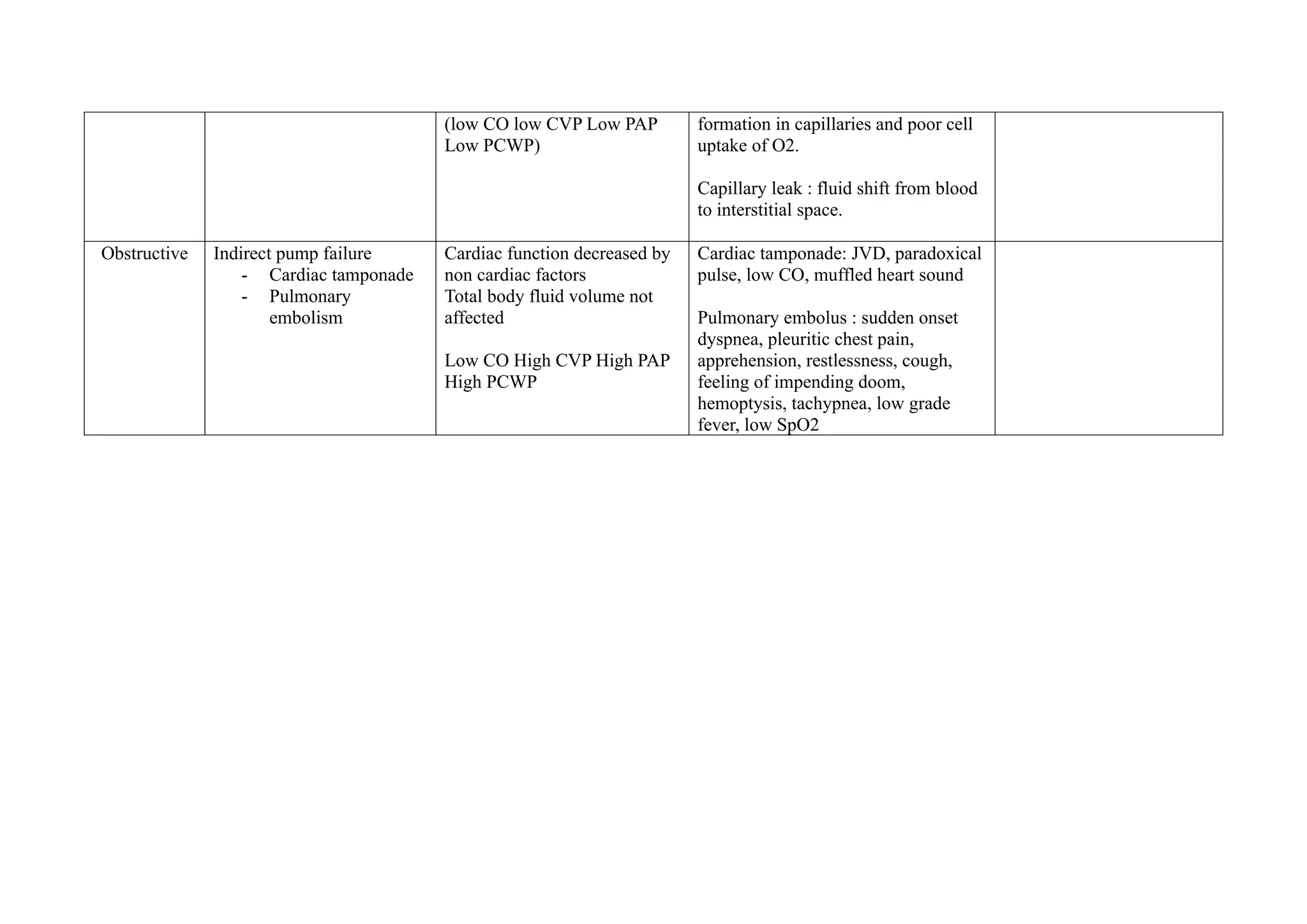
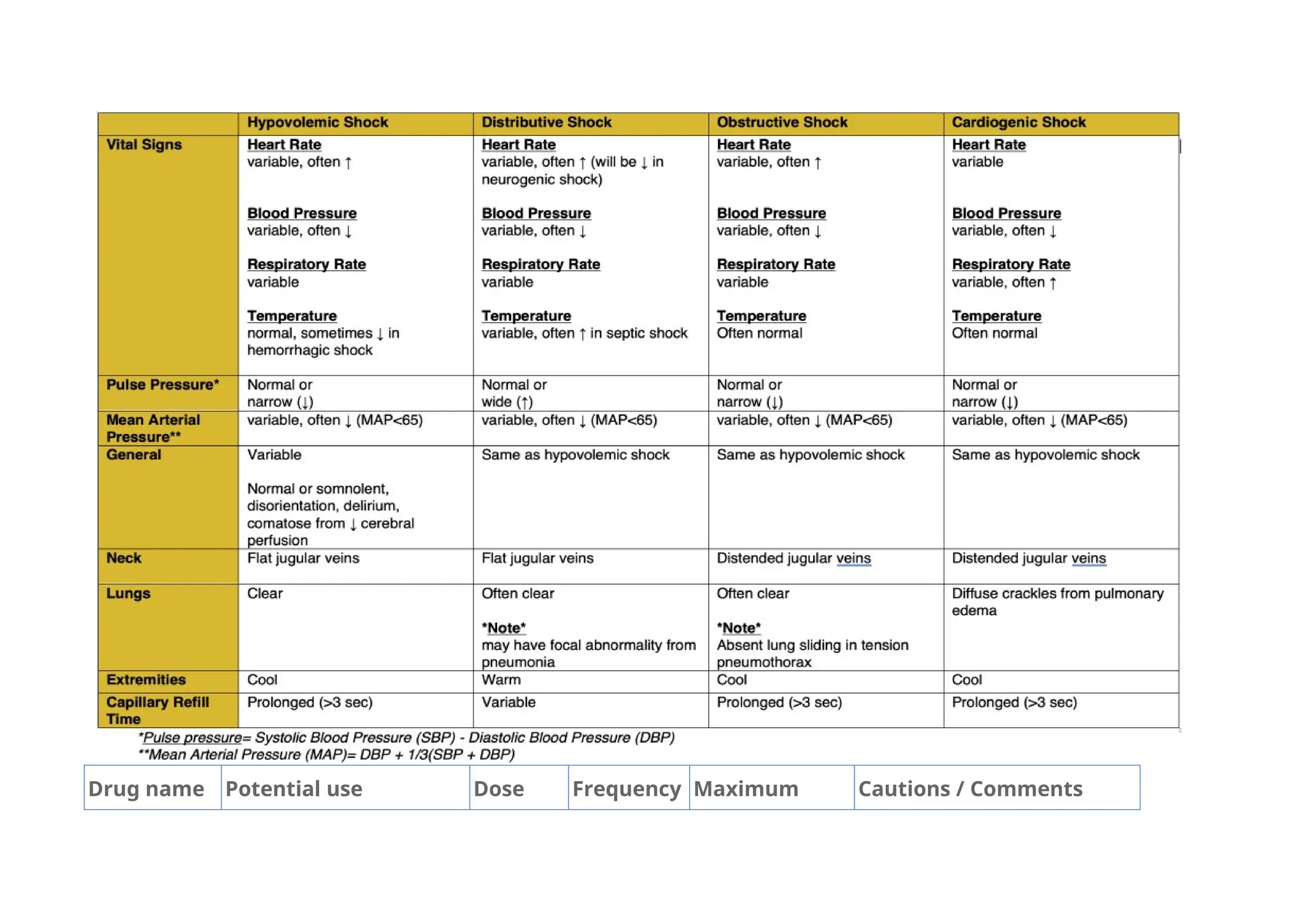
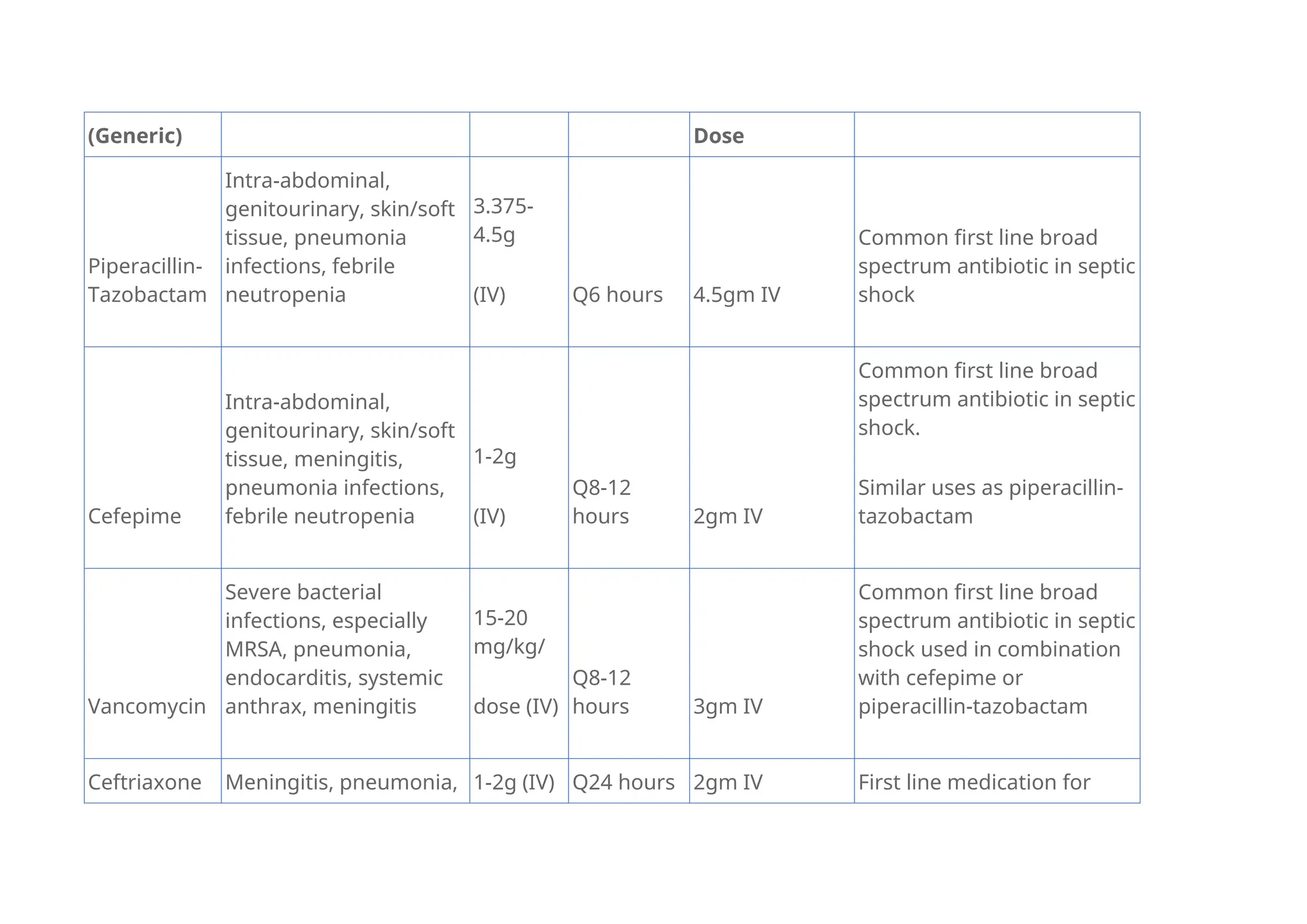
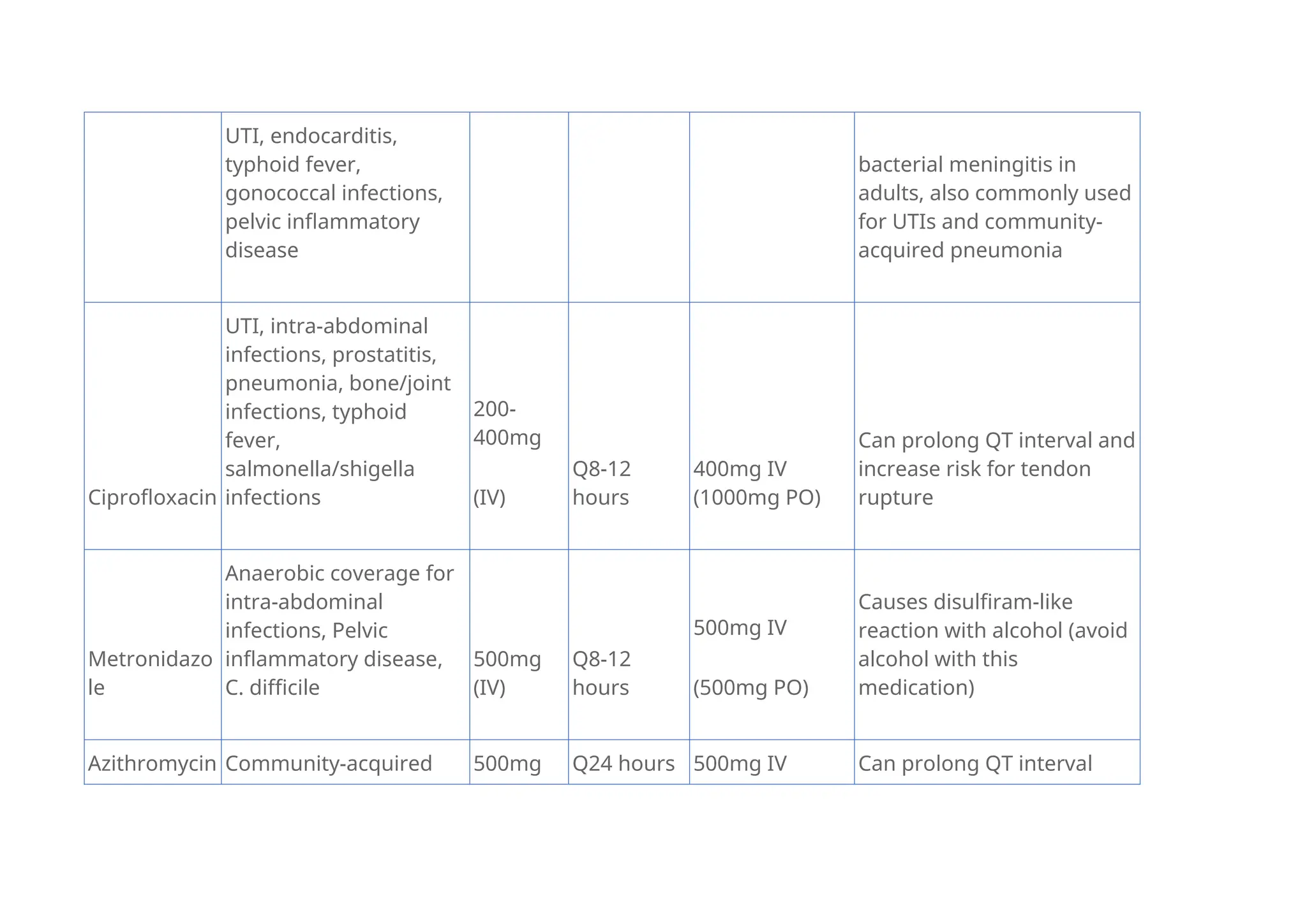
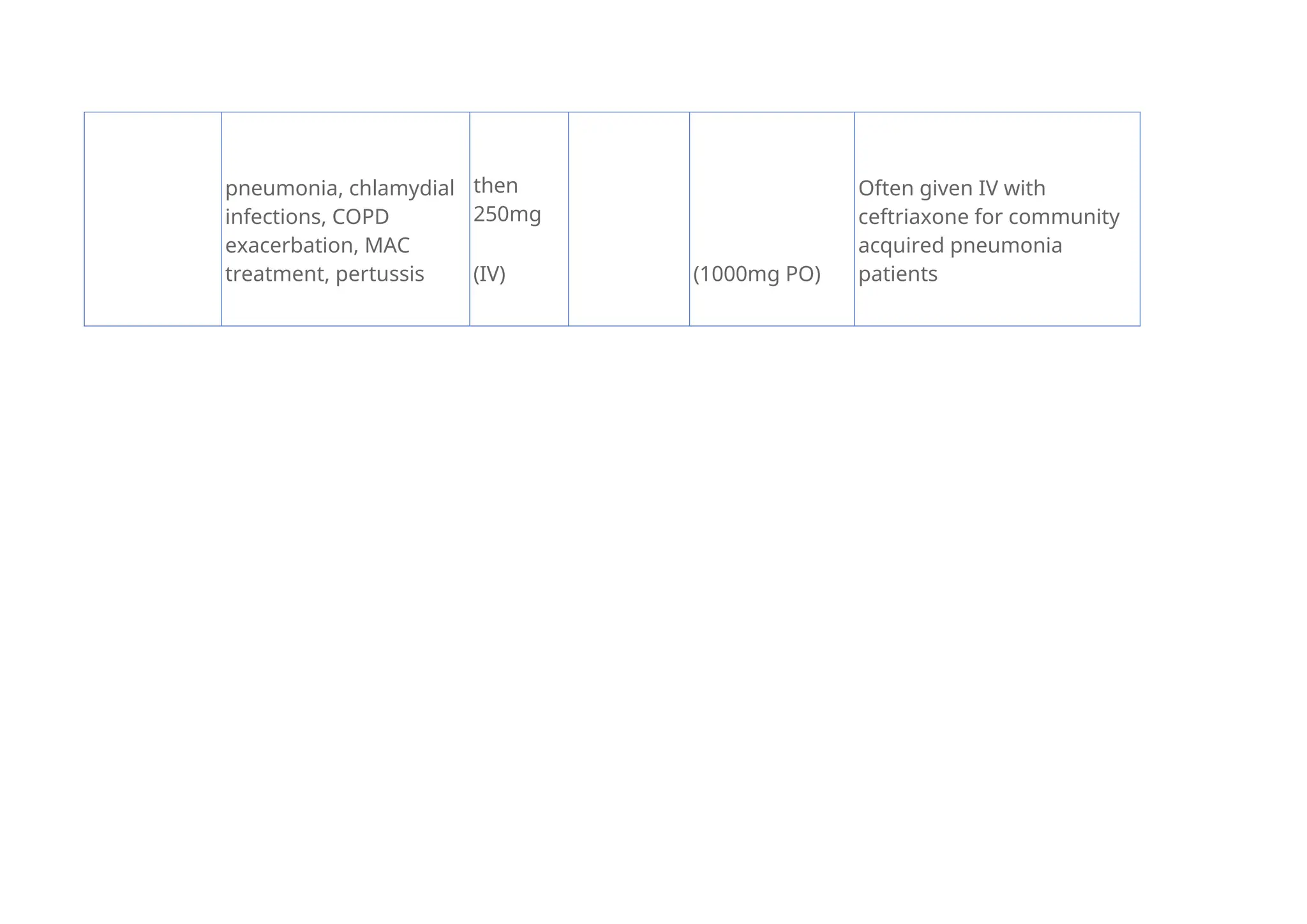
The document discusses various types of shock including hypovolemic, cardiogenic, distributive, and obstructive, detailing their causes, signs, symptoms, and management strategies. It outlines pathophysiological mechanisms such as fluid depletion, pump failure, and vessel dilation, along with crucial vital signs and clinical findings associated with each type. Additionally, the document lists antibiotics and their applications in treating infections related to septic shock, including dosage and precautions.